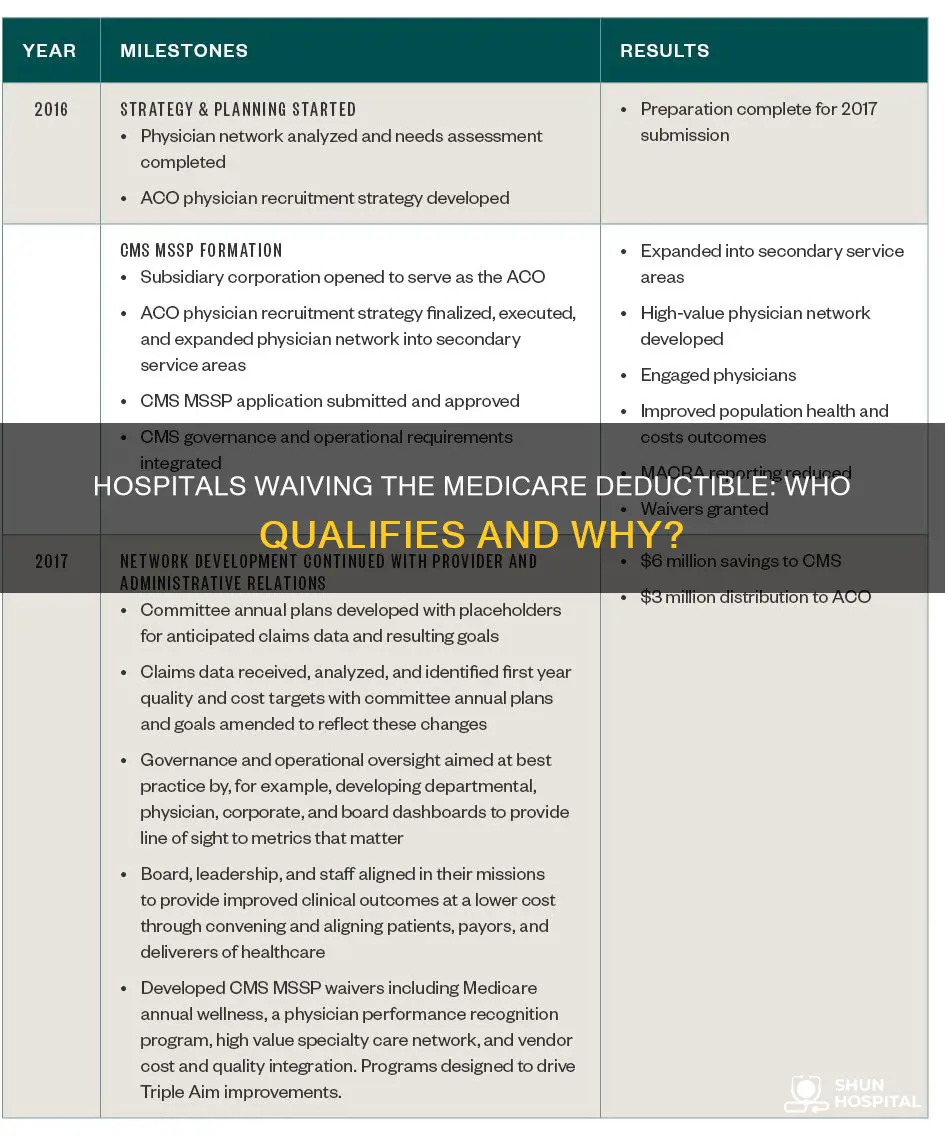
Medicare is undergoing significant changes in 2025, with updates to prescription drug plans, premiums, deductibles, and expanded coverage for services and drugs. However, the question of whether hospitals waive the $20 Medicare fee remains unclear. While Medicare historically underpaid hospitals, new data from 2022 shows that Medicare payments hit record lows, with Medicare paying just 82 cents for every dollar spent by hospitals. This has resulted in significant underpayments, impacting hospitals' ability to provide care. Medicare prescription drug plans and coverage for specific treatments, such as anti-obesity medications, are also important considerations. Understanding the evolving landscape of Medicare and its impact on healthcare providers and patients is essential for making informed decisions about healthcare coverage and expenses.
| Characteristics | Values |
|---|---|
| Medicare payments to hospitals | Record lows in 2022 |
| Medicare payment levels in 2022 | 82 cents for every dollar spent by hospitals |
| Medicare underpayments in 2022 | $99.2 billion |
| Medicare and Medicaid inpatient days | 50% of inpatient days in 96% of hospitals |
| Medicare and Medicaid inpatient days | 67% of inpatient days in over 82% of hospitals |
| Medicare underpayments in 2022 | $130 billion |
| Medicare underpayments in 2019 | $76 billion |
| Medicare Part A deductible | $1,676 |
| Medicare Part A coinsurance for days 61-90 | $419 per day |
| Medicare Part A coinsurance for lifetime reserve days | $838 per day |
| Medicare Part A premium | $285 per month |
| Medicare Part B premium | $185 per month |
| Medicare Part B deductible | $257 per year |
| Medicare Part D drug costs limit | $2,000 |
| Prescription drug coverage gap | Eliminated |
| Prescription payment plan | Opt-in |
Explore related products






What You'll Learn
![]()
Hospitals are underpaid by Medicare
Hospitals are increasingly feeling the strain of underpayment by Medicare and Medicaid. The American Hospital Association (AHA) has reported that in 2022, Medicare paid just 82 cents for every dollar spent by hospitals caring for patients—a record low. This resulted in a staggering $99.2 billion in Medicare underpayments for that year alone, a significant increase from the $76 billion in combined underpayments by Medicare and Medicaid in 2019.
Medicare payments are set by law rather than through a negotiation process, as with private insurers. This means that hospitals are unable to negotiate reimbursement rates, which are often below the cost of providing care. In fact, 94% of hospitals have half or more of their inpatient days paid for by public payers, and 96% of hospitals have 50% of their inpatient days paid by Medicare and Medicaid. This has put hospitals in an extremely difficult position, as they are unable to absorb the inflationary pressures they are currently facing.
The underpayment crisis is further exacerbated by the fact that Medicare and Medicaid account for more than 60% of all care provided by hospitals. As a result, very few hospitals can choose not to participate in these programs. Hospitals are required to care for Medicare and Medicaid beneficiaries as a condition for receiving federal tax exemption for providing healthcare to the community.
The AHA has urged policymakers to address this issue, as the underpayment of hospitals by Medicare and Medicaid is severely threatening access to care for patients and communities. The underpayment crisis has also contributed to skyrocketing hospital administrative costs and burdensome commercial insurer policies, which further impact patient care.
It is clear that the underpayment of hospitals by Medicare is a significant issue that needs to be addressed. Without action from policymakers, the sustainability of hospitals and access to care for patients are at risk.
Hospitals and DNA Testing: Pre-Mortem Options
You may want to see also
Explore related products






![]()
Hospitals are unable to absorb inflationary costs
While it is unclear if most hospitals waive the $20 Medicare fee, it is evident that hospitals are struggling to keep up with the costs of patient care. Medicare and Medicaid account for most hospital utilization, with 96% of hospitals having 50% of their inpatient days paid for by these public payers. Medicare consistently underpays hospitals, and the gap appears to be widening. In 2022, Medicare paid just 82 cents for every dollar spent by hospitals caring for Medicare patients, resulting in $99.2 billion in underpayments for that year alone. This underpayment occurs when the payment received is less than the costs of providing care, including personnel, technology, and other goods and services.
The Medicare Payment Advisory Commission's data projects that hospitals will continue to face financial strain, with margins remaining near -13% in 2024. Combined underpayments from Medicare and Medicaid to hospitals were nearly $130 billion in 2022, a significant increase from $76 billion in 2019. This underpayment crisis puts access to care for patients and communities at risk. Hospitals are unable to absorb the inflationary costs, and without action from policymakers, the situation will only worsen.
Healthcare spending has been increasing, and hospitals are facing rising administrative costs and the burden of commercial insurer policies. While data on healthcare price increases is not comprehensive due to government staffing shortages, it is clear that healthcare prices continue to rise, outpacing inflation. This gap between healthcare price increases and inflation further exacerbates the financial strain on hospitals, making it even more challenging for them to absorb inflationary costs.
The impact of inflation extends beyond hospitals, affecting the lives of everyday Americans. Inflation data is closely monitored by the Federal Reserve to set interest rates, which, in turn, influence borrowing costs for families and businesses. Accurate inflation data is crucial for making informed decisions and adjustments to government programs such as Social Security. However, staffing shortages have led to reduced data gathering, potentially compromising the accuracy of inflation measurements and subsequent policy decisions.
Hospital Workers: The Importance of Daily Showers
You may want to see also
Explore related products






![]()
Medicare Part A deductible increases
The Medicare Part A deductible has been steadily increasing over the years. For 2025, the Part A inpatient hospital deductible that beneficiaries pay if admitted to the hospital will be $1,676, an increase of $44 from $1,632 in 2024. This covers the beneficiary's share of costs for the first 60 days of Medicare-covered inpatient hospital care in a benefit period. The annual deductible for all Medicare Part B beneficiaries will be $257 in 2025, an increase of $17 from the annual deductible of $240 in 2024. The standard monthly premium for Medicare Part B enrollees will be $185.00 for 2025, an increase of $10.30 from $174.70 in 2024.
The increase in the 2025 Part B standard premium and deductible is mainly due to projected price changes and assumed utilization increases. The Part A deductible increase from 2023 to 2024 was $32, with the amount rising from $1,600 to $1,632. From 2022 to 2023, the increase was even higher at $100, with the deductible rising from $1,500 to $1,600.
Individuals who had at least 30 quarters of coverage, or were married to someone with at least 30 quarters of coverage, may buy into Part A at a reduced monthly premium rate, which will be $285 in 2025, a $7 increase from 2024. Certain uninsured older individuals who have fewer than 30 quarters of coverage and certain individuals with disabilities who have exhausted other entitlements will pay the full premium, which will be $518 a month in 2025, a $13 increase from 2024.
While Medicare Part A deductible increases may seem incremental, they are part of a broader context of Medicare underpayments to hospitals. According to the American Hospital Association (AHA), Medicare consistently reimburses hospitals below the cost of providing care to patients. In 2022, Medicare paid just 82 cents for every dollar spent by hospitals caring for Medicare patients, resulting in a staggering $99.2 billion in underpayments that year. This underpayment gap has widened over time, nearly tripling since 2012.
The Medicare Payment Advisory Commission's projections indicate that hospitals will continue to face financial pressures due to Medicare reimbursement rates, with margins expected to remain near -13% in 2024. Combined underpayments from Medicare and Medicaid to hospitals reached nearly $130 billion in 2022, a significant increase from $76 billion in 2019. These underpayments have severe implications for hospitals, threatening access to care for patients and communities.
Understanding Medicare and Medicaid Hospital Reimbursement
You may want to see also
Explore related products





![Medicare and Social Security: [5 in 1] Maximize Your Retirement Benefits, Secure Medical Coverage and Quality Healthcare | Proven Strategies to Protect Your Financial Future Avoiding Costly Mistakes](https://m.media-amazon.com/images/I/71sRJGiWeQL._AC_UL320_.jpg)
![]()
Medicare prescription drug plans don't cover anti-obesity medications
Medicare prescription drug plans, also known as Part D, cover a wide range of drugs to ensure that people with different medical conditions can access the prescription drugs they need. However, it's important to note that Medicare drug plans do not currently cover anti-obesity medications.
The Biden administration has proposed to allow Medicare to cover anti-obesity medications by reinterpreting the statutory language that currently prohibits coverage of drugs used solely for weight loss. This proposal reflects a shift in understanding obesity as a disease and acknowledges the health benefits of weight loss for people with obesity. The proposal would increase access to anti-obesity treatments for Medicare enrollees with obesity, addressing a long-standing gap in coverage.
Currently, people on Medicare can only get anti-obesity drugs covered by Part D if they are used for medically accepted FDA-approved indications other than obesity. For example, certain drugs may be covered for diabetes or cardiovascular disease risk reduction, but not specifically for weight loss. This limitation has been a source of contention, with lawmakers in Congress repeatedly introducing legislation to authorize Medicare coverage of anti-obesity drugs.
The potential cost implications of covering anti-obesity drugs under Medicare have been a significant consideration. The proposal is expected to increase Medicare spending by $25 billion over ten years, and the combination of high demand, new uses, and high prices for these treatments will likely impact Part D plan costs and premiums over time. However, the true cost to Medicare may be lower than estimated, as some people with obesity may already have coverage for these drugs for other medically accepted indications.
While the proposed expansion of coverage for anti-obesity drugs in Medicare is a positive step towards improving access to care, it's important to recognize that Medicare reimbursement rates for hospitals are often below the cost of providing care. This underpayment issue has been exacerbated by the fixed nature of Medicare payments, making it challenging for hospitals to cope with inflationary pressures. Policymakers need to address this crisis of government underpayment to ensure that access to care for patients and communities is not compromised.
Hospitals: CMS Regulations and Compliance Standards
You may want to see also
Explore related products






![]()
Medicare inpatient hospital services
Medicare Part A covers inpatient hospital care, including critical access hospitals and skilled nursing facilities. The coverage includes semi-private rooms and meals. The number of days covered and the out-of-pocket costs differ depending on the number of days spent in the hospital. For the first 60 days, there is no cost after meeting the Part A deductible of $1,676. Days 61-90 cost $419 each day, and days 91 onwards cost $838 each day for each lifetime reserve day, up to a maximum of 60 reserve days over your lifetime. After exhausting the lifetime reserve days, patients are responsible for all costs.
Inpatient hospital admission is a complex medical decision based on the doctor's judgment and the patient's need for medically necessary hospital care. Generally, inpatient admission is appropriate when the patient is expected to require two or more midnights of medically necessary hospital care. Hospitals are required to share the standard charges for their items and services on a public website to help patients make informed decisions about their care.
Medicare Part A also covers inpatient mental health care in freestanding psychiatric hospitals, but this is limited to up to 190 days during the patient's lifetime. However, this limit does not apply to care received in a Medicare-certified distinct part psychiatric unit within an acute care or critical access hospital.
While Medicare covers inpatient hospital services, it is important to note that Medicare consistently underpays hospitals for the care of patients. According to data from the American Hospital Association (AHA), Medicare paid just 82 cents for every dollar spent by hospitals on Medicare patients in 2022, resulting in a significant underpayment of $99.2 billion for that year. This underpayment poses challenges to hospitals and health systems that depend on public payers like Medicare and Medicaid, potentially impacting access to care for patients and communities.
Alcohol Detox: Hospital Treatment and Recovery Process
You may want to see also











![The Medicare Bible for Beginners: [3 in 1] Unlock Medical Benefits and Quality Healthcare | Super Easy Insider Strategies to Navigate Medicare While Avoiding Costly Mistakes](https://m.media-amazon.com/images/I/71tm-tSiWnL._AC_UL320_.jpg)