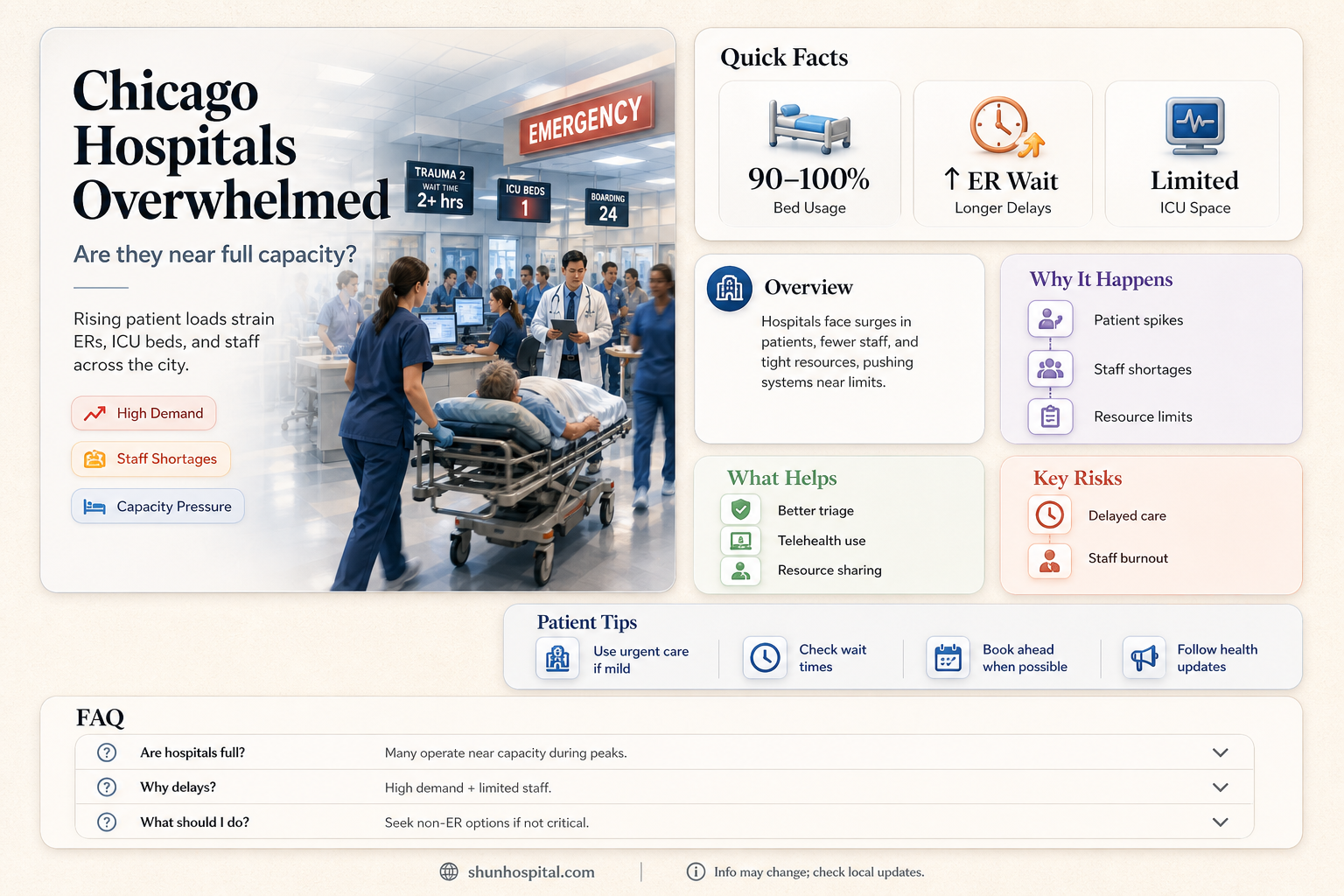
Chicago's hospitals are facing increasing strain as patient volumes rise, prompting concerns about whether they are operating at or near capacity. Factors such as seasonal illnesses, including respiratory viruses like RSV and influenza, coupled with the ongoing impact of COVID-19, have contributed to heightened demand for medical services. Emergency departments and intensive care units are particularly stressed, with reports of longer wait times and limited bed availability. Healthcare providers are working diligently to manage the influx, but the situation underscores the need for continued public health measures and community awareness to alleviate pressure on the healthcare system.
Explore related products






What You'll Learn
![]()
Current bed occupancy rates in Chicago hospitals
Chicago's hospitals are currently experiencing a delicate balance in bed occupancy rates, with fluctuations influenced by seasonal illnesses, staffing challenges, and community health trends. As of recent data, the average bed occupancy rate hovers around 75-80%, a figure that reflects both the resilience of healthcare systems and the ongoing strain they face. This range is critical because it leaves a buffer for emergency admissions, such as surges in flu cases or trauma incidents, while also indicating that hospitals are operating near their functional limits. For instance, during the winter months, when respiratory illnesses peak, occupancy rates can spike to 90% or higher, pushing facilities to implement contingency plans like diverting patients to less-burdened hospitals.
Analyzing these rates reveals a nuanced picture of healthcare demand. Hospitals in densely populated areas like the Loop or South Side often report higher occupancy due to greater patient volumes, while suburban facilities may have slightly lower rates. Pediatric wards, for example, see seasonal spikes during back-to-school periods, with occupancy rates climbing as high as 85% due to viral outbreaks. In contrast, intensive care units (ICUs) maintain lower baseline occupancy, typically around 60-70%, to ensure capacity for critical cases, but these numbers can surge during crises like the COVID-19 pandemic, when ICUs reached near-full capacity.
For those navigating Chicago’s healthcare system, understanding these trends is practical. Patients with non-urgent needs can benefit from scheduling appointments during off-peak times, such as early mornings or weekdays, to avoid longer wait times. Additionally, knowing which hospitals have lower occupancy rates can expedite care during emergencies. Apps like Zocdoc or hospital-specific portals often provide real-time updates on wait times, offering a strategic edge for informed decision-making.
A comparative look at Chicago’s occupancy rates versus national averages highlights both challenges and successes. While the city’s 75-80% occupancy aligns with the national average, it underscores the need for continued investment in infrastructure and staffing. Hospitals in Chicago have responded by expanding telemedicine services, which reduce in-person visits by up to 30% for minor ailments, thereby easing bed demand. However, this approach is not a panacea, as certain conditions still require physical hospitalization, emphasizing the importance of maintaining adequate bed capacity.
In conclusion, Chicago’s hospital bed occupancy rates are a dynamic metric shaped by seasonal, demographic, and operational factors. While current rates suggest a manageable situation, they also signal the need for proactive measures to prevent overcapacity. Patients, policymakers, and healthcare providers must collaborate to optimize resource allocation, ensuring that Chicago’s hospitals remain equipped to meet the community’s needs, both in routine times and during unforeseen surges.
Richmond VA Hospital's Age: A Historical Overview of Its Establishment
You may want to see also
Explore related products






![]()
Impact of COVID-19 on hospital capacity
The COVID-19 pandemic has placed unprecedented strain on healthcare systems worldwide, and Chicago’s hospitals have been no exception. During peak surges, particularly in late 2020 and early 2021, many facilities operated at or near capacity, with intensive care units (ICUs) often overwhelmed. For instance, in November 2020, some hospitals reported ICU occupancy rates exceeding 90%, forcing them to divert patients to other facilities. This crisis highlighted the fragility of hospital capacity when faced with a rapid influx of critically ill patients.
One critical factor in managing capacity has been the ability to scale resources dynamically. Hospitals implemented surge plans, converting non-ICU spaces into makeshift critical care units and postponing elective surgeries to free up beds and staff. However, these measures were not without trade-offs. Delayed procedures led to a backlog of patients needing urgent but non-COVID-related care, creating a secondary crisis in healthcare access. Staffing shortages further exacerbated the issue, as healthcare workers faced burnout and illness, reducing the effective capacity of hospitals even when physical beds were available.
The pandemic also exposed disparities in hospital capacity across Chicago’s neighborhoods. Hospitals in underserved areas, often with higher COVID-19 infection rates, were disproportionately affected. These facilities, already operating with limited resources, struggled to meet the demand, while hospitals in more affluent areas had greater flexibility to expand capacity. This imbalance underscored the need for equitable resource distribution and targeted support for vulnerable communities during public health emergencies.
To mitigate future capacity crises, Chicago hospitals have adopted long-term strategies. Telehealth services expanded significantly, reducing the burden on physical facilities for non-critical cases. Regional collaboration among hospitals improved patient transfers and resource sharing during surges. Additionally, investments in data analytics allowed for real-time monitoring of bed availability and staffing needs, enabling more proactive decision-making. While these measures cannot eliminate the risk of capacity strain, they provide a framework for resilience in the face of ongoing and future challenges.
Finding the Snack Bar at Butler Hospital: A Quick Guide
You may want to see also
Explore related products






![]()
Staffing shortages affecting patient care
Chicago hospitals are grappling with a crisis that extends beyond bed capacity: a severe staffing shortage that directly impacts patient care. Nurses, physicians, and support staff are stretched thin, often working overtime and double shifts to meet demand. This exhaustion leads to higher rates of medical errors, delayed treatments, and reduced quality of care. For instance, a study by the Illinois Hospital Association found that 78% of hospitals reported staffing shortages in 2023, with critical care units particularly affected. When a single nurse is responsible for 10 or more patients instead of the recommended 4–6, the risk of overlooked symptoms or medication errors skyrockets.
Consider the ripple effect of these shortages on patient outcomes. A delayed response to a patient’s deteriorating condition, due to overburdened staff, can mean the difference between recovery and long-term complications. For example, in emergency departments, wait times have increased by 20–30% in some Chicago hospitals, forcing patients with non-life-threatening conditions to wait hours for care. This not only frustrates patients but also diverts attention from those with critical needs. Pediatric and geriatric care units face unique challenges, as specialized staff shortages mean vulnerable populations receive less attentive care, potentially worsening chronic conditions or delaying developmental interventions.
To address this, hospitals must rethink their staffing strategies. One practical step is to invest in cross-training programs, enabling nurses and technicians to handle multiple roles during peak demand. For instance, training medical assistants to perform basic triage tasks can free up registered nurses for more complex duties. Additionally, offering competitive compensation packages, including retention bonuses and mental health support, can reduce turnover. Hospitals could also partner with local nursing schools to create pipelines for new graduates, providing mentorship and on-the-job training to ease the transition into high-stress environments.
However, these solutions come with cautions. Cross-training, while effective, risks diluting expertise if not implemented thoughtfully. Hospitals must ensure staff are only assigned tasks within their competency levels to avoid errors. Similarly, reliance on travel nurses, while a quick fix, can disrupt team dynamics and increase costs. A balanced approach, combining short-term staffing solutions with long-term workforce development, is essential. Ultimately, addressing staffing shortages requires systemic change, not just Band-Aid solutions, to ensure Chicago’s hospitals can deliver safe, effective care without compromising their workforce’s well-being.
Poisonous Berries and DCF: When Hospitals Must Report Child Ingestion
You may want to see also
Explore related products






![]()
Emergency room wait times and delays
Chicago's emergency departments are experiencing a perfect storm of challenges, leading to prolonged wait times and delayed care. The city's hospitals, particularly those in underserved areas, are grappling with a surge in patient volume, staffing shortages, and limited resources. This convergence of factors has created a critical situation where patients often face hours-long waits for treatment, even in life-threatening situations.
Consider the case of a 65-year-old patient with chest pain, a symptom that warrants immediate attention. Upon arrival at a Chicago ER, they may be triaged and assigned a priority level, but the reality is that they could still wait upwards of 4-6 hours before being seen by a physician. This delay is not due to negligence but rather a systemic issue. Hospitals are operating at or near capacity, with occupancy rates frequently exceeding 90%. As a result, emergency departments become bottlenecks, struggling to accommodate the influx of patients while managing limited treatment spaces and overworked staff.
To mitigate these delays, patients can take proactive steps. First, understand the triage process: ERs prioritize cases based on severity, not arrival time. Conditions like severe bleeding, difficulty breathing, or suspected stroke are immediate priorities. For less critical issues, consider urgent care centers or telemedicine services, which can provide faster, more efficient care. For instance, a patient with a minor fracture or a urinary tract infection might receive treatment within an hour at an urgent care facility, compared to a potential 3-4 hour wait at an ER.
However, for those with severe or complex conditions, the ER remains the best option, despite the delays. In such cases, patients or their caregivers should advocate for themselves. Communicate symptoms clearly and ask about expected wait times. If the condition worsens while waiting, notify the triage nurse immediately. Hospitals are increasingly implementing digital tools to manage patient flow, such as online check-ins and real-time wait time updates, which can help set expectations and reduce anxiety.
The impact of these delays extends beyond individual patients. Longer wait times contribute to increased stress on healthcare workers, higher rates of patients leaving without being seen, and potentially worse health outcomes. Addressing this issue requires systemic changes, including increased funding for healthcare infrastructure, expanded staffing, and better integration of community health resources. Until then, patients must navigate this challenging landscape with awareness and strategic decision-making to ensure they receive timely and effective care.
Boston Children's Hospital: Unveiling Its Prestigious National Ranking
You may want to see also
Explore related products



$13.99 $15.9



![]()
Strategies to manage hospital overflow
Chicago hospitals, like many urban healthcare systems, often face periods of high patient volume that test their capacity limits. During surges, whether due to seasonal illnesses, pandemics, or mass casualty events, managing overflow becomes critical to maintaining patient care quality. One effective strategy involves expanding physical space by converting non-clinical areas into temporary treatment zones. For instance, conference rooms, cafeterias, or even parking garages can be repurposed with portable medical equipment and privacy screens. This approach, while not ideal, provides immediate relief to overcrowded emergency departments and inpatient wards. However, it requires careful planning to ensure infection control, patient safety, and staff accessibility.
Another key strategy is optimizing patient flow through streamlined triage and discharge processes. Implementing protocols like "fast-track" triage for low-acuity cases can reduce wait times and free up resources for critical patients. Similarly, accelerating discharges by coordinating with pharmacies, transportation services, and follow-up care providers minimizes bed occupancy. Hospitals can also leverage technology, such as electronic health records (EHRs) with real-time bed tracking, to identify available spaces promptly. These measures, when executed efficiently, create a continuous flow of patients in and out of the facility, preventing bottlenecks.
Collaborating with external partners is a third critical strategy. Chicago hospitals can form regional coalitions to share resources, including staff, equipment, and patient transfers. For example, during a surge, a hospital at capacity might transfer stable patients to nearby facilities with available beds. Additionally, partnering with urgent care centers, telehealth providers, and mobile medical units can offload non-critical cases, reducing the burden on emergency departments. Such partnerships require clear communication channels and predefined agreements to ensure seamless coordination during crises.
Finally, preventive measures play a vital role in managing overflow before it occurs. Public health campaigns promoting vaccination, hygiene, and early medical intervention can reduce the incidence of severe illnesses that lead to hospitalization. For instance, during flu season, widespread vaccination drives targeting high-risk groups (e.g., seniors, immunocompromised individuals) can lower admission rates. Similarly, educating the public about appropriate healthcare utilization—such as using telehealth for minor ailments—can prevent unnecessary hospital visits. By addressing demand at its source, hospitals can mitigate overflow risks proactively.
In conclusion, managing hospital overflow in Chicago requires a multi-faceted approach that combines immediate solutions like space expansion and patient flow optimization with long-term strategies such as external partnerships and preventive care. Each strategy has its challenges, but when implemented thoughtfully, they collectively enhance a hospital’s ability to handle surges while maintaining high standards of care.
Understanding Code Blue and Code Red: Hospital Emergency Protocols Explained
You may want to see also
Frequently asked questions
Hospital capacity in Chicago fluctuates based on factors like COVID-19 surges, seasonal illnesses, and staffing levels. During peak periods, some hospitals may reach or exceed capacity, but the situation varies by facility and time.
If hospitals reach full capacity, they may implement measures like diverting ambulances to other facilities, postponing elective procedures, or setting up temporary overflow units. Coordination with regional healthcare systems also helps manage patient loads.
Most hospitals do not publicly disclose real-time bed availability. However, you can contact a specific hospital directly or check updates from local health departments or news sources during critical situations.