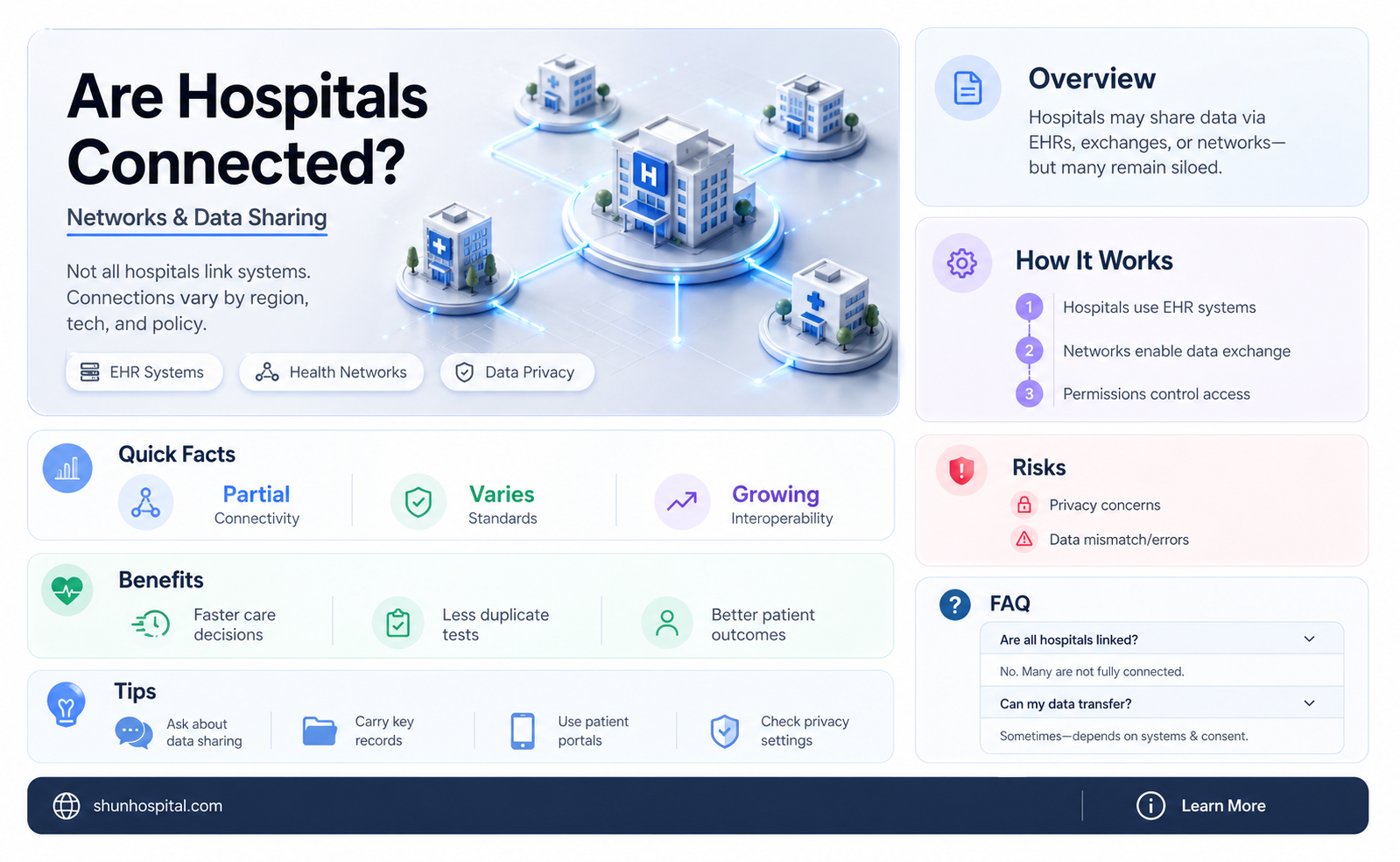
The question of whether all hospitals are connected is a multifaceted one, encompassing both physical and digital infrastructures. While hospitals are not universally linked by a single, centralized network, they often operate within interconnected systems at regional, national, or even international levels. Physically, hospitals may share resources, transfer patients, or collaborate through partnerships, especially in emergency or specialized care scenarios. Digitally, advancements in health information technology have enabled the exchange of patient data through electronic health records (EHRs) and interoperability standards, fostering better coordination among healthcare providers. However, the extent of connectivity varies widely depending on factors such as geographic location, funding, and regulatory frameworks, leaving gaps in seamless integration across all healthcare facilities.
Explore related products






What You'll Learn
- Inter-hospital Data Sharing: How patient records are exchanged between hospitals for continuity of care
- Telemedicine Networks: Use of technology to connect hospitals for remote consultations and care
- Regional Health Systems: Integration of hospitals within local or state healthcare networks
- Emergency Response Coordination: Collaboration between hospitals during crises or disasters
- Supply Chain Connectivity: Shared resources and logistics for medical supplies and equipment
![]()
Inter-hospital Data Sharing: How patient records are exchanged between hospitals for continuity of care
Hospitals are not universally connected in a seamless, standardized network, but inter-hospital data sharing is increasingly vital for patient care continuity. When a patient transitions between facilities—due to relocation, specialized treatment, or emergencies—their medical history must follow them. Without this, critical details like allergies, chronic conditions, or recent treatments can be missed, risking misdiagnosis or redundant tests. For instance, a diabetic patient’s insulin dosage or a cancer survivor’s radiation history are life-critical data points that must travel with them. This fragmented system highlights the urgency for interoperable health information exchanges (HIEs) to bridge gaps between institutions.
The technical backbone of inter-hospital data sharing relies on Health Level Seven (HL7) standards and Fast Healthcare Interoperability Resources (FHIR), which enable different electronic health record (EHR) systems to communicate. However, adoption varies widely. Large hospital networks often use proprietary systems that resist external integration, while smaller clinics may lack resources for advanced EHRs. A practical example is the Veterans Health Administration’s (VHA) seamless record-sharing across its facilities, contrasting with the patchwork access in rural or privately owned hospitals. To implement effective sharing, hospitals must prioritize compatibility and invest in infrastructure, even if it means phasing out legacy systems.
Privacy and security concerns are paramount in data exchange. The Health Insurance Portability and Accountability Act (HIPAA) sets strict guidelines for patient data protection, but breaches remain a risk. Encryption, role-based access controls, and audit trails are essential safeguards. For instance, a patient’s record should only be accessible to authorized providers involved in their care, not the entire network. Hospitals must also educate staff on phishing and social engineering threats, as human error is a leading cause of data leaks. Balancing accessibility with security is a delicate but non-negotiable aspect of inter-hospital sharing.
Despite challenges, successful models exist. The Indiana Health Information Exchange (IHIE) connects over 100 hospitals, enabling real-time access to records for 12 million patients. This has reduced duplicate testing by 20% and improved emergency response times. Similarly, Estonia’s nationwide EHR system allows any provider to access a patient’s full history with consent, setting a global benchmark. These examples demonstrate that with political will, investment, and collaboration, inter-hospital data sharing can become the norm rather than the exception. The takeaway is clear: fragmented systems harm patients, but integrated networks save lives.
Inmate Hospital Visits: Procedures, Security, and Patient Care Explained
You may want to see also
Explore related products






![]()
Telemedicine Networks: Use of technology to connect hospitals for remote consultations and care
Hospitals are not universally interconnected, but telemedicine networks are bridging this gap by leveraging technology to facilitate remote consultations and collaborative care. These networks enable healthcare providers in different facilities to share patient data, conduct virtual consultations, and coordinate treatment plans seamlessly. For instance, platforms like Teladoc and Amwell connect patients with specialists across various hospitals, ensuring timely access to expertise regardless of geographic barriers. This integration is particularly critical in rural areas, where local hospitals often lack specialized resources.
Implementing telemedicine networks requires a structured approach. First, hospitals must invest in interoperable electronic health record (EHR) systems to ensure data exchange compliance with standards like HL7 FHIR. Second, secure communication tools, such as HIPAA-compliant video conferencing software, are essential for protecting patient privacy during remote consultations. Third, training staff to use these technologies effectively is crucial; for example, nurses and physicians should be proficient in navigating telehealth platforms to avoid delays in care delivery. Finally, establishing clear protocols for cross-hospital collaboration, such as defining roles in multidisciplinary case reviews, ensures efficient workflow integration.
The benefits of telemedicine networks extend beyond convenience. A study published in the *Journal of the American Medical Informatics Association* found that remote consultations reduced patient wait times by an average of 40% and decreased hospital readmission rates by 20%. For chronic disease management, platforms like Philips’ eCareCoordinator allow hospitals to monitor patients remotely, adjusting treatment plans in real time. For instance, a diabetic patient’s glucose levels can be tracked daily, with alerts sent to both the patient’s local clinic and a specialized endocrinologist at a connected urban hospital, enabling proactive interventions.
Despite their advantages, telemedicine networks face challenges. One significant hurdle is the digital divide, where underfunded hospitals lack the infrastructure to support advanced telehealth technologies. Additionally, licensing restrictions often limit physicians’ ability to practice across state lines, fragmenting care coordination. To address these issues, policymakers must streamline regulations and allocate funding for technology upgrades. Hospitals can also partner with telehealth providers to share resources, as seen in the Mayo Clinic’s collaboration with rural hospitals to extend specialist access via their telemedicine network.
In conclusion, while not all hospitals are connected, telemedicine networks offer a viable solution to enhance collaboration and improve patient outcomes. By adopting interoperable systems, prioritizing security, and fostering cross-institutional partnerships, hospitals can overcome traditional barriers to care. As technology advances, these networks will become increasingly indispensable, transforming the healthcare landscape into a more integrated and patient-centric ecosystem.
Hospital Workers: Coronavirus Risk and Protection
You may want to see also
Explore related products





![]()
Regional Health Systems: Integration of hospitals within local or state healthcare networks
Hospitals within a region are increasingly interconnected, forming networks that streamline patient care, reduce costs, and improve outcomes. This integration, often facilitated by regional health systems, involves sharing resources, data, and expertise across local or state healthcare networks. For instance, in California, the Sutter Health network connects 24 hospitals, enabling seamless patient transfers, shared electronic health records (EHRs), and coordinated specialty care. Such systems ensure that a patient admitted to a rural hospital can access the same advanced diagnostics and treatment plans available in urban centers, bridging gaps in care quality.
To integrate hospitals effectively, regional health systems must prioritize interoperability of EHR systems. This requires standardized data formats and secure platforms for information exchange. For example, the Indiana Health Information Exchange (IHIE) connects over 100 hospitals, allowing providers to access patient histories across facilities. However, achieving this level of connectivity demands significant investment in technology and training. Hospitals must also navigate privacy regulations like HIPAA, ensuring patient data remains protected while being shared. Practical steps include conducting interoperability audits, investing in compatible software, and fostering collaboration among IT teams.
A persuasive argument for regional integration lies in its ability to address healthcare disparities. By pooling resources, hospitals in underserved areas can offer services like telemedicine, mobile clinics, and preventive care programs. For instance, the University of Vermont Health Network extends its reach to rural communities, providing virtual consultations and chronic disease management. This model reduces the burden on patients who would otherwise travel long distances for care. Policymakers and hospital administrators should advocate for funding and policies that support such initiatives, ensuring equitable access to healthcare across regions.
Comparatively, integrated regional systems outperform fragmented ones in managing public health crises. During the COVID-19 pandemic, networks like New York’s Northwell Health demonstrated the value of centralized resource allocation and data sharing. Hospitals within the network coordinated bed availability, ventilator distribution, and staffing, minimizing overwhelm. In contrast, isolated facilities often struggled with shortages and delayed responses. This highlights the need for proactive integration, not just for routine care but also for emergency preparedness. Hospitals should establish crisis protocols within their networks, including shared supply chains and communication channels.
Finally, successful regional integration requires a cultural shift toward collaboration. Hospitals must move beyond competition and embrace shared goals, such as reducing readmissions and improving population health. For example, the Mayo Clinic Care Network partners with hospitals nationwide, offering access to its expertise while allowing members to retain autonomy. This model fosters trust and mutual benefit, key to long-term success. Hospitals can start by forming regional consortia, identifying shared challenges, and piloting joint initiatives. Over time, these partnerships can evolve into robust, integrated systems that transform healthcare delivery.
Santa Fe, NM: Hospitals and Healthcare Options
You may want to see also
Explore related products




![]()
Emergency Response Coordination: Collaboration between hospitals during crises or disasters
Effective emergency response coordination hinges on seamless collaboration between hospitals, yet the reality of interconnectedness varies widely. While urban hospitals often share resources through regional health networks, rural facilities may operate in isolation due to geographical or technological barriers. For instance, during Hurricane Katrina, hospitals in New Orleans faced communication breakdowns, highlighting the fragility of ad-hoc connections. This disparity underscores the need for standardized protocols and robust infrastructure to ensure all hospitals, regardless of location, can collaborate during crises.
To enhance collaboration, hospitals must adopt interoperable communication systems. During the 2013 Boston Marathon bombing, hospitals used a shared electronic health record (EHR) system to track patient flow and resource allocation, demonstrating the power of connectivity. Implementing such systems requires investment in technology and training, but the payoff is immense: real-time data sharing can reduce redundancy and improve patient outcomes. For example, a regional health information exchange (HIE) can enable hospitals to access patient histories instantly, streamlining triage and treatment.
A critical yet overlooked aspect of hospital collaboration is resource pooling. During the COVID-19 pandemic, New York City hospitals coordinated ventilator sharing and patient transfers, illustrating the life-saving potential of collective action. Hospitals should establish mutual aid agreements in advance, outlining protocols for equipment, personnel, and bed sharing. For instance, a rural hospital could partner with a larger urban facility to secure access to specialized care during disasters. Such agreements must include clear triggers for activation, such as reaching 80% ICU capacity, to ensure timely response.
Despite technological advancements, human factors remain pivotal in emergency coordination. Regular drills and cross-training exercises can foster trust and familiarity between hospital teams. For example, a multi-hospital simulation of a mass casualty event can reveal communication gaps and refine roles. Additionally, designating a regional incident commander during crises can prevent duplication of efforts and ensure unified decision-making. Hospitals must also prioritize staff mental health, as burnout can hinder collaboration—a lesson learned from the Ebola outbreak, where overworked healthcare workers struggled to coordinate effectively.
In conclusion, while not all hospitals are currently connected, the framework for collaboration exists and must be strengthened. By investing in interoperable systems, formalizing resource-sharing agreements, and prioritizing human preparedness, hospitals can transform isolated responses into coordinated lifesaving efforts. The goal is not just connectivity but resilience—ensuring that when disaster strikes, no hospital stands alone.
Tommy Lasorda: Hospital Stay and Health Update
You may want to see also
Explore related products






![]()
Supply Chain Connectivity: Shared resources and logistics for medical supplies and equipment
Hospitals, despite their individual operations, are increasingly interconnected through shared supply chains, a necessity amplified by crises like the COVID-19 pandemic. This connectivity isn’t just about sharing excess supplies; it’s a strategic framework where resources like ventilators, PPE, and critical medications are pooled and redistributed based on real-time demand. For instance, during the pandemic, New York City’s hospitals coordinated through a regional health network to transfer ventilators from facilities with surplus to those on the brink of shortage, saving countless lives. Such examples highlight how shared logistics can transform isolated entities into a resilient healthcare ecosystem.
Implementing a shared supply chain requires a structured approach. First, hospitals must map their inventory in a centralized database, detailing stock levels of essential items like epinephrine auto-injectors (EpiPens), saline solution, or N95 masks. Second, establish a regional hub-and-spoke model where larger hospitals act as distribution centers for smaller facilities. Third, adopt predictive analytics to forecast demand spikes, ensuring critical supplies like pediatric dosages of antibiotics (e.g., 50 mg/kg of amoxicillin for children under 12) are available before shortages occur. Caution: Without standardized protocols, this system risks inefficiencies, such as mismatched supply-demand or delayed deliveries.
The benefits of shared logistics extend beyond crisis management. By consolidating procurement, hospitals can negotiate bulk discounts on high-cost equipment like MRI machines or chemotherapy drugs, reducing expenses by up to 20%. Additionally, shared transportation networks minimize carbon footprints—a single delivery truck servicing multiple facilities cuts emissions compared to individual shipments. For example, a Midwest hospital network reduced its logistics costs by $2 million annually by pooling deliveries of sterile gloves and surgical kits. This model also ensures rural hospitals, often underserved, receive timely supplies, bridging the urban-rural healthcare divide.
However, challenges persist. Data privacy concerns arise when hospitals share inventory details, requiring robust cybersecurity measures. Legal agreements must clearly outline liability in case of supply chain failures, such as delayed shipments of temperature-sensitive vaccines. Moreover, cultural resistance to collaboration among competing institutions can hinder progress. To overcome this, policymakers can incentivize participation through grants or regulatory mandates, while hospitals can start with pilot programs focusing on non-critical supplies like bandages or IV fluids to build trust.
In conclusion, shared resources and logistics aren’t just a trend but a necessity for modern healthcare. By leveraging technology, fostering collaboration, and addressing challenges head-on, hospitals can create a supply chain that’s not only efficient but also equitable. The takeaway is clear: connectivity isn’t optional—it’s the backbone of a healthcare system prepared for both everyday demands and unforeseen emergencies.
Hospital ID: What's the Purpose?
You may want to see also
Frequently asked questions
No, not all hospitals are connected through a shared network or system. While some hospitals within the same healthcare system or region may share electronic health records (EHRs) or other systems, many operate independently with their own infrastructure.
No, hospitals do not automatically share patient information with each other. Sharing is typically limited to cases where patients provide consent, or when required by law, such as in emergencies. Interoperability between systems is improving but is not universal.
No, hospitals are often independent entities or part of different healthcare organizations, networks, or systems. While some may collaborate or affiliate, they generally operate under separate management and governance structures.