In the heart of Los Angeles, two hospitals—one a prestigious, resource-rich academic medical center and the other a smaller, underfunded community hospital—are grappling with the coronavirus pandemic in starkly different ways. While the academic center leverages cutting-edge technology, ample staffing, and robust supply chains to manage the surge of patients, the community hospital struggles with limited resources, overworked staff, and a patient population disproportionately affected by socioeconomic disparities. These contrasting realities highlight the deep inequities in healthcare access and outcomes, revealing how the same crisis can manifest so differently across institutions just miles apart.
| Characteristics | Values |
|---|---|
| Hospital Names | Cedars-Sinai Medical Center (Private, Wealthy Area) & Martin Luther King Jr. Community Hospital (Public, Underserved Area) |
| Location | Both in Los Angeles, CA, but serving different socioeconomic populations. |
| Patient Demographics | Cedars-Sinai: Wealthier, insured patients; MLK: Low-income, uninsured/Medicaid patients. |
| Funding Sources | Cedars-Sinai: Private donations, insurance payments; MLK: Public funding, grants. |
| COVID-19 Case Load | Cedars-Sinai: Higher volume of severe cases due to specialized care; MLK: Higher volume of community cases. |
| Staffing Resources | Cedars-Sinai: More specialized staff, better staffing ratios; MLK: Staff shortages, higher nurse-to-patient ratios. |
| PPE Availability | Cedars-Sinai: Adequate supply; MLK: Limited supply, reliance on donations. |
| Testing Capacity | Cedars-Sinai: In-house testing, faster results; MLK: Dependent on external labs, slower results. |
| ICU Capacity | Cedars-Sinai: Larger ICU, more ventilators; MLK: Limited ICU beds, fewer ventilators. |
| Community Outreach | MLK: Active community outreach, mobile testing; Cedars-Sinai: Focused on patient care within hospital. |
| Mortality Rates | MLK: Higher mortality rates due to late presentations and comorbidities; Cedars-Sinai: Lower mortality rates. |
| Telehealth Adoption | Cedars-Sinai: Extensive telehealth services; MLK: Limited telehealth due to lack of patient access to technology. |
| Vaccine Distribution | Cedars-Sinai: Faster vaccine rollout; MLK: Slower rollout due to hesitancy and access issues. |
| Long-term Impact | MLK: Long-term strain on resources, increased health disparities; Cedars-Sinai: Better recovery, more resources for post-COVID care. |
Explore related products






What You'll Learn
- Staffing Challenges: One hospital struggles with shortages, while the other has surplus staff
- Resource Allocation: Disparities in PPE, ventilators, and testing kits between the two
- Patient Demographics: Serving affluent vs. underserved communities impacts COVID-19 response
- Financial Strain: One hospital thrives financially, the other faces bankruptcy risks
- Community Trust: Differing levels of public confidence affect patient influx and compliance
![]()
Staffing Challenges: One hospital struggles with shortages, while the other has surplus staff
In the heart of Los Angeles, two hospitals just miles apart are experiencing starkly different realities in their battle against the coronavirus pandemic, particularly when it comes to staffing. One, a public hospital serving a predominantly low-income population, is grappling with severe staff shortages that threaten its ability to provide adequate care. The other, a private, well-funded institution, finds itself with a surplus of staff, allowing it to not only manage the influx of COVID-19 patients but also to support other hospitals in need. The contrast highlights the broader disparities in healthcare resources and the unique challenges each facility faces.
The public hospital, already operating on a tight budget before the pandemic, has been hit hard by staffing shortages. Many of its nurses and doctors have fallen ill with COVID-19, forcing them to quarantine and leaving the hospital understaffed. Additionally, the hospital has struggled to attract temporary workers due to its lower pay rates compared to private institutions. As a result, remaining staff are overworked, often pulling double shifts to cover the gaps. This has led to burnout and fatigue, further exacerbating the staffing crisis. The hospital’s leadership has appealed to state and local authorities for assistance, but the competition for healthcare workers across the region has made it difficult to secure additional support.
In contrast, the private hospital has managed to maintain, and even expand, its workforce during the pandemic. With a larger budget, it has been able to offer competitive salaries and incentives to attract and retain staff. The hospital also implemented proactive measures early in the pandemic, such as hiring additional nurses and physicians in anticipation of a surge in patients. This foresight has paid off, as the hospital now has the flexibility to redeploy staff where needed and even lend personnel to overwhelmed facilities. Furthermore, its surplus staff has allowed it to establish specialized COVID-19 units and provide comprehensive care without compromising other services.
The staffing disparities between these two hospitals have significant implications for patient care. At the public hospital, the shortage of staff has led to longer wait times, delayed procedures, and reduced capacity to treat non-COVID patients. Overworked healthcare workers are also at higher risk of making errors, which can further compromise patient safety. Meanwhile, the private hospital’s surplus staff has enabled it to maintain high standards of care, ensuring that patients receive timely and effective treatment. This difference underscores the inequities in the healthcare system and the need for systemic solutions to address resource allocation.
Addressing these staffing challenges requires a multifaceted approach. For the public hospital, immediate financial support from government agencies and philanthropic organizations could help increase wages and attract temporary workers. Additionally, partnerships with nursing schools and training programs could provide a pipeline of new staff. The private hospital, on the other hand, could play a role in alleviating the burden on its public counterpart by sharing resources, such as staff and equipment, through formal agreements or collaborative initiatives. Such efforts would not only benefit individual hospitals but also strengthen the overall healthcare response to the pandemic in Los Angeles.
Ultimately, the contrasting staffing situations of these two hospitals serve as a microcosm of the broader challenges facing the healthcare system during the coronavirus pandemic. While the private hospital’s surplus staff positions it to weather the crisis more effectively, the public hospital’s shortages highlight the urgent need for investment in underfunded facilities. By learning from these disparities and implementing targeted solutions, Los Angeles can work toward a more equitable and resilient healthcare system for all its residents.
A Hospital Room: A Sanctuary of Healing and Care
You may want to see also
Explore related products






![]()
Resource Allocation: Disparities in PPE, ventilators, and testing kits between the two
In the heart of Los Angeles, two hospitals—one a well-funded, private institution in an affluent neighborhood and the other a public, safety-net hospital in a low-income area—highlight stark disparities in resource allocation during the coronavirus pandemic. Personal Protective Equipment (PPE) emerged as a critical point of divergence. The private hospital, backed by robust financial resources and established supply chains, maintained a steady stockpile of high-quality PPE, including N95 masks, gowns, and face shields. In contrast, the public hospital faced chronic shortages, often relying on donations or makeshift solutions like reusing single-use PPE. This disparity not only endangered frontline workers at the public hospital but also exacerbated the risk of infection spread within the facility and the surrounding community.
Ventilators, another lifeline in the fight against COVID-19, further underscored the resource gap. The private hospital boasted a surplus of state-of-the-art ventilators, ensuring that every critically ill patient received timely and adequate care. Meanwhile, the public hospital struggled with an outdated fleet of ventilators, many of which were in disrepair or insufficient in number. This shortage forced the public hospital to make agonizing triage decisions, prioritizing patients based on their likelihood of survival. The disparity in ventilator access mirrored broader systemic inequalities, as the public hospital served a predominantly uninsured or underinsured population with higher rates of pre-existing conditions.
Testing kits, essential for early detection and containment of the virus, also revealed a chasm between the two hospitals. The private hospital implemented rapid, on-site testing capabilities, allowing for quick diagnosis and isolation of infected individuals. In contrast, the public hospital faced delays due to reliance on off-site labs and limited test kit availability. These delays hindered contact tracing efforts and prolonged the time patients spent in crowded emergency rooms, increasing the risk of transmission. The private hospital’s ability to secure testing kits through private vendors and partnerships highlighted the advantages of financial flexibility, while the public hospital’s dependence on government allocations left it vulnerable to supply chain disruptions.
The root of these disparities lies in systemic funding inequalities. The private hospital benefited from a combination of private insurance reimbursements, philanthropic donations, and endowments, enabling it to invest in infrastructure and stockpiles proactively. Conversely, the public hospital operated on a shoestring budget, with funding often tied to political priorities and insufficient to meet the demands of a public health crisis. This financial gap was further exacerbated by the pandemic, as the public hospital absorbed a disproportionate share of uninsured COVID-19 patients, straining its already limited resources.
Addressing these disparities requires targeted policy interventions. Equitable distribution of federal and state resources, prioritization of safety-net hospitals in supply chains, and increased funding for public healthcare infrastructure are essential steps. Additionally, public-private partnerships could bridge the gap by leveraging the private sector’s resources to support underfunded institutions. Without such measures, the pandemic will continue to expose and deepen the fault lines in Los Angeles’ healthcare system, leaving the most vulnerable populations at greater risk.
The Hospital Habits of Chinese People
You may want to see also
Explore related products






![]()
Patient Demographics: Serving affluent vs. underserved communities impacts COVID-19 response
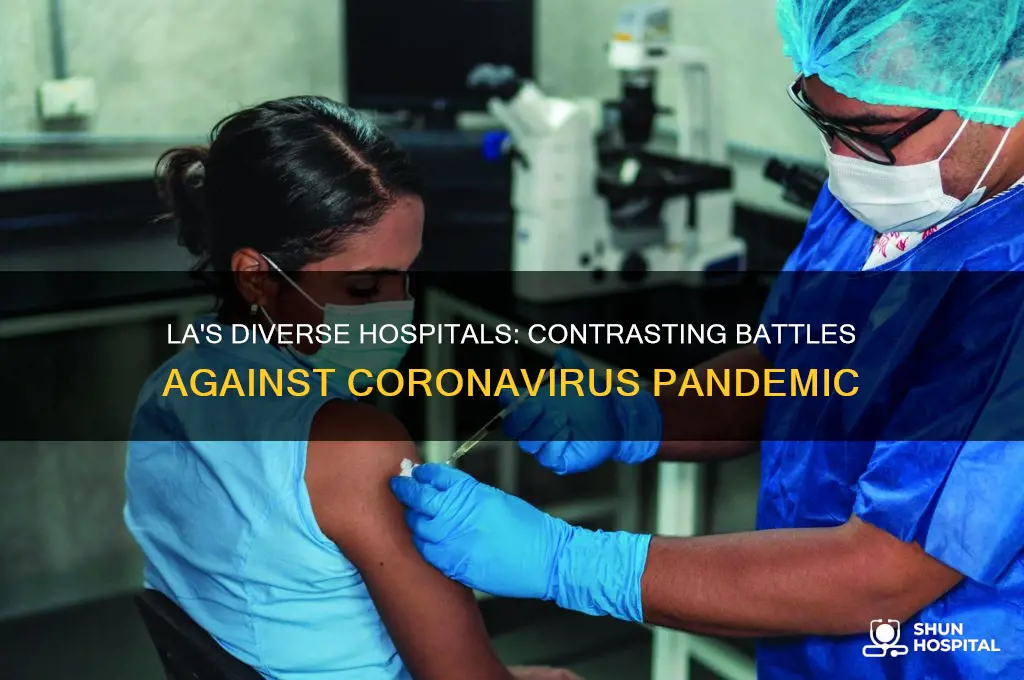
In Los Angeles, the stark contrast between affluent and underserved communities has significantly influenced how hospitals respond to the COVID-19 pandemic. Hospitals serving wealthy areas, such as Cedars-Sinai Medical Center, often cater to patients with private insurance, higher health literacy, and greater access to resources. These patients are more likely to seek early testing and treatment, which can lead to better outcomes. Affluent communities also tend to have higher vaccination rates due to better access to information and healthcare facilities. As a result, hospitals in these areas have focused on providing advanced treatments, telemedicine options, and streamlined care for COVID-19 patients, leveraging their robust financial and technological resources.
Conversely, hospitals serving underserved communities, like Martin Luther King Jr. Community Hospital (MLKCH) in South Los Angeles, face unique challenges. Patients in these areas often lack health insurance, have limited access to transportation, and live in crowded housing conditions, which exacerbate the spread of the virus. Additionally, many residents in underserved communities are essential workers, increasing their exposure risk. Hospitals like MLKCH have had to prioritize community outreach, mobile testing units, and multilingual education campaigns to address these disparities. Their response has been more resource-intensive, requiring creative solutions to overcome systemic barriers to care.
The patient demographics in these hospitals also dictate the types of interventions needed. Affluent hospitals can focus on specialized care, such as monoclonal antibody treatments and intensive care for severe cases, knowing their patients are more likely to arrive early in the disease course. In contrast, underserved hospitals often deal with patients presenting later in their illness, requiring more urgent and intensive interventions. This delay in care is partly due to economic constraints, fear of medical bills, and a historical distrust of the healthcare system among marginalized populations.
Another critical difference lies in the long-term impact of COVID-19 on these communities. Hospitals in affluent areas have shifted their focus to post-COVID care, including rehabilitation for "long-haul" symptoms, which their patients can afford. Meanwhile, underserved hospitals continue to grapple with acute cases and the ongoing challenge of managing chronic conditions exacerbated by the pandemic, such as diabetes and hypertension. The disparity in resources means that while one hospital may be planning for recovery, the other is still fighting to control the spread.
Ultimately, the COVID-19 response in Los Angeles hospitals reflects broader societal inequalities. Hospitals serving affluent communities benefit from pre-existing advantages, allowing them to innovate and adapt quickly. In contrast, those serving underserved communities must address systemic issues like poverty, lack of access, and health disparities, which complicate every aspect of their response. Recognizing these differences is crucial for policymakers and healthcare leaders to allocate resources equitably and ensure that all communities, regardless of socioeconomic status, receive the care they need during a public health crisis.
Code Black: Hospital Emergency Protocol Explained
You may want to see also
Explore related products






![]()
Financial Strain: One hospital thrives financially, the other faces bankruptcy risks
In the heart of Los Angeles, two hospitals, just miles apart, are experiencing starkly different financial realities as they navigate the challenges of the coronavirus pandemic. Cedars-Sinai Medical Center, a prestigious nonprofit hospital, has not only maintained its financial stability but has also seen a significant increase in revenue. This can be attributed to its robust pre-pandemic financial reserves, high-acuity patient services, and a well-established network of private insurance patients. Cedars-Sinai's ability to quickly adapt to the surge in COVID-19 cases, coupled with its reputation for excellence, has allowed it to attract a steady stream of patients, ensuring a consistent cash flow. The hospital's financial thriving is further supported by its ability to negotiate favorable reimbursement rates with insurance companies and its success in securing government grants and donations.
In stark contrast, Martin Luther King Jr. Community Hospital (MLKCH), a safety-net hospital serving a predominantly low-income population, is facing an unprecedented financial crisis. The hospital, which relies heavily on Medicaid reimbursements, has been hit hard by the pandemic. Medicaid reimbursements, notoriously lower than private insurance payments, have left MLKCH struggling to cover its operational costs. The surge in uninsured COVID-19 patients has exacerbated this issue, as the hospital is forced to provide care without the guarantee of reimbursement. Furthermore, MLKCH's limited financial reserves have made it difficult to invest in the necessary infrastructure and equipment to handle the influx of patients, creating a vicious cycle of financial strain.
The financial disparities between these two hospitals can also be attributed to their patient demographics. Cedars-Sinai's patient population is largely comprised of individuals with private insurance, who are more likely to seek elective procedures and specialized care, services that are typically more lucrative for hospitals. In contrast, MLKCH serves a population with a higher proportion of uninsured and underinsured individuals, who are more likely to rely on emergency services and less profitable treatments. This difference in patient mix has significant implications for the hospitals' revenue streams, with Cedars-Sinai benefiting from higher-margin services and MLKCH struggling to break even.
Another critical factor contributing to the financial strain on MLKCH is the hospital's higher operating costs relative to its revenue. The need to provide care for a large number of uninsured patients, coupled with the increased costs associated with COVID-19 treatment, has put a significant strain on the hospital's resources. In contrast, Cedars-Sinai's efficient cost management strategies, including streamlined supply chain processes and optimized staffing models, have enabled it to maintain a healthy operating margin. The ability to quickly pivot to telemedicine and other cost-saving measures has further bolstered Cedars-Sinai's financial position, while MLKCH has struggled to implement similar initiatives due to limited resources and technological infrastructure.
As the pandemic continues to evolve, the financial divergence between these two hospitals is likely to widen. Cedars-Sinai's strong financial position will enable it to invest in cutting-edge technology, expand its services, and attract top talent, further solidifying its reputation as a leading healthcare provider. Meanwhile, MLKCH's financial struggles may force it to make difficult decisions, such as cutting services, reducing staff, or even declaring bankruptcy. To mitigate this risk, policymakers and healthcare leaders must explore innovative solutions, such as increasing Medicaid reimbursements, providing targeted financial assistance, and implementing value-based care models that prioritize outcomes over volume. By addressing the underlying financial disparities between hospitals like Cedars-Sinai and MLKCH, we can work towards a more equitable and sustainable healthcare system that serves all Angelenos, regardless of their socioeconomic status.
Discovering Yale New Haven Hospital's Exact Location in Connecticut
You may want to see also
Explore related products






![]()
Community Trust: Differing levels of public confidence affect patient influx and compliance
In the heart of Los Angeles, two hospitals—one in a predominantly affluent area and the other in a historically underserved community—illustrate how differing levels of community trust profoundly impact patient influx and compliance during the coronavirus pandemic. The first hospital, located in a wealthy neighborhood, enjoys a long-standing reputation for high-quality care and state-of-the-art facilities. Residents in this area have historically trusted the healthcare system, viewing it as reliable and responsive to their needs. As a result, when the pandemic struck, this hospital saw a steady stream of patients seeking testing, treatment, and vaccinations. The community’s trust translated into high compliance rates with public health measures, such as mask mandates and vaccination drives, which helped mitigate the spread of the virus.
In contrast, the second hospital, situated in a low-income, minority-dominated neighborhood, faced significant challenges due to decades of systemic neglect and mistrust in the healthcare system. Historical injustices, such as the Tuskegee Syphilis Study and unequal treatment, have left a legacy of skepticism among residents. During the pandemic, this mistrust manifested in lower patient influx, as many community members hesitated to seek medical care or follow public health guidelines. The hospital struggled to convince residents of the safety and efficacy of vaccines, leading to lower vaccination rates compared to wealthier areas. This lack of trust not only hindered individual health outcomes but also exacerbated the community’s vulnerability to COVID-19 outbreaks.
To address these disparities, the second hospital implemented community-centered strategies to rebuild trust. They partnered with local leaders, churches, and grassroots organizations to disseminate accurate information about the virus and vaccines. By involving trusted figures in the community, the hospital aimed to bridge the gap between healthcare providers and residents. Additionally, they offered culturally sensitive care and ensured that staff reflected the diversity of the community, fostering a sense of familiarity and understanding. These efforts gradually increased patient influx and compliance, though progress remained slower compared to the more affluent hospital.
The differing levels of community trust also influenced how each hospital managed resources and patient care. The wealthier hospital, with its higher patient volume, could allocate resources efficiently, ensuring timely treatment and adequate staffing. Meanwhile, the underserved hospital faced resource constraints due to lower patient turnout and higher no-show rates for appointments. This disparity highlighted the need for targeted funding and support to strengthen healthcare infrastructure in marginalized communities. Without addressing the root causes of mistrust, such inequalities would persist, perpetuating health disparities during crises like the pandemic.
Ultimately, the experiences of these two Los Angeles hospitals underscore the critical role of community trust in shaping public health outcomes. Hospitals in areas with high trust levels benefit from proactive patient engagement and compliance, while those in distrustful communities must invest in relationship-building and tailored outreach. Policymakers and healthcare leaders must recognize that trust is not uniform and that addressing historical inequities is essential to ensuring equitable care. By prioritizing community trust, hospitals can improve patient influx, compliance, and overall resilience in the face of public health emergencies.
Loose Horse in Hospital: Has the Fugitive Equine Been Caught?
You may want to see also
Frequently asked questions
The two hospitals are Cedars-Sinai Medical Center, a large, well-funded private hospital, and Martin Luther King Jr. Community Hospital, a smaller, public facility serving a predominantly low-income and uninsured population.
Cedars-Sinai has leveraged its extensive resources to expand testing, increase ICU capacity, and implement advanced telemedicine services. It has also conducted research and clinical trials related to COVID-19 treatments.
MLK Jr. Community Hospital has struggled with limited resources, a high patient load, and serving a community with significant pre-existing health disparities. It has relied on partnerships and emergency funding to address these challenges.
While Cedars-Sinai has focused on cutting-edge treatments and research, MLK Jr. Community Hospital has prioritized community outreach, education, and addressing social determinants of health. Both have worked with local health departments to ensure equitable vaccine distribution.





![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)

![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)

![Pandemic [Blu-ray]](https://m.media-amazon.com/images/I/61EbhmkB1tS._AC_UL320_.jpg)
![Pandemic [DVD]](https://m.media-amazon.com/images/I/91ynbSGeZVS._AC_UL320_.jpg)
![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)