Over the past five years, the question of whether hospital mortality rates have increased has garnered significant attention from healthcare professionals, policymakers, and researchers. Factors such as the global COVID-19 pandemic, aging populations, and advancements in medical technology have introduced complexities into mortality trends. While some studies suggest a rise in hospital mortality rates due to overwhelmed healthcare systems and delayed treatments during the pandemic, others argue that improved medical interventions and protocols may have mitigated these increases. Disparities in data collection and reporting across regions further complicate the analysis, making it essential to examine both short-term fluctuations and long-term patterns to draw accurate conclusions. Understanding these trends is crucial for identifying systemic challenges and implementing targeted interventions to improve patient outcomes.
Explore related products






What You'll Learn
![]()
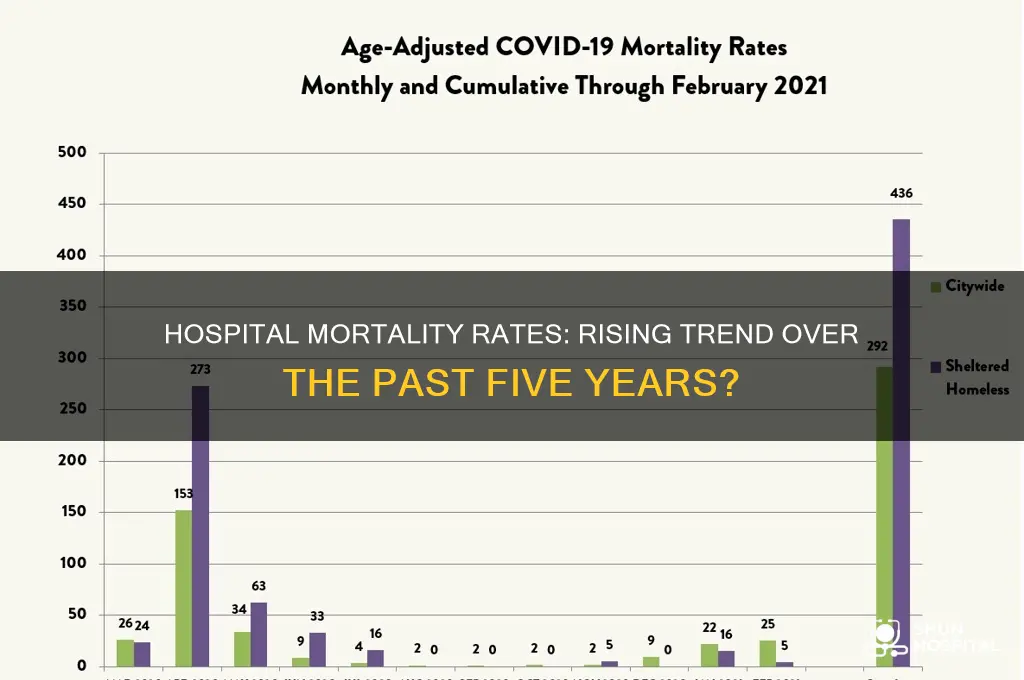
Impact of COVID-19 on hospital mortality rates
The COVID-19 pandemic has had a profound impact on hospital mortality rates globally, significantly contributing to the observed increase in the past five years. Prior to the pandemic, hospital mortality rates in many countries were either stable or showing a gradual decline due to advancements in medical technology, improved healthcare protocols, and better patient management. However, the emergence of COVID-19 in late 2019 disrupted this trend, overwhelming healthcare systems and leading to a sharp rise in mortality rates, particularly in hospitals. The virus not only directly caused fatalities but also indirectly increased mortality by straining resources, delaying treatments for non-COVID conditions, and increasing the risk of hospital-acquired infections.
One of the most direct impacts of COVID-19 on hospital mortality rates was the influx of severely ill patients requiring intensive care. Hospitals in hard-hit regions often operated beyond capacity, leading to shortages of critical resources such as ventilators, ICU beds, and healthcare personnel. This strain on healthcare infrastructure resulted in higher mortality rates among COVID-19 patients, particularly during peak waves of the pandemic. Studies have shown that mortality rates in hospitals were significantly higher during these periods compared to pre-pandemic levels, with older adults and those with comorbidities being disproportionately affected. The overwhelming caseload also meant that hospitals had to triage care, often prioritizing younger or otherwise healthier patients, which further exacerbated mortality rates among vulnerable populations.
Indirectly, the pandemic also increased hospital mortality rates by disrupting routine healthcare services. Many hospitals postponed elective surgeries and non-urgent treatments to allocate resources to COVID-19 patients, leading to delayed diagnoses and treatments for conditions like cancer, cardiovascular diseases, and diabetes. This delay in care contributed to poorer outcomes and higher mortality rates for patients with these conditions. Additionally, the fear of contracting COVID-19 in healthcare settings led to a decrease in hospital visits for acute and chronic conditions, further worsening health outcomes and increasing mortality.
Another critical factor in the rise of hospital mortality rates during the pandemic was the increased risk of hospital-acquired infections, including secondary bacterial and fungal infections in COVID-19 patients. Prolonged hospital stays, invasive procedures, and the use of immunosuppressive medications made patients more susceptible to these infections, which often had high mortality rates. Furthermore, the rapid turnover of patients and the need for healthcare workers to manage high caseloads may have contributed to lapses in infection control practices, exacerbating the problem.
In conclusion, the COVID-19 pandemic has been a major driver of the increase in hospital mortality rates over the past five years. Its direct impact on COVID-19 patients, combined with the indirect effects on healthcare delivery and infection control, has led to a significant rise in fatalities within hospital settings. While mortality rates have begun to stabilize in some regions as vaccination rates increase and healthcare systems adapt, the long-term consequences of the pandemic on hospital outcomes remain a critical area of study. Understanding these impacts is essential for improving healthcare resilience and preparedness for future public health crises.
Emergency Room or Urgent Care: Which is Best?
You may want to see also
Explore related products


$28.99 $37.99




![]()
Trends in mortality rates for specific age groups
The analysis of hospital mortality rates over the past five years reveals distinct trends across specific age groups, influenced by factors such as healthcare advancements, public health policies, and demographic shifts. Among pediatric populations (ages 0–18), mortality rates have generally declined, driven by improvements in neonatal care, vaccination programs, and the management of childhood diseases. However, disparities persist, particularly in low-income regions where access to specialized care remains limited. In contrast, young and middle-aged adults (ages 19–64) have shown a slight increase in hospital mortality rates, primarily attributed to the rise in chronic conditions like obesity, diabetes, and cardiovascular diseases, exacerbated by lifestyle factors and delayed healthcare-seeking behaviors during the COVID-19 pandemic.
For older adults (ages 65–84), hospital mortality rates have exhibited a mixed trend. While advancements in geriatric care and chronic disease management have led to reductions in mortality for certain conditions, the aging population and higher prevalence of comorbidities have offset some of these gains. Additionally, the impact of the COVID-19 pandemic disproportionately affected this age group, leading to temporary spikes in mortality rates. Among the oldest adults (ages 85 and above), mortality rates remain the highest across all age groups, with a gradual upward trend due to age-related frailty, multimorbidity, and increased susceptibility to infections. Despite this, palliative care improvements have focused on enhancing quality of life, which may influence end-of-life hospitalization patterns.
Regional variations also play a significant role in these trends. In high-income countries, mortality rates for most age groups have stabilized or decreased due to robust healthcare infrastructure and preventive measures. Conversely, low- and middle-income countries often report higher mortality rates, particularly among younger age groups, due to inadequate access to essential healthcare services. For instance, maternal and infant mortality rates in these regions remain elevated, contributing to overall hospital mortality figures.
Another critical factor is the differential impact of infectious diseases across age groups. While younger populations have benefited from reduced mortality due to vaccine-preventable diseases, older adults continue to face higher risks from infections like influenza and pneumonia. The COVID-19 pandemic further highlighted age-specific vulnerabilities, with mortality rates sharply increasing among older adults while remaining relatively low in younger populations.
In summary, trends in hospital mortality rates over the past five years vary significantly by age group, shaped by a combination of medical advancements, public health challenges, and socioeconomic determinants. While pediatric and some adult populations have seen declines, older adults continue to face elevated risks, underscoring the need for targeted interventions to address age-specific health needs and reduce disparities.
Las Vegas Nurses: Hospital Treatment and Care
You may want to see also
Explore related products






![]()
Influence of healthcare policy changes on mortality
Healthcare policy changes have played a significant role in shaping hospital mortality rates over the past five years. One of the most influential factors has been the implementation of value-based care models, which prioritize patient outcomes over the volume of services provided. Policies such as the Hospital Readmissions Reduction Program (HRRP) in the United States have incentivized hospitals to reduce avoidable readmissions by penalizing those with higher-than-expected rates. While this has led to improvements in care coordination and discharge planning, its direct impact on overall mortality rates remains debated. Some studies suggest that reduced readmissions correlate with lower mortality, as patients receive more consistent and effective care, while others argue that penalties may lead to unintended consequences, such as delayed readmissions or increased mortality among vulnerable populations.
Another critical policy change influencing mortality rates is the expansion of health insurance coverage under initiatives like the Affordable Care Act (ACA) in the U.S. or similar programs globally. Increased access to healthcare has enabled earlier disease detection and management, potentially reducing hospital mortality. For instance, insured individuals are more likely to seek preventive care, manage chronic conditions, and receive timely interventions, all of which contribute to lower mortality rates. However, disparities in access to care persist, particularly in regions with uneven policy implementation or inadequate healthcare infrastructure, limiting the full potential of these policies to reduce mortality.
The COVID-19 pandemic has also highlighted the profound impact of healthcare policy decisions on hospital mortality. Policies such as resource allocation, staffing mandates, and infection control protocols were critical in managing patient outcomes during the crisis. For example, hospitals in regions with robust public health policies, including early lockdowns and adequate personal protective equipment (PPE) distribution, generally reported lower mortality rates compared to those in areas with delayed or inconsistent responses. Additionally, the rapid authorization of vaccines and treatments under emergency policies significantly reduced mortality among hospitalized COVID-19 patients, demonstrating the life-saving potential of swift and evidence-based policy actions.
Furthermore, policies addressing healthcare workforce shortages and burnout have indirect but significant effects on mortality rates. Initiatives to improve staffing ratios, enhance worker protections, and invest in mental health support for healthcare professionals can lead to better patient care and outcomes. Overworked and understaffed hospitals often experience higher error rates and reduced quality of care, contributing to increased mortality. By prioritizing workforce well-being, policymakers can create an environment where healthcare delivery is safer and more effective, ultimately lowering hospital mortality rates.
Lastly, the integration of technology and data-driven policies has emerged as a key driver in reducing mortality. Electronic health records (EHRs), telemedicine, and predictive analytics enable more personalized and efficient care, reducing the likelihood of adverse outcomes. Policies promoting interoperability and data sharing among healthcare providers facilitate better coordination and decision-making, which can directly impact mortality rates. However, the success of these policies depends on equitable access to technology and digital literacy, ensuring that advancements benefit all patient populations rather than exacerbating existing disparities.
In conclusion, healthcare policy changes have a multifaceted influence on hospital mortality rates, with outcomes dependent on the design, implementation, and context of these policies. While initiatives like value-based care, insurance expansion, pandemic response measures, workforce support, and technological integration hold promise, their effectiveness must be continually evaluated to address unintended consequences and ensure equitable improvements in patient outcomes.
Effective Ways to Contact a Hospital Room
You may want to see also
Explore related products

$14.04 $24.95


$15.38 $26.99



![]()
Role of medical technology advancements in survival rates
The role of medical technology advancements in influencing survival rates cannot be overstated, particularly when examining trends in hospital mortality over the past five years. Innovations in diagnostic tools, treatment modalities, and patient monitoring systems have significantly contributed to improved patient outcomes. For instance, the advent of advanced imaging technologies, such as high-resolution MRI and CT scans, has enabled earlier and more accurate detection of diseases, allowing for timely interventions. This early detection is critical in conditions like cancer, cardiovascular diseases, and neurological disorders, where prompt treatment can drastically reduce mortality rates. Studies indicate that hospitals adopting cutting-edge diagnostic technologies have reported lower mortality rates compared to those relying on older methods, underscoring the direct impact of technological advancements on survival.
Another pivotal area where medical technology has enhanced survival rates is in the field of minimally invasive surgical techniques. Procedures such as robotic-assisted surgeries, laparoscopy, and endovascular interventions have revolutionized patient care by reducing recovery times, minimizing complications, and improving overall survival. These techniques allow for greater precision, lower infection risks, and less trauma to the patient, which are particularly beneficial for elderly or critically ill patients. Hospitals that have integrated these technologies into their surgical practices have observed a decline in postoperative mortality rates, highlighting the transformative role of innovation in surgical care.
The integration of artificial intelligence (AI) and machine learning in healthcare has also played a significant role in improving survival rates. AI-powered algorithms can analyze vast amounts of patient data to predict disease progression, identify high-risk patients, and recommend personalized treatment plans. For example, AI models have been employed to predict sepsis, a leading cause of hospital mortality, enabling early intervention and reducing fatality rates. Additionally, AI-driven decision support systems assist clinicians in making informed choices, reducing errors, and optimizing treatment strategies, which collectively contribute to lower mortality rates.
Furthermore, advancements in telemedicine and remote patient monitoring have expanded access to care, particularly in underserved or rural areas, thereby indirectly improving survival rates. Wearable devices and remote monitoring tools allow healthcare providers to track patients' vital signs in real time, detect early warning signs of deterioration, and intervene before conditions worsen. This is especially critical for chronic disease management and post-discharge care, where continuous monitoring can prevent readmissions and reduce mortality. The COVID-19 pandemic accelerated the adoption of telemedicine, and its long-term benefits on survival rates are becoming increasingly evident.
In conclusion, medical technology advancements have been a driving force behind the improvement in survival rates and the reduction in hospital mortality over the past five years. From enhanced diagnostics and minimally invasive surgeries to AI-driven analytics and telemedicine, these innovations have transformed patient care, making it more precise, accessible, and effective. As technology continues to evolve, its role in further decreasing mortality rates and enhancing healthcare outcomes will only grow, emphasizing the need for continued investment in medical innovation.
Understanding Hospital Blood Pressure Readings
You may want to see also
Explore related products

$31.37 $34.97





![]()
Comparison of mortality rates across different hospital types
The comparison of mortality rates across different hospital types is a critical aspect of understanding whether hospital mortality rates have increased over the past five years. Research indicates that mortality rates can vary significantly depending on the type of hospital, influenced by factors such as patient complexity, resource availability, and specialization. For instance, tertiary care hospitals, which often handle more severe and complex cases, tend to report higher mortality rates compared to primary or secondary care facilities. This disparity is not necessarily indicative of poorer care but rather reflects the higher acuity of patients treated in these settings. Over the past five years, studies have shown that while overall mortality rates may have stabilized or slightly increased, the gap between tertiary and primary care hospitals has widened, suggesting that patient complexity is a driving factor.
Specialized hospitals, such as those focused on cardiology, oncology, or pediatrics, also exhibit distinct mortality rate trends. These facilities often have lower mortality rates for conditions within their specialty due to concentrated expertise and advanced resources. However, when compared to general hospitals, their overall mortality rates may appear higher because they attract patients with more critical or rare conditions. A five-year analysis reveals that specialized hospitals have maintained relatively consistent mortality rates, benefiting from advancements in targeted treatments and protocols. In contrast, general hospitals, which treat a broader range of conditions, have seen slight increases in mortality rates, potentially due to resource constraints and a higher volume of diverse cases.
Rural and urban hospitals present another dimension in the comparison of mortality rates. Rural hospitals often face challenges such as limited staffing, fewer specialized services, and delayed access to critical care, which contribute to higher mortality rates. Urban hospitals, with greater access to resources and specialists, generally report lower mortality rates. Recent data suggests that the disparity between rural and urban hospital mortality rates has grown over the past five years, exacerbated by healthcare workforce shortages and funding disparities in rural areas. This trend underscores the need for targeted interventions to improve outcomes in rural settings.
Teaching hospitals, which combine patient care with medical education and research, often have mortality rates comparable to or lower than non-teaching hospitals, despite treating complex cases. This is attributed to the presence of experienced faculty, adherence to evidence-based practices, and access to cutting-edge treatments. However, smaller community hospitals, which may lack these advantages, have shown a slight upward trend in mortality rates over the past five years. This divergence highlights the impact of institutional resources and expertise on patient outcomes.
Finally, the comparison of mortality rates across hospital types must consider adjustments for case mix and patient severity. Hospitals treating older patients or those with multiple comorbidities will naturally report higher mortality rates. Standardized mortality ratios (SMRs), which account for these factors, provide a more accurate basis for comparison. Over the past five years, SMRs have shown that while some hospital types have improved their performance, others have struggled, particularly those with limited resources or serving high-risk populations. This nuanced comparison is essential for identifying areas needing improvement and informing policy decisions to address rising mortality rates.
How Hospitals and Pharma Companies Collaborate
You may want to see also
Frequently asked questions
Hospital mortality rates have varied over the past 5 years, with some regions or specific conditions showing increases while others remain stable or decrease. Factors like the COVID-19 pandemic, aging populations, and healthcare access disparities have influenced these trends.
Changes in hospital mortality rates are influenced by factors such as advancements in medical technology, healthcare policy changes, disease outbreaks (e.g., COVID-19), patient demographics, and the prevalence of chronic conditions.
Yes, the COVID-19 pandemic significantly impacted hospital mortality rates, leading to increases in many regions due to overwhelmed healthcare systems, limited resources, and the severity of the virus, especially among vulnerable populations.
Hospital mortality rates can be higher in rural areas due to limited access to specialized care, longer travel times to hospitals, and fewer healthcare resources, though this varies by region and specific healthcare systems.