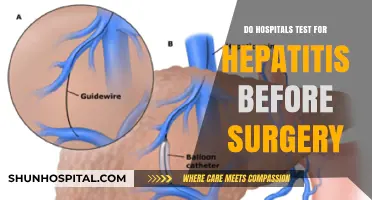
The cost of prescription drugs in the US is notoriously high, with one in three adults saying they have been unable to take their medication as prescribed due to cost. There are many factors contributing to the high cost of prescription drugs, and hospitals and pharmacies are subject to different pricing schemes. Hospitals can retain a substantial share of insurer pharmaceutical expenditures, and as they have consolidated into large health systems, they have been able to increase the reimbursement prices they demand from insurers. This article will explore whether hospitals upcharge medications compared to pharmacies.
| Characteristics | Values |
|---|---|
| High prescription drug spending | In 2021, the US had the highest per capita prescription drug spending at an average of $1,432 per American. |
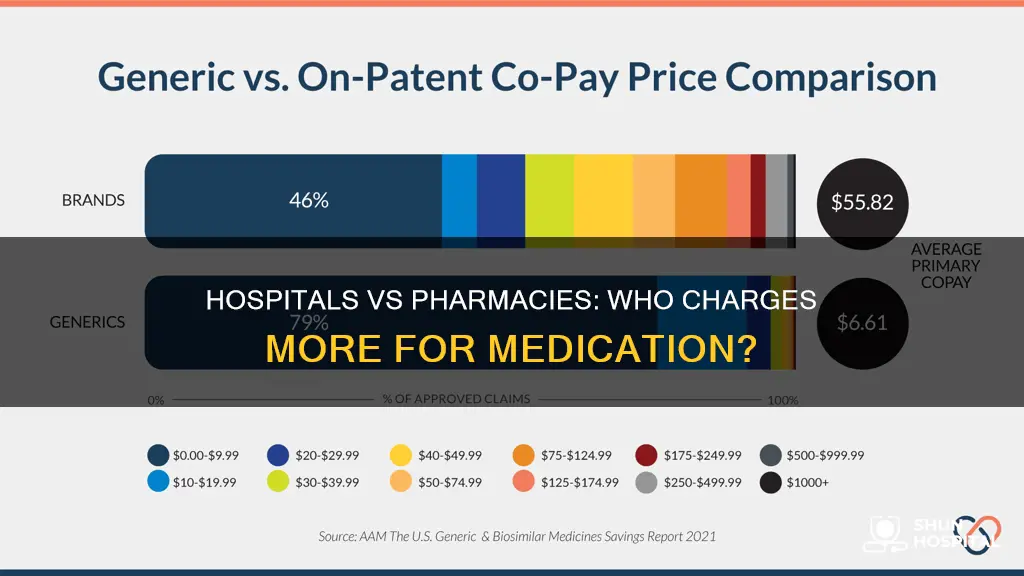
| Pharmaceutical manufacturers charge different prices | Manufacturers of brand-name drugs frequently charge different purchasers different prices for the same product. |
| Hospitals vs pharmacies | Hospitals pay on average 9% less than retail pharmacies for top-selling outpatient drugs. |
| Hospitals and insurers | Hospitals can retain a substantial share of insurer pharmaceutical expenditures. |
| Discounts and rebates | Manufacturers offer discounts and rebates on brand-name drugs based on volume and the purchaser's ability to influence market share. |
| Insured vs uninsured | Uninsured people pay the most for prescription drugs. |
| Pharmacy benefit managers (PBMs) | PBMs negotiate prices with health insurers and pharmacies, contributing to the costs paid by health consumers. |
| Cost-saving strategies | Strategies to reduce drug costs include checking formularies, splitting pills, comparing prices, and prescription drug discount programs. |
Explore related products


![Prime Screen [5 Pack] 6 Panel Urine Drug Test Kit (THC-Marijuana, BZO-Benzos, MET-Meth, OPI, AMP, COC), WDOA-264](https://m.media-amazon.com/images/I/71hU5zzuEaL._AC_UL320_.jpg)
![[5 pack] Prime Screen 14 Panel Urine Drug Test Cup - Instant Testing Marijuana (THC),OPI,AMP, BAR, BUP, BZO, COC, mAMP, MDMA, MTD, OXY, PCP, PPX, TCA](https://m.media-amazon.com/images/I/71cI114sLUL._AC_UL320_.jpg)


What You'll Learn
![]()
Hospitals' ability to influence market share
Hospitals have significant influence over the market share in the pharmaceutical industry. They are the intermediary between the buyers and sellers of drugs and can retain a large share of insurer pharmaceutical expenditures. This is due to their ability to negotiate higher commercial prices as their market share increases. This is known as the hospital's bargaining power, and it is influenced by the market share of the health system rather than individual hospitals. The market share of a health system is calculated by dividing the total number of beds in a given market by the total number of beds across all hospitals in the same market.
Hospital system consolidation has resulted in highly concentrated markets, allowing hospitals to leverage their market power to demand higher reimbursement prices from insurers. This is particularly evident in the case of specialized cancer hospitals, which are eligible for significant discounts on drug acquisition prices under the federal 340B Drug Pricing Program. Additionally, pharmacy chains and pharmacy benefit managers (PBMs) divert a significant portion of spending on patient-administered drugs, further impacting the market dynamics.
The complex nature of the pharmaceutical supply and financing chain adds to the hospitals' ability to influence market share. The process involves raw ingredient suppliers, manufacturers, wholesalers, and dispensing pharmacies, each contributing to the final price of prescription medications. Wholesalers, for instance, receive discounts for bulk purchases from manufacturers and then mark up the prices before selling to hospitals or retail pharmacies. This multi-layered system makes it challenging to implement effective policies to address high drug prices.
Furthermore, the concentration of private insurers in local markets also plays a role in hospital pricing. While economic theory suggests that insurer concentration should lead to lower prices, the interplay between insurer and provider concentration is not yet fully understood. The dynamics between these market forces influence the prices paid for healthcare services, including prescription drugs.
Overall, hospitals' ability to influence market share is significant, and it is shaped by their position in the pharmaceutical supply chain, their consolidation into large health systems, the complexity of the financing chain, and the concentration of private insurers. Understanding these dynamics is crucial for policymakers to make informed decisions and address the high and rising prices of prescription drugs.
Nyack Hospital: Dementia Unit Care and Facilities
You may want to see also
Explore related products

![Prime Screen-12 Panel Multi Drug Urine Test Compact Cup (AMP,BAR,BUP,BZO,COC,mAMP/MET,MDMA,MOP/OPI,MTD,OXY,PCP,THC) C-Cup-[2 Pack]- CDOA-6125](https://m.media-amazon.com/images/I/81wHyqSLmsL._AC_UL320_.jpg)

![[5 Pack] EZCHECK® 6-Panel Drug Test - at-Home Rapid Urine Screening Kit for 6 Most Used Drugs: (THC-Marijuana, BZO-Benzos, MET-Meth, OPI/MOP-Opiates, AMP-Amphetamine, COC)](https://m.media-amazon.com/images/I/71c1jjFYkLL._AC_UL320_.jpg)


![]()
Higher insurance reimbursements
Hospitals and pharmacies occupy different positions in the pharmaceutical supply chain. Wholesalers distribute medications to hospitals and retail pharmacies, which then dispense them to patients. Hospitals, however, can leverage their intermediary position between buyers and sellers of drugs to retain a substantial share of insurer pharmaceutical expenditures. This is achieved through markups of reimbursement prices, which are the amounts paid by insurers to hospitals and physician practices relative to the amounts paid by these providers to drug manufacturers.
A study published in the New England Journal of Medicine found that hospitals imposed large price markups and retained a substantial share of total insurer spending on physician-administered drugs for patients with private insurance. The effects were particularly pronounced for hospitals eligible for discounts under the federal 340B Drug Pricing Program on acquisition costs paid to manufacturers. The study used 2020-2021 national Blue Cross Blue Shield claims data regarding patients in the United States who had drug-infusion visits for oncologic conditions, inflammatory conditions, or blood-cell deficiency disorders.
The reimbursement prices charged by hospitals to insurers are typically higher than the acquisition prices paid by hospitals to drug manufacturers. This difference in pricing allows hospitals to retain a significant portion of insurer expenditures. Additionally, as hospitals have consolidated into large health systems, they have gained greater negotiating power, enabling them to increase the reimbursement prices they demand from insurers.
The amount hospitals receive for treating a patient depends on who is paying the bill. Private insurers negotiate prices with each hospital, and their negotiated prices are considered trade secrets. Payment structures vary, with some insurers agreeing to payments that are a percentage of a hospital's list price or Medicare reimbursements, while others negotiate specific payments for specific conditions. Private insurers tend to pay more than traditional Medicare reimbursement rates, with private Medicare Advantage plans paying an average of 10% more.
In summary, hospitals can charge higher prices for medications compared to pharmacies due to their intermediary position in the pharmaceutical supply chain and their ability to negotiate reimbursement rates with insurers. This results in higher insurance reimbursements for hospitals, allowing them to retain a substantial share of insurer pharmaceutical expenditures.
Shinji's Controversial Act: Asuka's Hospital Trauma
You may want to see also
Explore related products

$4.29 $4.99


![Prime Screen [1 Pack] 10 Panel Urine Drug Test Kit - Testing Instantly for 10 Different Drugs THC (Marijuana), BZO (Benzos), MET (Meth), PCP (Phencyclidine), MTD, AMP, BAR, COC, OPI, MDMA - WDOA-3104](https://m.media-amazon.com/images/I/81UcneTKK9L._AC_UL320_.jpg)
![[5 Pack] Prime Screen Multi Drug Urine Test Cup -6 Panel (BZO,COC,mAMP,OPI, OXY,THC) C-CUP-TDOA-564](https://m.media-amazon.com/images/I/71ZZPH0MbUL._AC_UL320_.jpg)
![Easy@Home 5 Panel Urine Drug Test Kit [15 Pack] - THC/Marijuana, Cocaine, OPI, AMP, BZO All Drugs Testing Strips in One Kit - Home Use Drug Detox Tests with Results in 5 Mins #EDOAP-754](https://m.media-amazon.com/images/I/71TJn6SkcYL._AC_UL320_.jpg)
![]()
Discounts for hospitals
Hospitals can retain a significant portion of pharmaceutical expenditures from insurers. They can increase the reimbursement prices they demand from insurers as they are the intermediary between the buyer and seller of drugs. In addition, approximately one-third of hospitals, including all specialized cancer hospitals, are eligible for substantial discounts on drug acquisition prices under the federal 340B Drug Pricing Program.
The drug supply chain involves raw ingredient suppliers, manufacturers, wholesalers, and dispensing pharmacies. Wholesalers, who purchase 92% of prescription drugs in bulk, may receive discounts from manufacturers for buying in large volumes. They then mark up the price before selling to hospitals or retail pharmacies.
The average sales price, calculated by the Centers for Medicare and Medicaid Services (CMS), is used to reimburse drugs under Medicare Part B. CMS requires manufacturers to report net revenues, taking into account discounts and rebates to insurers, wholesalers, distributors, and pharmacies. While CMS pays hospitals and physician practices the same rate for a drug, it includes an additional 6% margin to cover inventory costs.
The Inflation Reduction Act grants the federal government the authority to negotiate Medicare drug prices, aiming to reduce costs for seniors and improve health equity. Pharmacy benefit managers (PBMs) are intermediaries that negotiate with drug manufacturers and pharmacies to develop pharmacy networks for insurance plans.
Healthcare workers, including hospital employees, medical providers, nurses, and doctors, are eligible for various discounts and deals from different companies. For example, companies like DreamCloud, Ergobaby, and Brooks Running offer exclusive discounts to healthcare professionals as a token of appreciation for their dedication and service.
Hospitals Provide Peri Bottles: Why and How to Use Them
You may want to see also
Explore related products

![SAFE LIFE [25] Pack- 10 Panel Multi Drug Urine Test Cup (THC 50, AMP,BUP,BZO,COC,mAMP/MET,MDMA,MOP/OPI,MTD,OXY)-Highly Sensitive- Fast Result in 5 Mins](https://m.media-amazon.com/images/I/71xomjcy33L._AC_UL320_.jpg)
![Prime Screen [5 Pack] 5 Panel Urine Drug Test Kit - Testing Instantly for 5 Different Drugs AMP, COC, MET (Meth), OPI, THC (Marijuana) - WDOA-254](https://m.media-amazon.com/images/I/71FsDMfvdFL._AC_UL320_.jpg)

![Prime Screen [5 Pack] 12 Panel Urine Drug Test Kit (AMP, BAR, BUP, Benzos BZO, COC, mAMP, MDMA, MOP, MTD, OXY, PCP, Marijuana THC) - WDOA-6125](https://m.media-amazon.com/images/I/51jbz+-PFBL._AC_UL320_.jpg)

![]()
Pharmacy benefit managers
The role of PBMs in the pharmaceutical supply chain has come under scrutiny in recent years due to concerns about rising drug prices and instances of fraud. In one notable case, Florida pharmacy owners Peter Bolos and Michael Palso were sentenced for their roles in a multimillion-dollar healthcare fraud scheme. Bolos and Palso, along with other co-conspirators, deceived PBMs such as Express Scripts and CVS Caremark regarding tens of thousands of prescriptions. The PBMs processed and approved claims for prescription drugs on behalf of insurance companies, including private insurers such as Blue Cross Blue Shield of Tennessee and public insurers such as Medicaid and TRICARE. The co-conspirators defrauded the PBMs into authorizing millions of dollars' worth of claims, resulting in significant financial losses for the insurance companies.
Instances of fraud involving PBMs are not isolated incidents. In another case, Larry Smith and others were charged with a nationwide conspiracy to defraud PBMs out of $174,202,105 by submitting fraudulent bills for prescriptions purchased from a telemarketing company. Smith admitted to conspiring with multiple individuals and companies to defraud PBMs into paying for fraudulent prescriptions for topical pain creams, vitamins, and other products.
The issue of rising drug prices in the United States has prompted calls for increased PBM transparency and regulatory interventions to address the complexity of the pharmaceutical supply and financing chain. The Inflation Reduction Act, for example, grants the federal government new authority to negotiate Medicare drug prices, which is expected to generate significant savings over time.
In summary, pharmacy benefit managers are key intermediaries in the pharmaceutical supply chain, and their actions can have significant implications for drug pricing and healthcare costs. While instances of fraud involving PBMs have led to legal consequences, there is a growing recognition that a more holistic and comprehensive approach is needed to address the underlying issues of high and rising prescription drug prices in the United States.
Improving Hospital Quality with ACOs
You may want to see also
Explore related products





![]()
The role of wholesalers
Wholesalers are a critical component of the pharmaceutical supply chain, acting as intermediaries between manufacturers and dispensing pharmacies, hospitals, clinics, and other healthcare facilities. They purchase prescription drugs in bulk from manufacturers, store them, and then sell and distribute them to their clients. This process involves setting prices, managing inventory, and coordinating product shipment.
In the United States, wholesalers play a significant role in the distribution of prescription medications, with approximately 92% of prescription drugs passing through their hands before reaching pharmacies and other dispensers. This central role grants them considerable influence over drug pricing, particularly in the case of generic drugs, where they actively contribute to price setting. Wholesalers also benefit from list price increases, compete in specialty drug distribution, and can mitigate or exacerbate drug shortages.
The average wholesale price (AWP) is a key metric in drug cost calculation, representing the price pharmacies pay to wholesalers for drug products. The average wholesale price is often used as a benchmark for reimbursement rates by state Medicaid programs, which employ the estimated acquisition cost (EAC) to reimburse pharmacies for the cost of the drug plus a dispensing fee. However, the actual cost paid by pharmacies to wholesalers, after accounting for all discounts, is reflected in the average actual cost (AAC).
Wholesalers also play a role in the distribution of infused drugs, which are administered by physicians in hospitals or clinics. In this context, manufacturers and their wholesalers sell directly to hospitals and physician practices, which then negotiate discounts with manufacturers to reduce the amount paid. The difference between the reimbursement price from insurers and the acquisition price paid to manufacturers constitutes revenue for the provider organization.
Trupanion Insurance: Is It Accepted at Oradell Animal Hospital?
You may want to see also
Frequently asked questions
Hospitals can leverage their position as intermediaries between drug buyers and sellers to retain a substantial share of insurer pharmaceutical expenditures. They have been known to increase the reimbursement prices they demand from insurers. However, hospitals also purchase drugs from distributors, and they pay, on average, 9% less than retail pharmacies.
There are several reasons for the high cost of prescription drugs. Firstly, pharmaceutical manufacturers of brand-name drugs often charge different prices to different purchasers for the same product. Secondly, pharmacy benefit managers (PBMs), who negotiate prices with health insurers and pharmacies, contribute to higher costs due to their fees and incentives. Additionally, insurers have been shifting costs to patients through higher copays, deductibles, and premiums.
The cost of prescription drugs is influenced by various factors, including the raw material and manufacturing costs, distribution and wholesale markups, and the involvement of intermediaries such as PBMs. Additionally, the size of discounts and rebates can impact the final price, with larger discounts given for higher volumes purchased and the ability to influence market share.
Consumers can take several steps to reduce their prescription drug costs. They can check the list of preferred medications (the formulary) offered by their health insurance, which tend to be more affordable. In some cases, splitting pills or opting for a higher dosage that can be divided into smaller doses may result in cost savings. Additionally, comparing prices at different pharmacies and exploring prescription drug discount programs can help identify more affordable options.
Efforts are being made to address the high cost of prescription drugs. The Inflation Reduction Act grants the federal government the authority to negotiate Medicare drug prices, which is projected to generate significant savings over time. Policymakers are also incorporating private sector purchasing techniques into proposals to extend drug benefits to Medicare beneficiaries. Additionally, there is a push for greater transparency in the operations of PBMs and limitations on their practices to control drug pricing.


![Prime Screen [5 Pack] 10 Panel Urine Drug Test Kit - Testing Instantly for THC (Marijuana), BZO (Benzos), MET (Meth), PCP (Phencyclidine), MTD, AMP, BAR, COC, OPI, MDMA - WDOA-3104](https://m.media-amazon.com/images/I/71MI2Y3yIRL._AC_UL320_.jpg)
![Prime Screen 12 Panel Multi Drug Urine Drug Test Card (AMP,BAR,BZO,COC,mAMP,MDMA,MOP/OPI 300,MTD,OXY,PCP,TCA,THC) - WDOA-7125 [1 Pack]](https://m.media-amazon.com/images/I/81tgsharFcL._AC_UL320_.jpg)



![Prime Screen 12 Panel Drug Test Kit - Instant Urine Testing Marijuana(THC),AMP,BAR,BZO,COC,mAMP,MDMA,MOP/OPI 300 Cut-Off Level,MTD,OXY,PCP,TCA -TDOA-7125 [5 Pack]](https://m.media-amazon.com/images/I/71oTnSSHRaL._AC_UL320_.jpg)


![PrimeScreen - [5 Pack] 5 Panel Urine Drug Test - Marijuana (THC),Cocaine (COC),Opiate (OPI 2000),Benzodiazepines (BZO),Methamphetamine (MET) WDOA-654](https://m.media-amazon.com/images/I/615xqvfSh-L._AC_UL320_.jpg)

![[25 Pack] U-CATCH Plus Multi-Drug Test Kit for All: 12 Panel Urine Test Cup Rapid Drug Test at Home for Marijuana(THC),AMP,BAR,BUP,BZO,COC,MDMA,MET,MOP,MTD,OXY,PCP](https://m.media-amazon.com/images/I/61R3c9ksLLL._AC_UL320_.jpg)