In the 1950s, circumcisions were often performed outside of traditional hospital settings, reflecting the era's medical practices and societal norms. Many procedures took place in doctors' offices, clinics, or even at home, particularly in rural or underserved areas where access to hospitals was limited. This was facilitated by the relative simplicity of the procedure and the availability of local anesthetics, making it feasible for general practitioners or pediatricians to perform circumcisions without the need for a hospital environment. However, the lack of standardized sterilization and safety protocols in non-hospital settings raised concerns about infection and complications, which would later contribute to shifts in medical practices in subsequent decades.
| Characteristics | Values |
|---|---|
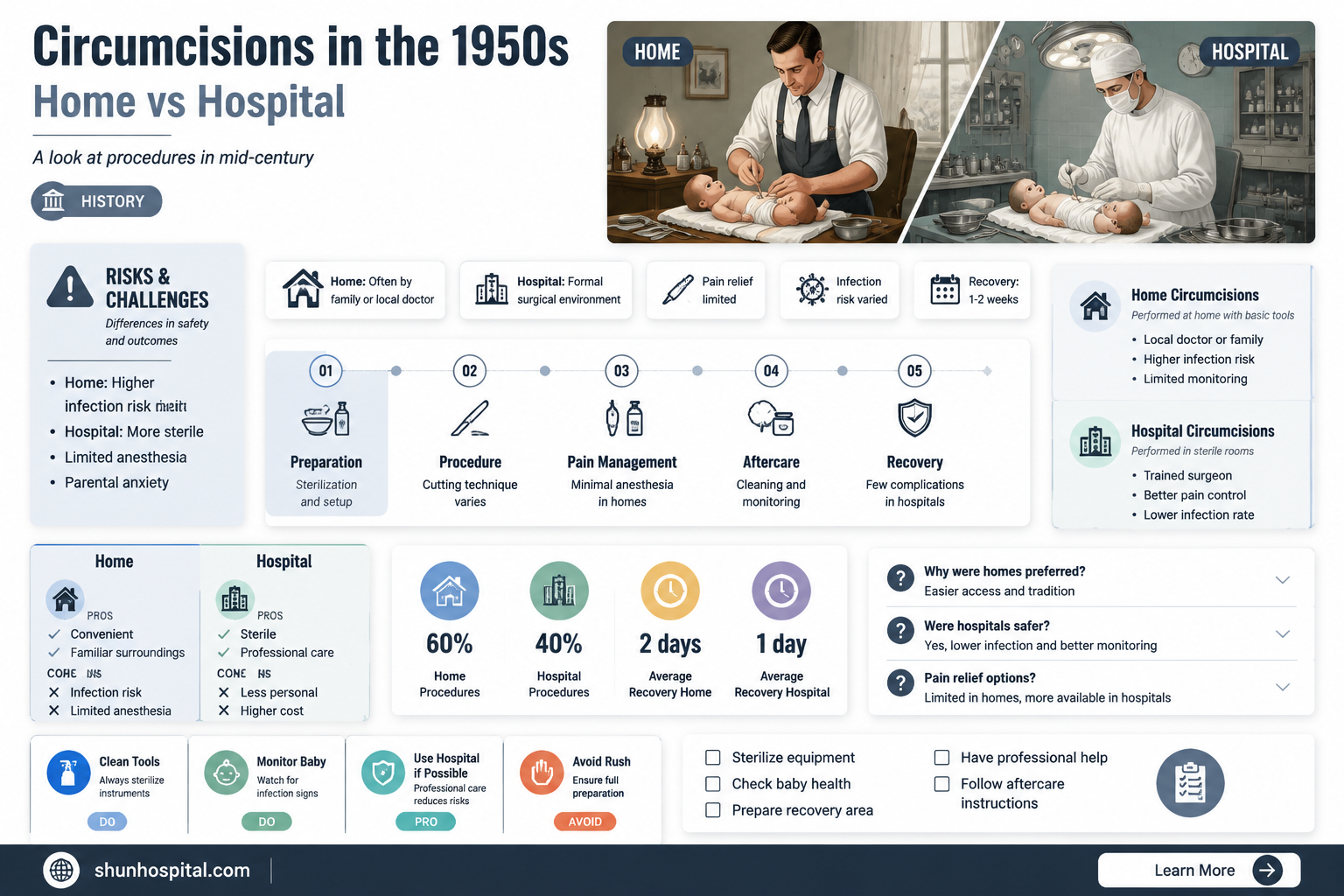
| Setting | Home, doctor's office, or other non-hospital locations |
| Anesthesia | Local anesthesia (e.g., dorsal penile nerve block) or none |
| Performer | General practitioners, pediatricians, mohelim (for religious ceremonies), or sometimes midwives |
| Technique | Various methods, including the Gomco clamp, Plastibell device, or surgical excision |
| Aftercare | Minimal post-operative care, often limited to cleaning and dressing changes |
| Complication Rate | Higher compared to hospital settings due to less sterile conditions and varying levels of expertise |
| Prevalence | Common in the 1950s, especially in regions with limited access to hospitals or for religious/cultural reasons |
| Hygiene Standards | Lower compared to modern hospital settings, increasing infection risks |
| Follow-Up Care | Limited, with parents or caregivers responsible for monitoring healing |
| Legal and Ethical Considerations | Less regulated, with varying standards depending on location and practitioner |
| Cultural/Religious Context | Often performed for religious (e.g., Jewish or Islamic) or cultural reasons, not just medical |
| Cost | Generally lower than hospital-based procedures, making it more accessible |
| Documentation | Limited records, as many procedures were not formally documented in medical systems |
Explore related products






What You'll Learn
![]()
Home circumcision practices in the 1950s
In the 1950s, home circumcision practices were not uncommon, particularly in regions where access to hospitals or specialized medical facilities was limited. Many families opted for circumcisions to be performed at home, often by individuals who were not formally trained medical professionals. These practitioners could include local doctors making house calls, midwives, mohelim (in Jewish communities), or even experienced community members who had learned the procedure through tradition or necessity. The decision to perform circumcisions at home was frequently driven by cultural, religious, or economic factors, as hospital procedures could be costly or logistically challenging.
The process of a home circumcision in the 1950s typically involved minimal medical equipment compared to modern standards. Sterilization methods were rudimentary, often relying on boiling instruments or using alcohol for disinfection. Local anesthetics, if used at all, were basic and might include cocaine or procaine solutions. Pain management was a significant concern, and infants were sometimes restrained or given sedatives like paregoric, a tincture of opium, to keep them calm during the procedure. The lack of advanced medical resources meant that complications, such as infection or excessive bleeding, were more common and harder to manage.
Religious traditions played a pivotal role in home circumcision practices during this era. In Jewish communities, the brit milah (ritual circumcision) was performed by a mohel, who was often trained in both the religious and practical aspects of the procedure. Similarly, in Islamic communities, circumcision (khitan) was sometimes conducted at home by a trained individual, though this varied widely by region and family preference. These religious ceremonies often included family and community members, blending medical practice with cultural and spiritual significance.
Despite the prevalence of home circumcisions, there were growing concerns about safety and hygiene in the 1950s. Medical professionals began advocating for hospital-based procedures to reduce risks, but this shift was gradual. Many families continued to rely on home practices due to trust in traditional methods or skepticism of modern medicine. However, as medical knowledge advanced and healthcare access improved, the trend began to move toward safer, more controlled environments for circumcisions.
In summary, home circumcision practices in the 1950s were a reflection of the era's cultural, religious, and socioeconomic realities. While these procedures were often performed out of necessity or tradition, they carried inherent risks due to limited medical resources and expertise. The transition to hospital-based circumcisions gained momentum as awareness of safety and hygiene increased, marking a significant shift in how this procedure was approached in subsequent decades.
Home Hospital: A Safe Space?
You may want to see also
Explore related products






![]()
Role of mohel in non-hospital circumcisions
In the 1950s, non-hospital circumcisions were a common practice, particularly within Jewish communities, where the ritual of brit milah (circumcision) held significant religious and cultural importance. The role of the mohel, a trained individual specializing in performing circumcisions, was central to these procedures. Mohels were often rabbis or individuals with specific religious training, but they were not typically medical professionals. Their expertise lay in adhering to the religious requirements of the ritual while ensuring the procedure was performed as safely as possible within the constraints of the time.
The mohel’s primary responsibility was to conduct the circumcision in accordance with Jewish law, which includes specific steps such as the removal of the foreskin, the recitation of blessings, and the application of a styptic to stop bleeding. In non-hospital settings, these procedures were usually carried out in private homes, synagogues, or community centers. The mohel would bring their own instruments, which were often sterilized using methods available at the time, such as boiling or alcohol wipes. While these methods were rudimentary compared to modern standards, they were considered sufficient for the task.
In addition to performing the circumcision, the mohel played a crucial role in educating the family about post-procedure care. This included instructions on cleaning the wound, applying topical treatments, and monitoring for signs of infection. Given the lack of immediate medical resources outside of a hospital, the mohel’s guidance was essential for ensuring the infant’s recovery. Families placed a high level of trust in the mohel’s expertise, as they were seen as both religious authorities and skilled practitioners of the ritual.
The mohel also served as a spiritual guide during the ceremony, explaining the significance of the brit milah to the family and community members in attendance. This dual role of religious leader and circumciser underscored the mohel’s importance in maintaining cultural and religious traditions. In the 1950s, when hospital births and medicalized circumcisions were becoming more common, the mohel’s presence in non-hospital settings was a deliberate choice by families who prioritized religious observance over medical trends.
Despite the lack of a clinical environment, mohels in the 1950s were expected to handle complications, though their ability to do so was limited compared to medical professionals. Minor issues like excessive bleeding or infection were managed with basic first aid, but severe complications would require referral to a hospital. This reality highlights the mohel’s role as a bridge between religious tradition and practical necessity, operating within the constraints of the era’s medical knowledge and resources.
In summary, the role of the mohel in non-hospital circumcisions during the 1950s was multifaceted, encompassing religious, cultural, and practical responsibilities. They were trusted figures who ensured the ritual was performed correctly, provided post-procedure care instructions, and maintained the spiritual significance of the brit milah. Their work reflects the intersection of tradition and necessity in an era when medical and religious practices often coexisted outside of institutional settings.
Why Bri's Daughter is Hospitalized: Unraveling the Concerning Situation
You may want to see also
Explore related products






![]()
Use of local anesthesia outside hospitals
In the 1950s, circumcisions were indeed performed outside of hospital settings, often in clinics, doctors' offices, or even at home. The use of local anesthesia in these non-hospital environments was a common practice, particularly for routine procedures like circumcision. Local anesthesia, such as lidocaine or procaine, was administered to numb the specific area being operated on, ensuring the patient experienced minimal pain during the procedure. This approach was favored for its simplicity and the fact that it did not require the extensive monitoring and resources associated with general anesthesia.
The administration of local anesthesia outside hospitals in the 1950s was typically carried out by trained medical professionals, including general practitioners, pediatricians, and sometimes mohelim in religious circumcision ceremonies. These practitioners would inject the anesthetic agent directly into the base of the penis or the surrounding area, using a fine needle to minimize discomfort. The procedure was relatively quick, and the onset of numbness was rapid, allowing the circumcision to be performed within minutes of the injection. This method was particularly useful in settings where access to hospital facilities was limited or where cultural and religious traditions dictated that the procedure be performed outside a hospital.
One of the key advantages of using local anesthesia for circumcisions outside hospitals was its safety profile when administered correctly. The doses used were carefully calculated based on the patient's age and weight, reducing the risk of adverse reactions. However, it was crucial for the practitioner to be well-versed in the technique and to monitor the patient for any signs of allergic reactions or other complications. In the 1950s, medical training emphasized the importance of aseptic techniques to prevent infections, which was especially critical in non-hospital settings where sterilization facilities might be less advanced.
Despite its benefits, the use of local anesthesia outside hospitals was not without challenges. Ensuring proper sterilization of equipment and maintaining a clean environment were paramount to prevent infections. Additionally, the availability of emergency equipment and medications to manage potential complications was often limited in non-hospital settings. Practitioners had to be prepared to handle rare but serious issues, such as excessive bleeding or severe allergic reactions, which could arise even with a relatively straightforward procedure like circumcision.
In summary, the use of local anesthesia for circumcisions performed outside hospitals in the 1950s was a practical and widely accepted practice. It allowed for the procedure to be conducted in various settings, accommodating cultural, religious, and logistical needs. While it offered a safe and effective means of pain management, it required skilled administration and careful attention to hygiene and potential complications. This approach reflects the medical practices of the era, balancing accessibility with the need for safety and efficacy in non-hospital environments.
Preferred Hospital: Choosing and Answering Interview Question
You may want to see also
Explore related products






![]()
Hygiene and safety in home procedures
In the 1950s, circumcisions were indeed performed outside of hospital settings, often in homes or clinics, particularly in regions where access to hospitals was limited or for cultural and religious reasons. When conducting such procedures at home, hygiene and safety were paramount to prevent infections and complications. The first critical step was to ensure a sterile environment. The area where the procedure would take place needed to be thoroughly cleaned with disinfectant solutions, and all instruments—such as scalpels, clamps, and probes—had to be sterilized using autoclaves or boiling methods. Disposable gloves, if available, were worn by the practitioner, though this was not always standard practice at the time.
Maintaining a sterile field during the procedure was essential. Instruments were laid out on clean, sterile drapes, and any contact with non-sterile surfaces was avoided. The infant or patient was also prepared with antiseptic solutions to minimize the risk of infection at the surgical site. In the 1950s, antibiotics were not as widely used prophylactically as they are today, so meticulous hygiene was the primary defense against post-operative infections. Caregivers were often instructed to keep the area clean and dry after the procedure, using sterile dressings and avoiding irritants.
Safety measures extended beyond hygiene. The person performing the circumcision needed to be trained and experienced, as improper technique could lead to severe complications such as excessive bleeding, infection, or damage to the penis. In home settings, having a second person present to assist and monitor the patient was advisable. Additionally, basic emergency supplies, such as sterile gauze, bandages, and a tourniquet, should be readily available in case of unexpected bleeding.
Another critical aspect of safety was pain management. In the 1950s, local anesthesia was not always used for infant circumcisions, but when performed at home, some form of pain relief, such as a topical numbing agent or a sugar solution for infants, was often employed. Ensuring the patient was calm and secure during the procedure was also important, as distress could lead to movement and increase the risk of injury.
Finally, post-procedure care was vital for hygiene and safety. Caregivers were instructed to monitor the area for signs of infection, such as redness, swelling, or discharge, and to seek medical attention immediately if complications arose. Keeping the area clean and avoiding tight diapers or clothing helped prevent irritation and promote healing. While home circumcisions in the 1950s were common, they required strict adherence to hygiene and safety protocols to minimize risks and ensure the best possible outcome.
John Q Filming Locations: Which Hospital Was It?
You may want to see also
Explore related products

$16.99





![]()
Legal and cultural norms of the era
In the 1950s, the legal and cultural norms surrounding circumcision in the United States and many Western countries were significantly different from those of today. Circumcision was widely accepted as a routine medical procedure, often performed shortly after birth, but the settings in which these procedures took place varied. While hospitals were the most common and preferred locations for circumcisions, it was not uncommon for them to be performed outside of traditional medical facilities, particularly in rural or underserved areas. Legally, there were fewer regulations governing who could perform circumcisions, and in some cases, non-medical personnel, such as mohelim in Jewish communities or even midwives, conducted the procedure. This practice was often rooted in cultural or religious traditions rather than medical necessity.
Culturally, circumcision in the 1950s was influenced by prevailing medical beliefs and societal attitudes. The procedure was frequently recommended by doctors for reasons ranging from hygiene to the prevention of perceived future health issues, despite limited scientific evidence supporting these claims. In Jewish and Muslim communities, circumcision was a religious rite, and these rituals were often performed outside of hospitals, in homes or places of worship. The cultural acceptance of such practices was high, and legal systems generally respected religious freedoms, allowing these traditions to continue without significant interference. However, the lack of standardized medical oversight in non-hospital settings raised concerns about safety and hygiene, though these issues were not widely publicized or addressed during the era.
The legal framework of the 1950s did not strictly mandate that circumcisions be performed by licensed medical professionals in hospital settings. In many jurisdictions, there were no specific laws prohibiting non-medical personnel from conducting circumcisions, particularly in cases of religious ceremonies. This leniency was partly due to the era's general deference to religious practices and the limited role of government in personal medical decisions. However, as medicalization of childbirth and neonatal care increased, there was a gradual shift toward preferring hospital-based procedures, though this transition was not yet complete by the 1950s. Rural areas, in particular, often relied on local practitioners or community members due to limited access to hospitals or medical professionals.
Cultural norms also played a significant role in shaping the acceptance of out-of-hospital circumcisions. In Jewish communities, the brit milah (ritual circumcision) was typically performed by a mohel, often in the family home, and this practice was deeply ingrained in religious and cultural traditions. Similarly, in some Muslim communities, circumcision was conducted by religious leaders or traditional practitioners. These rituals were viewed as essential components of cultural and religious identity, and their performance outside of hospitals was widely accepted. The broader society generally respected these practices, and legal systems tended to accommodate them, reflecting the era's emphasis on religious freedom and cultural autonomy.
Despite the prevalence of out-of-hospital circumcisions, there were growing concerns within the medical community about the risks associated with non-sterile environments and lack of trained personnel. However, these concerns were not yet strong enough to prompt widespread legal changes or public outcry. The 1950s marked a transitional period, where traditional practices coexisted with increasing medicalization, but cultural and religious norms continued to play a dominant role in determining where and how circumcisions were performed. This era's legal and cultural landscape allowed for a diversity of practices, reflecting the complex interplay between tradition, religion, and emerging medical standards.
Detecting Kidney Stones: Hospital Procedures and Tests
You may want to see also
Frequently asked questions
Yes, circumcisions in the 1950s were often performed in settings other than hospitals, including doctors' offices, clinics, and even at home by trained professionals or traditional practitioners.
Circumcisions were often carried out by general practitioners, pediatricians, or mohelim (in Jewish religious contexts). In some cases, midwives or traditional practitioners performed the procedure, especially in rural or non-Western settings.
Yes, there were risks, including infection, bleeding, and complications from inadequate sterilization or lack of medical supervision. However, many procedures were performed safely by trained individuals using available medical standards of the time.































