The question of whether hospital CMIS (Clinical Management Information Systems) are posted publicly or accessible to patients and stakeholders is a critical topic in healthcare transparency and data management. As hospitals increasingly adopt digital systems to streamline patient care, billing, and administrative processes, the visibility and availability of CMIS data have become a point of interest. While some healthcare providers share certain aspects of their CMIS, such as appointment schedules or patient records, through secure portals, the extent to which these systems are posted or made publicly accessible varies widely. This raises important considerations regarding patient privacy, compliance with regulations like HIPAA, and the balance between transparency and data security in modern healthcare settings.
Explore related products






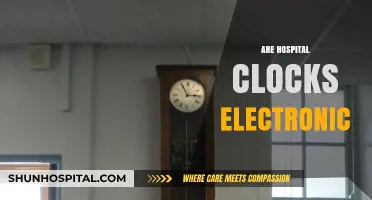
What You'll Learn
- CMI Posting Requirements: Regulations and guidelines for posting Clinical Management Information (CMI) in hospitals
- CMI Data Accuracy: Ensuring precision and reliability of CMI data before posting in hospital systems
- CMI Access Control: Managing user permissions and security for accessing posted CMI in hospitals
- CMI Reporting Tools: Software and platforms used for generating and posting CMI reports in hospitals
- CMI Compliance Audits: Regular checks to ensure posted CMI meets hospital and regulatory standards
![]()
CMI Posting Requirements: Regulations and guidelines for posting Clinical Management Information (CMI) in hospitals
Hospitals must adhere to strict regulations when posting Clinical Management Information (CMI) to ensure patient confidentiality, compliance with legal standards, and data accuracy. The Health Insurance Portability and Accountability Act (HIPAA) in the United States, for instance, mandates that any displayed CMI must be accessible only to authorized personnel and must exclude direct patient identifiers unless absolutely necessary. Similarly, the General Data Protection Regulation (GDPR) in Europe requires hospitals to anonymize or pseudonymize patient data before posting, ensuring that individuals cannot be easily identified. Failure to comply with these regulations can result in severe penalties, including fines and legal action, making it imperative for hospitals to establish robust protocols for CMI posting.
When posting CMI, hospitals must follow a structured process to maintain data integrity and accessibility. First, determine the purpose of the posting—whether it’s for clinical decision-making, quality improvement, or staff training. Next, identify the specific data elements required, such as diagnostic codes, treatment plans, or medication dosages (e.g., 5 mg of warfarin for patients aged 65 and older). Use standardized formats like ICD-10 codes for diagnoses and SNOMED CT for clinical terms to ensure consistency. Finally, designate secure locations for posting, such as password-protected intranet sites or locked bulletin boards in restricted areas. Regular audits of posted CMI are essential to verify compliance and address any discrepancies promptly.
A comparative analysis of CMI posting practices reveals variations across hospitals, often influenced by local regulations and institutional policies. For example, some hospitals may post CMI in real-time on digital dashboards accessible to all clinical staff, while others limit access to department-specific portals. In pediatric wards, CMI postings might include age-specific guidelines, such as adjusting medication dosages for children under 12 (e.g., 0.5 mg/kg of acetaminophen for fever management). Conversely, geriatric units may emphasize comorbidity management, posting protocols for patients with multiple chronic conditions. These differences highlight the need for tailored approaches that balance accessibility with patient privacy and clinical relevance.
To ensure effective CMI posting, hospitals should adopt practical tips that streamline the process while maintaining compliance. Train staff on the importance of data privacy and the consequences of unauthorized sharing. Implement role-based access controls to restrict CMI visibility to relevant personnel only. For example, nurses may need access to medication schedules, while administrators focus on resource allocation metrics. Additionally, use color-coding or symbols to differentiate between sensitive and non-sensitive information, reducing the risk of accidental exposure. Regularly update posted CMI to reflect the latest clinical guidelines, such as revised antibiotic dosing protocols for resistant infections. By integrating these practices, hospitals can enhance the utility of CMI postings while safeguarding patient information.
Enhancing Patient Care: Crafting Effective Hospital Quality Improvement Plans
You may want to see also
Explore related products






![]()
CMI Data Accuracy: Ensuring precision and reliability of CMI data before posting in hospital systems
Clinical Modification (CMI) data forms the backbone of healthcare analytics, influencing everything from patient care to reimbursement. Yet, its accuracy is often compromised by human error, outdated coding practices, or system incompatibilities. A single misplaced digit in a diagnosis code can lead to incorrect treatment plans or financial penalties. For instance, mistyping "E11.9" (Type 2 diabetes without complications) as "E10.9" (Type 1 diabetes without complications) alters the patient’s care trajectory entirely. Ensuring precision begins with standardized data entry protocols, such as mandatory double-checks for high-risk codes and automated alerts for inconsistent entries. Without these safeguards, even minor discrepancies can snowball into systemic issues, undermining trust in hospital CMIs.
Consider the workflow of a busy emergency department, where nurses and physicians input CMI data under time pressure. Here, accuracy hinges on intuitive interfaces and real-time validation tools. For example, integrating drop-down menus for common diagnoses or dosage ranges (e.g., 50–100 mg for metoprolol in hypertension patients) reduces manual errors. However, reliance on technology alone is insufficient. Staff training must emphasize the criticality of precise coding, particularly for age-specific categories like pediatric dosages (e.g., 5 mg/kg of acetaminophen for children under 12). Hospitals that combine user-friendly systems with rigorous training report up to 30% fewer coding errors, highlighting the interplay between human and technological factors.
The stakes of inaccurate CMI data extend beyond individual patients to population health initiatives. Misclassified data can skew epidemiological trends, leading to misguided resource allocation. For instance, overreporting of "J45" (asthma) in a community might prompt unnecessary inhaler stockpiles while underreporting "F11.2" (opioid dependence) could leave addiction services underfunded. To mitigate this, hospitals should implement periodic audits and cross-reference CMI data with external sources like state health registries. A comparative analysis of internal and external datasets can reveal discrepancies, such as a 15% variance in diabetes prevalence rates, prompting corrective action. Such proactive measures ensure that posted CMIs reflect reality, not systemic biases.
Finally, the reliability of CMI data is contingent on its compatibility with evolving healthcare standards. As ICD-11 replaces ICD-10, hospitals must update their systems to accommodate new codes and structures. For example, ICD-11 introduces more granular coding for mental health conditions, requiring staff to differentiate between "6D40" (anxiety disorders) and "6D41" (phobic anxiety disorders). Failure to adapt risks rendering historical data incompatible with future analytics. Hospitals should adopt phased transition plans, starting with pilot departments and gradually scaling up. By prioritizing flexibility and foresight, they can ensure that posted CMIs remain accurate, reliable, and future-proof.
Chicago Hospitals: Success Stories and Challenges
You may want to see also
Explore related products






![]()
CMI Access Control: Managing user permissions and security for accessing posted CMI in hospitals
Clinical Management Information (CMI) systems in hospitals are increasingly being posted online or made accessible through digital platforms to enhance efficiency and patient care. However, this shift raises critical concerns about user permissions and security. Unauthorized access to sensitive patient data can lead to breaches, legal repercussions, and compromised trust. Effective CMI access control is not just a technical necessity but a cornerstone of healthcare integrity.
Consider the following scenario: a nurse requires access to a patient’s CMI to administer a specific medication, such as 500 mg of amoxicillin twice daily for a 12-year-old with a bacterial infection. Without proper access controls, this information could be viewed or altered by unauthorized personnel, potentially leading to medication errors or privacy violations. Role-based access control (RBAC) is a practical solution, where permissions are assigned based on job responsibilities. For instance, nurses might have read-only access to medication histories, while pharmacists could have edit privileges for dosage adjustments.
Implementing CMI access control involves a multi-step process. First, identify user roles and their corresponding access needs. Next, configure the system to enforce these permissions, ensuring that only authorized users can view, edit, or share CMI. Regular audits are essential to monitor access patterns and detect anomalies. For example, if a janitorial staff member repeatedly accesses patient records, this could indicate a security gap. Tools like multi-factor authentication (MFA) add an extra layer of protection, requiring users to verify their identity through a second method, such as a code sent to their phone.
Despite these measures, challenges persist. Overly restrictive access controls can hinder workflow, while lax security invites risks. Striking the right balance requires collaboration between IT teams, healthcare providers, and compliance officers. For instance, a hospital might allow temporary elevated access during emergencies, such as granting a resident physician full CMI access during a code blue, but automatically revoking it afterward.
In conclusion, managing user permissions and security for posted CMI in hospitals is a delicate but essential task. By adopting RBAC, conducting regular audits, and leveraging tools like MFA, healthcare organizations can safeguard patient data while maintaining operational efficiency. The goal is not just to comply with regulations but to foster a culture of accountability and trust in digital healthcare systems.
Medieval Hospitals: Who Received Treatment?
You may want to see also
Explore related products






![]()
CMI Reporting Tools: Software and platforms used for generating and posting CMI reports in hospitals
Hospitals rely on Case Mix Index (CMI) reporting to measure patient acuity, allocate resources, and optimize reimbursement. Generating accurate, timely CMI reports requires specialized software and platforms that streamline data collection, analysis, and visualization. Tools like 3M 360 Encompass, Optum’s Episode Treatment Groups (ETGs), and Premier’s Clinical and Financial Performance (CFP) platform dominate this space, offering features such as automated coding, benchmarking, and predictive analytics. These systems integrate with electronic health records (EHRs) to pull data seamlessly, reducing manual errors and ensuring compliance with regulatory standards like MS-DRGs or APR-DRGs.
Selecting the right CMI reporting tool involves evaluating specific hospital needs, such as size, specialty focus, and budget. For instance, smaller hospitals might prioritize cost-effective solutions with basic reporting capabilities, while larger systems may require advanced analytics and customization options. Cloud-based platforms like Kaufman Hall’s Axiom Software offer scalability and remote access, ideal for multi-facility networks. Conversely, on-premise solutions provide greater control over data security but demand higher IT infrastructure investment. Hospitals must also consider interoperability with existing systems to avoid data silos and ensure smooth workflow integration.
Implementation of CMI reporting tools requires careful planning to maximize ROI. Start by defining key performance indicators (KPIs) such as CMI trends, length of stay, and readmission rates. Train staff on software functionality and reporting workflows to ensure consistent usage. Regularly audit data accuracy to identify discrepancies between reported and actual CMIs, which can impact reimbursement. For example, a hospital using 3M 360 Encompass might discover undercoding of comorbidities, leading to a lower CMI and reduced payments. Addressing such issues promptly ensures financial health and operational efficiency.
The future of CMI reporting tools lies in artificial intelligence (AI) and machine learning (ML) integration. AI-driven platforms can predict patient acuity shifts, optimize staffing, and identify cost-saving opportunities. For instance, Optum’s ETGs combined with AI can forecast high-risk patient populations, enabling proactive interventions. However, hospitals must balance innovation with ethical considerations, ensuring transparency in AI-generated insights. As value-based care models expand, CMI reporting tools will evolve to support population health management, making them indispensable for hospitals navigating complex healthcare landscapes.
How Hospitals Help with Semen-Related Issues
You may want to see also
Explore related products





![]()
CMI Compliance Audits: Regular checks to ensure posted CMI meets hospital and regulatory standards
Hospitals must ensure that Clinical Management Information (CMI) is not only posted but also compliant with stringent standards. CMI Compliance Audits serve as the backbone of this process, systematically verifying that all displayed information aligns with both internal hospital policies and external regulatory requirements. These audits are critical because even minor discrepancies in CMI—such as outdated dosage guidelines or missing patient age categories—can lead to severe clinical errors, legal liabilities, or compromised patient safety. For instance, a misplaced decimal in a medication dosage (e.g., 5.0 mg vs. 50 mg) could have life-threatening consequences, underscoring the need for meticulous scrutiny.
Conducting CMI Compliance Audits involves a structured approach. First, identify all posted CMI materials, including digital displays, printed charts, and online portals. Next, cross-reference these materials against the latest regulatory guidelines, such as those from the Joint Commission or FDA, and hospital-specific protocols. For example, audits should confirm that pediatric dosage charts clearly differentiate between age groups (e.g., neonates, infants, toddlers) and that emergency response protocols are updated with the most recent CPR guidelines. Practical tips include using checklists tailored to specific departments (e.g., oncology, pediatrics) and involving interdisciplinary teams to ensure comprehensive coverage.
One of the challenges in CMI Compliance Audits is balancing thoroughness with efficiency. Auditors must avoid superficial checks, such as merely confirming the presence of posters, and instead delve into content accuracy. For instance, a posted antibiotic guideline should not only list dosages but also include contraindications and monitoring instructions. Comparative analysis can be useful here: compare current CMI against historical versions to track changes and identify potential oversights. Additionally, leveraging technology, such as QR codes linking to verified digital resources, can streamline audits and reduce human error.
The persuasive case for regular CMI Compliance Audits lies in their proactive nature. Rather than waiting for incidents to expose gaps, audits act as a preventive measure, fostering a culture of continuous improvement. Hospitals that prioritize these audits often report fewer medication errors and higher staff confidence in posted information. For example, a hospital that implemented quarterly audits saw a 30% reduction in dosage-related incidents within the first year. This data-driven approach not only enhances patient safety but also strengthens the hospital’s standing during regulatory inspections.
In conclusion, CMI Compliance Audits are indispensable for maintaining the integrity of posted clinical information. By combining analytical rigor, practical strategies, and a persuasive focus on outcomes, hospitals can ensure that their CMI meets the highest standards. Whether through detailed checklists, technological integration, or interdisciplinary collaboration, the goal remains clear: to safeguard patient care through accurate, up-to-date, and compliant information.
Fetterman's Health: Discharged and Campaigning
You may want to see also
Frequently asked questions
Hospital CMIs are typically not posted publicly due to privacy and security concerns. Access is usually restricted to authorized healthcare professionals and administrators.
Patients can often access their personal health information through patient portals or by requesting records directly from the hospital, but full CMI data is generally not available to patients.
Hospital CMIs may be shared with external organizations for research, regulatory compliance, or healthcare improvement purposes, but this is done under strict data-sharing agreements and privacy regulations.