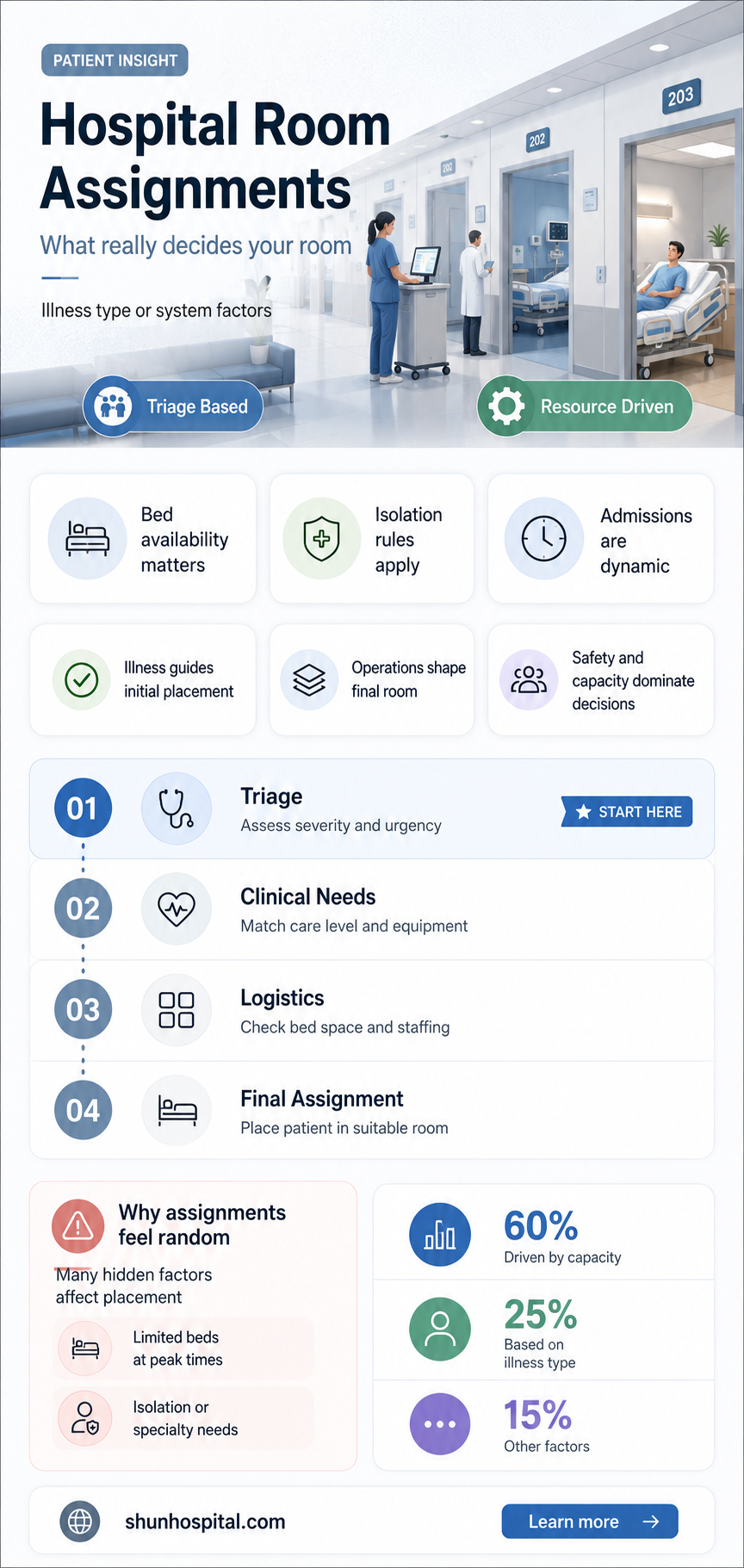
Hospital room assignments are often perceived as being solely determined by the nature of a patient's illness, but in reality, the process is far more complex and multifaceted. While the severity and type of condition do play a significant role in determining placement, other factors such as bed availability, patient preferences, and hospital policies also heavily influence these decisions. For instance, patients with similar medical needs might be grouped together for efficient resource allocation, while others may be separated to prevent cross-contamination or ensure specialized care. Additionally, logistical considerations like proximity to necessary equipment or staff expertise can further shape room assignments. Understanding this nuanced process highlights the delicate balance hospitals must strike between medical necessity and operational efficiency.
| Characteristics | Values |
|---|---|
| Primary Factor | Patient's medical condition and required level of care |
| Additional Factors | - Bed availability - Staffing ratios - Infection control needs - Patient preferences (when possible) - Length of stay - Special equipment requirements |
| Always Based on Illness? | No, while illness is a major factor, it's not the sole determinant. |
| Examples of Non-Illness Based Assignments | - Placing a patient needing frequent monitoring near nurses' station - Isolating infectious patients regardless of primary diagnosis - Grouping patients with similar care needs (e.g., post-surgical recovery) |
| Importance of Flexibility | Hospitals need flexibility to adapt assignments based on dynamic factors like bed availability and patient needs. |
Explore related products






What You'll Learn
- Patient Privacy vs. Illness Grouping: Balancing privacy needs with efficient illness-based room assignments
- Resource Allocation Impact: How illness-based assignments affect hospital resource distribution and management
- Infection Control Measures: Role of room assignments in preventing illness-specific infections
- Patient Comfort Considerations: Impact of illness-based assignments on patient comfort and recovery
- Alternative Assignment Methods: Exploring non-illness-based criteria for hospital room allocations
![]()
Patient Privacy vs. Illness Grouping: Balancing privacy needs with efficient illness-based room assignments
In the complex environment of healthcare, the allocation of hospital rooms is a critical aspect that impacts both patient privacy and the efficiency of medical care. The question of whether room assignments are always based on the nature of illness is a nuanced one, as it involves balancing the need for specialized care with the fundamental right to privacy. While illness-based grouping can streamline treatment and resource allocation, it must be carefully managed to avoid compromising patient confidentiality and dignity.
The Case for Illness-Based Room Assignments
Grouping patients with similar medical conditions can significantly enhance the efficiency of healthcare delivery. For instance, patients with infectious diseases are often isolated in designated wards to prevent cross-contamination, while those undergoing similar treatments, such as chemotherapy, may benefit from shared spaces where medical equipment and staff expertise are readily available. This approach not only optimizes resource utilization but also fosters a sense of community among patients facing similar health challenges. Additionally, it allows healthcare providers to tailor the environment to specific medical needs, such as low-stimulation rooms for neurological patients or specialized monitoring for critical cases.
Privacy Concerns in Illness-Based Grouping
Despite its advantages, illness-based room assignments raise significant privacy concerns. Patients may feel uncomfortable sharing spaces with others who have similar conditions, fearing that their medical status could become known to fellow patients or visitors. This is particularly sensitive for individuals with stigmatized illnesses, such as HIV/AIDS or mental health disorders, where disclosure could lead to discrimination or emotional distress. Moreover, the risk of inadvertent information sharing in shared spaces can erode trust in the healthcare system, making patients hesitant to seek care or disclose critical details about their health.
Strategies to Balance Privacy and Efficiency
To address these challenges, hospitals must implement strategies that balance the benefits of illness-based grouping with robust privacy protections. One approach is the use of semi-private rooms with physical barriers or curtains to provide visual and auditory privacy. Hospitals can also adopt strict confidentiality policies, training staff to avoid discussing patient conditions in shared areas and ensuring that medical records are handled discreetly. Additionally, offering patients the option to request alternative room assignments, when feasible, can empower them to prioritize their privacy needs.
Technological Solutions and Patient-Centered Design
Advancements in technology and patient-centered design offer innovative ways to mitigate privacy risks while maintaining efficient room assignments. Electronic health records (EHRs) with stringent access controls can prevent unauthorized information sharing, while smart room designs that incorporate soundproofing and modular layouts can enhance privacy in shared spaces. Furthermore, digital tools such as patient portals and mobile apps can enable individuals to manage their health information discreetly, reducing the need for verbal discussions in public areas.
Ultimately, the decision to assign hospital rooms based on the nature of illness requires a delicate balance between operational efficiency and patient privacy. While illness-based grouping can improve care delivery, it must be implemented with a deep respect for individual rights and dignity. By adopting thoughtful policies, leveraging technology, and prioritizing patient-centered design, hospitals can create environments that optimize treatment outcomes while safeguarding privacy, ensuring that every patient feels respected and secure during their stay.
Connect Chromecast to Hospital Wi-Fi: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Resource Allocation Impact: How illness-based assignments affect hospital resource distribution and management
Hospital room assignments based on the nature of illness significantly impact resource allocation, influencing how hospitals distribute and manage their limited resources. When patients are grouped according to their medical conditions, hospitals can optimize the use of specialized equipment, staff expertise, and medications. For instance, patients with infectious diseases are often isolated in designated wards to prevent cross-contamination, ensuring that resources like personal protective equipment (PPE) and disinfection supplies are concentrated where they are most needed. This targeted approach minimizes waste and enhances efficiency, as resources are not spread thinly across unrelated cases.
Illness-based assignments also streamline staffing by aligning healthcare professionals with their areas of expertise. For example, oncology patients housed in the same unit benefit from the concentrated presence of oncologists, nurses trained in chemotherapy administration, and support staff familiar with cancer care protocols. This specialization reduces the time staff spend traveling between disparate locations and allows for quicker response times to patient needs. Additionally, it fosters a collaborative environment where multidisciplinary teams can easily coordinate care, further improving resource utilization and patient outcomes.
However, illness-based room assignments can strain resources if not carefully managed. High-demand specialties, such as intensive care or cardiology, may require more advanced equipment and highly trained personnel, leading to resource bottlenecks. Hospitals must balance the need for specialized care with the availability of resources, often requiring dynamic adjustments to accommodate fluctuating patient volumes. For instance, during a surge in respiratory illnesses, hospitals may need to reallocate ventilators and respiratory therapists to the affected ward, potentially leaving other areas understaffed or under-equipped.
Another critical aspect of resource allocation in illness-based assignments is the management of shared facilities and services. Diagnostic tools like MRI machines or laboratories are often centralized, but their usage must be prioritized based on the needs of specific patient groups. Hospitals employing illness-based assignments can schedule these resources more effectively, reducing wait times for critical tests and procedures. However, this requires robust communication and coordination among departments to ensure that no single group monopolizes shared resources at the expense of others.
Finally, illness-based room assignments influence long-term resource planning and investment. By analyzing patient distribution patterns, hospitals can identify trends in disease prevalence and allocate funds to expand or upgrade facilities accordingly. For example, a rise in chronic diseases like diabetes may prompt investment in endocrinology wards and related equipment. This proactive approach ensures that resources are allocated sustainably, aligning with the evolving healthcare needs of the population. In summary, while illness-based assignments offer numerous advantages for resource distribution and management, they require careful planning and flexibility to address potential challenges and ensure equitable care across all patient groups.
Deadly Foodborne Pathogens: Which One Tops Hospitalization Rates?
You may want to see also
Explore related products





![]()
Infection Control Measures: Role of room assignments in preventing illness-specific infections
Infection control measures in hospitals are critical for preventing the spread of illness-specific infections, and room assignments play a pivotal role in this process. While hospital room assignments are not always solely based on the nature of the illness, they are strategically planned to minimize the risk of cross-contamination and protect vulnerable patients. For instance, patients with infectious diseases such as tuberculosis (TB), methicillin-resistant *Staphylococcus aureus* (MRSA), or Clostridioides difficile (C. diff) are often placed in isolation rooms with negative pressure ventilation to prevent airborne or contact transmission. These rooms are designed to ensure that contaminated air is contained and filtered before being released, safeguarding both healthcare workers and other patients.
The nature of the illness significantly influences room assignments, particularly when dealing with highly contagious pathogens. For example, patients with respiratory infections like COVID-19 or influenza may be cohorted together in designated wards to reduce the risk of spreading the virus to non-infected individuals. However, this approach requires careful consideration of each patient’s immune status and comorbidities to avoid unintended exposure. Similarly, immunocompromised patients, such as those undergoing chemotherapy or organ transplants, are often placed in private rooms or areas with enhanced protective measures to shield them from opportunistic infections. This tailored approach underscores the importance of aligning room assignments with infection control protocols.
Another critical aspect of room assignments is the segregation of patients based on infection type to prevent healthcare-associated infections (HAIs). For instance, patients with antibiotic-resistant bacteria are often isolated to limit the spread of these pathogens, which can be particularly dangerous in hospital settings. Additionally, surgical patients may be housed in separate units to minimize their exposure to infectious agents, as their immune systems may be temporarily compromised post-operation. By categorizing patients based on their infection risk and susceptibility, hospitals can implement targeted infection control measures, such as dedicated staff, specialized cleaning protocols, and personal protective equipment (PPE) requirements.
Effective room assignments also depend on real-time surveillance and communication within the healthcare team. Infection control specialists and nurses must collaborate to assess patient conditions, identify potential infection risks, and adjust room allocations accordingly. Electronic health records (EHRs) and infection tracking systems play a vital role in this process, enabling staff to quickly identify patients with infectious diseases and ensure they are placed in appropriate settings. Furthermore, educating patients and their families about the rationale behind room assignments can foster compliance with isolation precautions and reduce the likelihood of breaches in infection control protocols.
In conclusion, while hospital room assignments are not exclusively based on the nature of the illness, they are a cornerstone of infection control measures aimed at preventing illness-specific infections. By strategically placing patients in isolation rooms, cohorting those with similar infections, and segregating high-risk individuals, hospitals can significantly reduce the transmission of pathogens. This proactive approach, combined with robust surveillance and interdisciplinary collaboration, ensures that room assignments contribute effectively to the broader goal of maintaining a safe and healthy healthcare environment.
Israel's Underground Tunnels: Shifa Hospital's Secrets
You may want to see also
Explore related products






![]()
Patient Comfort Considerations: Impact of illness-based assignments on patient comfort and recovery
Hospital room assignments are not always strictly based on the nature of the illness, but when they are, it can significantly impact patient comfort and recovery. Illness-based assignments often aim to group patients with similar medical conditions together, which can streamline care delivery and create a more specialized environment. For instance, patients with infectious diseases may be placed in isolation rooms to prevent the spread of pathogens, while those recovering from surgery might be housed in quieter, low-stimulation areas. This approach can enhance comfort by ensuring that the physical environment aligns with the patient’s specific needs, such as reduced noise levels for post-operative recovery or easy access to specialized equipment for chronic conditions. However, this practice must be balanced with the potential for patients to feel stigmatized or isolated if grouped solely by their illness, which can negatively affect mental well-being.
One of the key benefits of illness-based room assignments is the optimization of medical resources and staff expertise. When patients with similar conditions are grouped together, healthcare providers can more efficiently allocate time, equipment, and specialized care. For example, a ward dedicated to cardiac patients allows nurses and doctors with cardiology expertise to focus their efforts, potentially improving the quality of care. This efficiency can indirectly enhance patient comfort by reducing wait times and ensuring that interventions are timely and appropriate. Additionally, patients may feel more at ease knowing they are surrounded by staff who are highly familiar with their specific condition, fostering a sense of security and trust in their treatment plan.
Despite these advantages, illness-based assignments can sometimes compromise patient comfort if not carefully managed. For instance, grouping patients with the same severe or terminal illness may create an environment of shared anxiety or despair, which can hinder emotional recovery. Patients may also feel a loss of individuality if their room assignment reinforces their identity as "just another case" of a particular disease. To mitigate this, hospitals should complement illness-based assignments with personalized care plans and emotional support services, such as counseling or peer support groups, to address the psychological impact of such groupings.
Another important consideration is the physical layout and amenities of hospital rooms in illness-based assignments. For example, patients with mobility issues due to orthopedic conditions may require rooms with wider doorways, grab bars, and easy access to physical therapy spaces. Similarly, patients with respiratory conditions may benefit from rooms with better ventilation or proximity to outdoor areas. When these factors are taken into account, illness-based assignments can significantly improve comfort by tailoring the environment to the patient’s functional needs. However, hospitals must ensure that these specialized rooms are available and that patients are not placed in suboptimal settings due to resource constraints.
Finally, the impact of illness-based room assignments on patient recovery cannot be overlooked. A well-designed assignment system can promote faster healing by minimizing disruptions and providing a conducive environment for rest and rehabilitation. For example, patients with neurological conditions may recover more effectively in rooms with controlled lighting and minimal sensory stimuli. Conversely, poor assignments—such as placing a patient with a sleep disorder in a noisy area—can delay recovery and increase stress. Hospitals should therefore adopt a holistic approach, considering not only the medical condition but also the patient’s overall comfort, preferences, and psychosocial needs when making room assignments. By doing so, they can maximize the positive impact of illness-based assignments on both comfort and recovery.
Hospitalization Decision for Aplastic Anemia: When and Why?
You may want to see also
Explore related products





![]()
Alternative Assignment Methods: Exploring non-illness-based criteria for hospital room allocations
Hospital room assignments traditionally prioritize the nature of illness, ensuring patients with similar medical conditions are grouped together for efficient care. However, this approach may overlook other factors that significantly impact patient comfort, recovery, and overall experience. Exploring alternative assignment methods based on non-illness-based criteria could lead to more holistic and patient-centered hospital environments. For instance, assigning rooms based on patient preferences, such as proximity to family or quiet areas, can enhance emotional well-being, which is crucial for recovery. Similarly, grouping patients by language or cultural background can improve communication and reduce feelings of isolation, fostering a more supportive atmosphere.
Another non-illness-based criterion is logistical efficiency, which considers factors like mobility and frequency of medical interventions. Patients requiring frequent monitoring or those with limited mobility could be placed closer to nursing stations or critical care areas, reducing response times and minimizing physical strain on staff. This method not only optimizes resource allocation but also ensures that patients receive timely care. Additionally, socio-behavioral compatibility could be a factor, where patients with similar personalities, lifestyles, or interests are roomed together. This approach may reduce conflicts and create a more harmonious environment, particularly in shared rooms.
Incorporating technological preferences into room assignments is another innovative idea. Hospitals could allocate rooms based on patients' comfort with technology, such as smart beds or remote monitoring devices. Tech-savvy patients might benefit from rooms equipped with advanced systems, while others may prefer simpler setups. This ensures that technology enhances rather than complicates the patient experience. Furthermore, environmental preferences, such as natural light exposure or temperature settings, could be considered to tailor the physical environment to individual needs, promoting comfort and faster recovery.
A patient-centric approach that includes psychological and emotional factors could also be transformative. For example, assigning rooms based on stress levels or anxiety profiles might allow hospitals to provide targeted psychological support. Patients with high anxiety could be placed in quieter areas or given access to calming amenities, while more social patients might benefit from shared spaces. This method acknowledges the interplay between mental health and physical recovery, addressing both aspects holistically.
Finally, flexibility and adaptability should be core principles in alternative assignment methods. Hospitals could implement dynamic systems that allow for adjustments based on real-time feedback and changing patient needs. For instance, a patient initially assigned based on logistical efficiency might later be moved to a quieter area if their condition stabilizes. Such adaptability ensures that room assignments remain optimal throughout the patient's stay, maximizing both clinical outcomes and satisfaction. By embracing these non-illness-based criteria, hospitals can create more personalized, efficient, and compassionate care environments.
Florence's Foundling Hospital: Completion Date and Historical Significance
You may want to see also
Frequently asked questions
No, hospital room assignments are not always solely based on the nature of illness. Factors like patient needs, bed availability, infection control, and hospital policies also play a role.
Yes, patients with different illnesses can share a room, especially in semi-private or shared rooms, unless there are specific medical or infection control reasons to separate them.
Not necessarily. While some critical illnesses may require private rooms for isolation or specialized care, many critical care units use shared spaces depending on the hospital's layout and resources.
Hospitals consider factors like patient gender, age, mobility, infection risk, and available resources. The goal is to ensure safety, efficiency, and optimal care for all patients.