The question of whether most people die at home or in a hospital is a significant one, reflecting broader trends in healthcare, societal preferences, and end-of-life care practices. Historically, home deaths were more common, but with advancements in medical technology and the aging population, hospital deaths have become prevalent in many countries. However, recent shifts toward palliative care and patient-centered approaches have renewed interest in home-based end-of-life care, raising questions about current patterns and future directions. Understanding where most people die is crucial for improving care systems, allocating resources, and ensuring individuals’ preferences are respected in their final moments.
| Characteristics | Values |
|---|---|
| Preferred Place of Death | Home (increasing trend in many countries) |
| Actual Place of Death | Hospital (still the most common, but declining in some regions) |
| Percentage Dying at Home | Varies by country: ~20-30% in the US, ~50% in the UK (2020s data) |
| Percentage Dying in Hospital | ~50-60% in the US, ~30-40% in the UK (2020s data) |
| Factors Influencing Location | Age, disease type, availability of palliative care, cultural norms |
| Trends Over Time | Shift toward home deaths due to improved palliative care services |
| Regional Differences | Higher home deaths in countries with strong palliative care systems |
| Impact of COVID-19 | Increased hospital deaths during peaks, but home deaths remained steady or increased in some areas |
| Demographic Variations | Older adults more likely to die at home; younger individuals in hospitals |
| Cost Implications | Home deaths often less costly than prolonged hospital stays |
Explore related products






What You'll Learn
- Home Deaths Trends: Analyzing recent statistics on the rise of home deaths vs. hospital deaths
- Cultural Preferences: How cultural norms influence where people prefer to die
- Medical Conditions: Which illnesses lead to more home or hospital deaths
- Palliative Care Impact: Role of palliative care in increasing home deaths
- Age and Location: How age and geographic location affect place of death
![]()
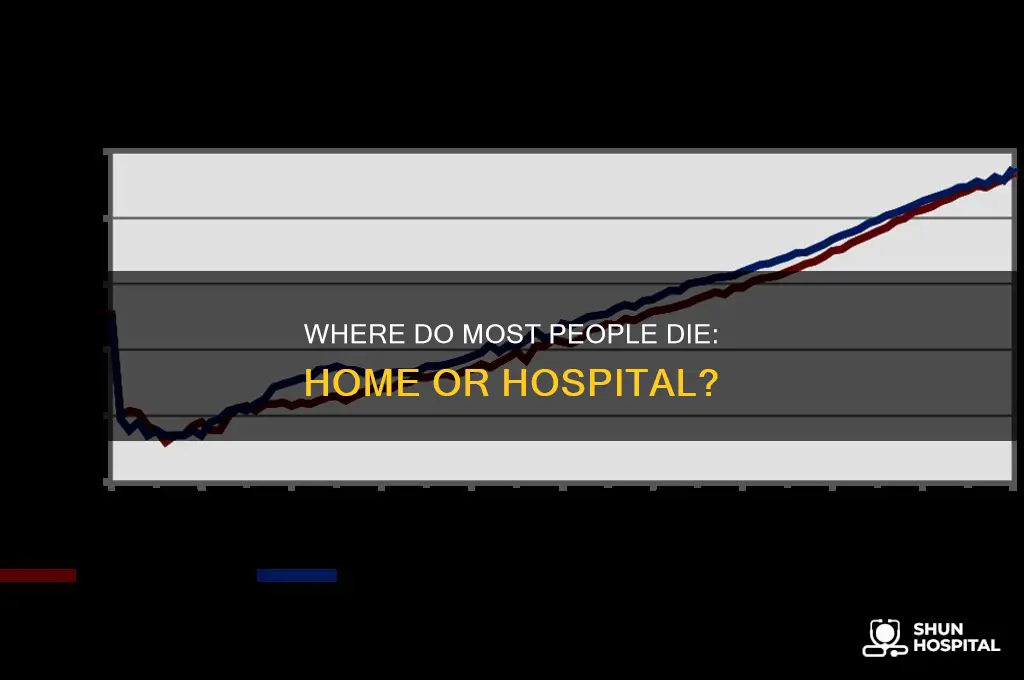
Home Deaths Trends: Analyzing recent statistics on the rise of home deaths vs. hospital deaths
Recent trends in end-of-life care reveal a notable shift toward home deaths, challenging the long-standing dominance of hospital deaths. Historically, hospitals have been the primary place of death, but recent statistics indicate a growing preference for dying at home. According to a 2021 study published in the *Journal of Palliative Care*, the proportion of home deaths in countries like the United States, the United Kingdom, and Canada has increased steadily over the past decade. This shift is driven by factors such as advancements in home-based medical care, the rise of palliative care services, and a cultural reevaluation of end-of-life preferences.
One key factor contributing to the rise in home deaths is the expansion of palliative and hospice care services. These programs provide comprehensive support for patients and families, enabling more people to manage terminal illnesses in the comfort of their own homes. For instance, data from the Centers for Disease Control and Prevention (CDC) shows that hospice care utilization in the U.S. has nearly doubled since 2000, with a significant portion of hospice patients opting to remain at home. This trend aligns with surveys indicating that a majority of individuals express a desire to die at home if given the choice, highlighting the importance of patient-centered care.
Despite the rise in home deaths, hospitals remain the most common place of death in many regions, particularly for sudden or acute conditions. However, the gap is narrowing. In the U.K., for example, the Office for National Statistics reported that home deaths surpassed hospital deaths for the first time in 2020, a trend accelerated by the COVID-19 pandemic. The pandemic forced many families to reconsider end-of-life care options, with restrictions on hospital visits prompting a shift toward home-based care. This period underscored the feasibility and benefits of home deaths when adequate support is available.
Demographic and cultural shifts also play a role in these trends. Aging populations in many countries are increasing the demand for end-of-life care, with older adults often preferring to spend their final days in familiar surroundings. Additionally, cultural attitudes toward death and dying are evolving, with a greater emphasis on quality of life and personal autonomy. In countries like Japan and the Netherlands, where home deaths have been more common, cultural norms and robust community support systems have long facilitated this preference.
Moving forward, policymakers and healthcare providers must address challenges to sustain the rise in home deaths. These include ensuring equitable access to palliative care, training healthcare professionals in home-based care, and providing financial support for families. As the trend continues, understanding and responding to the factors driving home deaths will be crucial in reshaping end-of-life care to better meet the needs and preferences of patients and their families. The shift from hospital to home deaths represents not just a statistical change but a profound transformation in how societies approach the end of life.
Providence Hospital Southfield MI: Location, Directions, and Access Guide
You may want to see also
Explore related products






![]()
Cultural Preferences: How cultural norms influence where people prefer to die
Cultural preferences play a significant role in determining where individuals prefer to spend their final moments, whether at home or in a hospital. These preferences are deeply rooted in societal norms, family structures, and spiritual beliefs that vary widely across different cultures. For instance, in many Western countries, there has been a growing trend toward home-based end-of-life care, often driven by the desire for familiarity, comfort, and family presence. This shift is supported by advancements in palliative care services that enable individuals to receive medical support at home. Conversely, in cultures where healthcare systems are more centralized or where hospitals are seen as the most reliable source of care, dying in a medical facility is often the preferred or default option.
In many Asian cultures, such as in Japan and China, dying at home is traditionally considered more respectful and aligned with familial duties. The concept of filial piety emphasizes the importance of family care, and many believe that allowing a loved one to pass away at home is a final act of devotion. However, urbanization and changing family dynamics have led to a gradual increase in hospital deaths, as younger generations may lack the resources or time to provide round-the-clock care at home. Despite this shift, cultural values still heavily influence the preference for home-based end-of-life care in these societies.
In contrast, some cultures prioritize medical intervention and view hospitals as the most appropriate place for death. For example, in the United States, the emphasis on advanced medical technology and the belief in prolonging life often lead to a higher prevalence of hospital deaths. This preference is also influenced by the fear of inadequate pain management or complications that might arise at home. Similarly, in parts of Europe, such as Germany, the preference for hospital deaths is tied to the trust in the healthcare system and the expectation of professional medical care during the final stages of life.
Religious beliefs also intersect with cultural norms to shape preferences for the place of death. In many Islamic cultures, for instance, dying at home is preferred to ensure that the individual is surrounded by family and can receive the proper religious rites and prayers. Similarly, in Hindu traditions, dying at home is often seen as essential for a peaceful transition to the afterlife, as it allows for the performance of specific rituals. These spiritual considerations can override practical concerns, such as access to medical care, and reinforce the cultural preference for home-based end-of-life care.
Ultimately, understanding cultural preferences requires recognizing the complex interplay between tradition, family values, healthcare infrastructure, and personal beliefs. Policymakers and healthcare providers must consider these factors when designing end-of-life care services to ensure they align with the diverse needs and preferences of different cultural groups. By respecting and accommodating cultural norms, societies can support individuals in dying in a place that feels most dignified and meaningful to them, whether that be at home or in a hospital.
Chicago Hospital's Recent Event: Unveiling the Latest Developments and Impact
You may want to see also
Explore related products






![]()
Medical Conditions: Which illnesses lead to more home or hospital deaths
The question of where people are more likely to die—at home or in a hospital—often depends on the nature of their medical condition. Certain illnesses are more likely to result in hospital deaths due to their acute or complex nature, while others may allow individuals to remain at home, especially with proper palliative care. Understanding these patterns can help families and healthcare providers plan for end-of-life care more effectively.
Acute Conditions Leading to Hospital Deaths: Medical conditions that require immediate and intensive intervention, such as severe heart attacks, strokes, or traumatic injuries, are more likely to result in hospital deaths. These conditions often necessitate emergency procedures, surgeries, or critical care that can only be provided in a hospital setting. For example, a ruptured aneurysm or a severe pulmonary embolism typically leads to hospitalization and a higher likelihood of dying in the hospital due to the urgent and life-threatening nature of these events.
Chronic Illnesses and Home Deaths: In contrast, many chronic illnesses, such as advanced heart failure, chronic obstructive pulmonary disease (COPD), or end-stage renal disease, often allow individuals to spend their final days at home, especially if they have access to palliative care or hospice services. These conditions progress gradually, and with proper symptom management, patients can remain comfortable at home. Studies show that many people with advanced cancer also prefer to die at home, and with adequate support, this preference can often be honored, leading to a higher proportion of home deaths for these conditions.
Infectious Diseases and Variability: The place of death for infectious diseases can vary widely depending on the specific illness and healthcare infrastructure. For instance, during the COVID-19 pandemic, many deaths occurred in hospitals due to the need for intensive respiratory support. However, in regions with robust community healthcare systems, some individuals with COVID-19 or other infectious diseases were able to receive end-of-life care at home. This highlights the importance of healthcare resources and patient preferences in determining the place of death.
Neurodegenerative Diseases and Home Care: Conditions like Alzheimer’s disease, Parkinson’s disease, and other neurodegenerative disorders often result in home deaths, particularly in the later stages. These illnesses progress slowly, and patients frequently require long-term care that can be provided at home by family members or caregivers. Hospice services play a crucial role in supporting these patients, enabling them to remain in a familiar environment during their final days.
Pediatric and Rare Conditions: For children with life-limiting conditions, such as certain genetic disorders or cancers, the place of death can vary. Some families opt for hospital-based care to ensure access to specialized treatments, while others prefer home-based palliative care to provide a more comfortable and familiar setting. Rare diseases may also influence the place of death, depending on the availability of specialized care and the progression of the illness.
In summary, the likelihood of dying at home or in a hospital is closely tied to the specific medical condition and its management. Acute and complex illnesses often lead to hospital deaths, while chronic and progressive diseases more frequently result in home deaths, especially with adequate palliative care support. Understanding these patterns can help individuals and families make informed decisions about end-of-life care.
Magnet Program: Hospitals' Ultimate Recognition
You may want to see also
Explore related products






![]()
Palliative Care Impact: Role of palliative care in increasing home deaths
Palliative care plays a pivotal role in reshaping the landscape of end-of-life care, particularly in increasing the likelihood of individuals dying at home rather than in a hospital setting. Historically, hospitals have been the most common place of death, often due to the perceived need for medical intervention during the final stages of life. However, research indicates that a significant proportion of people express a preference to spend their last days at home, surrounded by familiar environments and loved ones. Palliative care addresses this desire by providing comprehensive support that enables patients to remain at home comfortably and safely. Through symptom management, emotional support, and coordination of care, palliative care teams empower patients and families to navigate the challenges of end-of-life care outside of hospital walls.
One of the key impacts of palliative care is its ability to manage symptoms effectively, reducing the need for hospital admissions. Many patients nearing the end of life experience pain, shortness of breath, anxiety, or other distressing symptoms that can be alleviated through specialized palliative care interventions. By offering tailored treatments and medications, palliative care professionals ensure that patients can remain at home without suffering unnecessarily. This proactive approach not only improves quality of life but also minimizes crises that might otherwise lead to hospitalization. Studies have shown that access to palliative care is associated with fewer hospital deaths and a higher proportion of home deaths, reflecting its success in aligning care with patient preferences.
Another critical aspect of palliative care is its focus on advance care planning and patient-centered decision-making. Palliative care teams engage patients and families in conversations about goals of care, preferences for treatment, and end-of-life wishes early in the care process. This ensures that care plans are aligned with the patient’s values and desires, including the wish to die at home. By fostering open communication and providing education about the dying process, palliative care reduces the fear and uncertainty that often drive hospital admissions. Families, too, are better prepared to care for their loved ones at home when supported by palliative care professionals who offer guidance, respite, and emotional support.
The integration of community-based palliative care services further enhances the likelihood of home deaths. These services, often delivered by multidisciplinary teams including nurses, physicians, social workers, and volunteers, bring specialized care directly to the patient’s home. This model ensures continuity of care and reduces the logistical and emotional burdens associated with hospital visits. Additionally, community palliative care programs often collaborate with primary care providers and other healthcare services to create a seamless support network. This holistic approach addresses not only the medical needs of the patient but also the social, emotional, and spiritual aspects of end-of-life care, making home-based care a viable and preferred option.
Finally, the impact of palliative care on increasing home deaths is evident in its ability to provide 24/7 support and crisis management. Many palliative care programs offer round-the-clock access to healthcare professionals who can address urgent concerns and prevent emergencies that might necessitate hospital admission. This level of responsiveness reassures patients and families that they are not alone, even in the most challenging moments. By offering this safety net, palliative care fosters confidence in home-based care, enabling more people to die in the place they find most comforting. In this way, palliative care not only honors individual preferences but also transforms the end-of-life experience, making home deaths a more achievable and dignified reality.
Hospitals' Ethical Dilemma: Faulty Deaths and Legal Consequences
You may want to see also
Explore related products






![]()
Age and Location: How age and geographic location affect place of death
The question of where people spend their final moments—whether at home or in a hospital—is deeply influenced by age and geographic location. As individuals age, their health needs often become more complex, leading to a higher likelihood of dying in a hospital setting. Older adults, particularly those over 75, are more prone to chronic illnesses, acute conditions, and emergencies that require immediate medical intervention. Hospitals are equipped to handle these situations, making them a common place of death for the elderly. However, cultural and personal preferences also play a role; in some regions, families prioritize home-based care for their elderly relatives, even in the final stages of life.
Geographic location significantly shapes the accessibility of healthcare resources and end-of-life care options, which in turn affects where people die. In urban areas, where hospitals and specialized care facilities are more readily available, deaths in hospitals are more common. Rural populations, on the other hand, often face challenges such as limited access to medical facilities, longer travel times, and fewer palliative care services. As a result, rural residents may be more likely to die at home, either by choice or due to the impracticality of reaching a hospital in time. Additionally, rural areas often have stronger community and family support systems, which can facilitate home-based end-of-life care.
Cultural and socioeconomic factors tied to geographic location also influence place of death. In regions with strong traditions of family-centered care, such as parts of Asia and Southern Europe, dying at home is often preferred and culturally valued. Conversely, in societies where medicalization of death is more accepted, such as North America and Northern Europe, hospital deaths are more prevalent. Socioeconomic status further complicates this dynamic; individuals in lower-income areas may lack access to home-based palliative care services, increasing the likelihood of hospital deaths. Wealthier regions, with better access to resources, may see a higher proportion of home deaths due to the availability of private care options.
Age and location intersect in ways that further determine end-of-life settings. For instance, younger individuals who die, often due to accidents or sudden illnesses, are more likely to die in hospitals regardless of location, as these events typically require emergency medical attention. In contrast, older adults in rural areas may choose or default to home deaths due to the challenges of accessing hospital care. Urban elderly populations, however, might still lean toward hospital deaths due to the proximity of medical facilities and the complexity of their health needs. These patterns highlight the need for tailored end-of-life care strategies that consider both age-related health requirements and regional resources.
Ultimately, the interplay between age and geographic location reveals a nuanced picture of where people die. While hospitals remain a common place of death, particularly for the elderly and those in urban areas, home deaths are more prevalent in rural regions and cultures that prioritize family-centered care. Addressing this issue requires expanding access to palliative care services, improving healthcare infrastructure in underserved areas, and respecting individual and cultural preferences for end-of-life care. By understanding these dynamics, societies can work toward ensuring that people die in the settings that align with their needs and wishes, whether at home or in a hospital.
Understanding PPO Networks: Doctors and Hospitals Available to Members
You may want to see also
Frequently asked questions
Most people die in hospitals, though the preference for home-based end-of-life care is increasing in many countries.
Statistics vary by country, but in the U.S., about 30% of deaths occur at home, while approximately 60% occur in hospitals or nursing facilities.
Many deaths occur in hospitals due to acute medical conditions, lack of access to home-based palliative care, or family preferences for medical supervision during end-of-life care.
Dying at home is often preferred for its comfort and familiarity, but the "best" place depends on individual needs, available support, and medical requirements.