Hospitals worldwide have adapted their treatment protocols to address the challenges posed by COVID-19, focusing on a combination of supportive care, antiviral therapies, and innovative interventions. Early in the pandemic, treatment primarily involved managing symptoms such as fever, cough, and shortness of breath, with oxygen therapy and mechanical ventilation for severe cases. As research progressed, antiviral medications like remdesivir and monoclonal antibody treatments were introduced to reduce viral replication and improve outcomes. Additionally, corticosteroids such as dexamethasone became standard for patients with severe disease to mitigate inflammation. Hospitals have also emphasized preventive measures, including vaccination campaigns and infection control practices, while continuously monitoring emerging variants and adjusting treatments accordingly. The integration of telemedicine and remote monitoring has further enhanced patient care, ensuring timely interventions and reducing the strain on healthcare systems.
Explore related products


$42.58 $44.95




What You'll Learn
- Oxygen Therapy: Administering oxygen via nasal cannulas, masks, or ventilators to support breathing in severe cases
- Antiviral Medications: Using drugs like remdesivir to inhibit viral replication and reduce disease severity
- Corticosteroids: Prescribing dexamethasone to reduce inflammation and improve outcomes in hospitalized patients
- Monoclonal Antibodies: Delivering lab-made antibodies to block viral entry and prevent severe illness
- Supportive Care: Managing symptoms, fluids, nutrition, and preventing complications like blood clots or infections
![]()
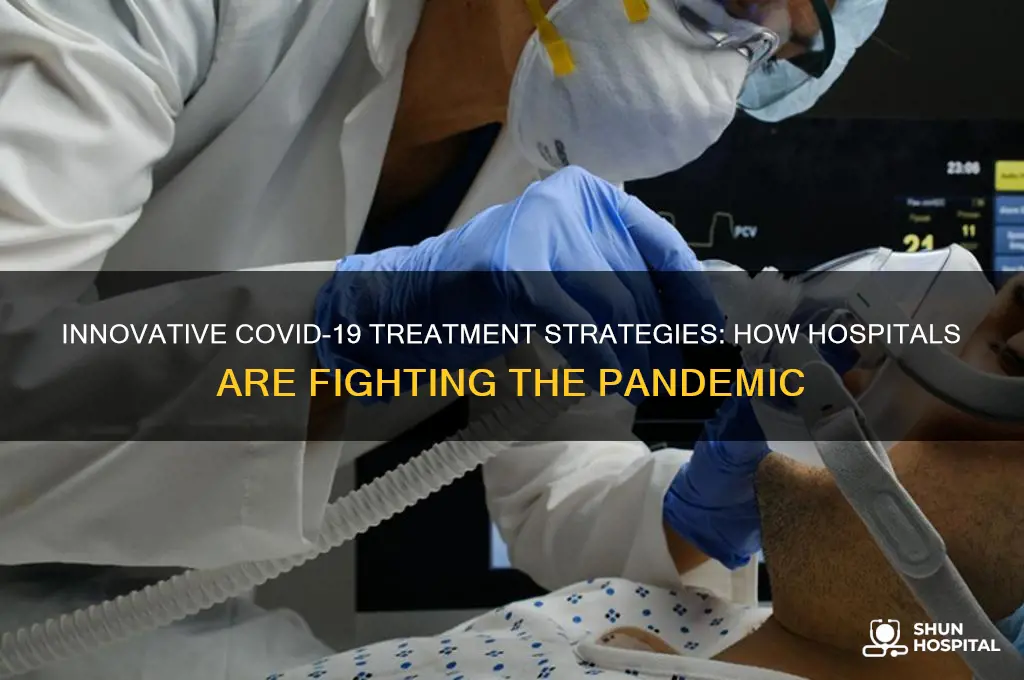
Oxygen Therapy: Administering oxygen via nasal cannulas, masks, or ventilators to support breathing in severe cases
Oxygen therapy stands as a cornerstone in the treatment of severe COVID-19 cases, where respiratory distress threatens to overwhelm the body’s ability to function. The primary goal is to maintain adequate oxygen saturation levels, typically aiming for SpO2 readings above 92% in adults, though targets may vary based on patient-specific factors such as pre-existing conditions or age. Administering oxygen via nasal cannulas, masks, or ventilators is a tiered approach, escalating based on disease severity. Nasal cannulas, delivering 1–6 liters of oxygen per minute, are often the first line of defense for patients with mild to moderate hypoxemia. For those requiring higher concentrations, non-rebreather masks can provide up to 15 liters per minute, ensuring a more substantial oxygen supply. Ventilators, the most invasive option, are reserved for critical cases where spontaneous breathing is insufficient, offering precise control over oxygen delivery and respiratory rate.
The choice of oxygen delivery method hinges on balancing efficacy with patient comfort and clinical condition. Nasal cannulas, for instance, are well-tolerated for extended periods but may not suffice for patients with severe acute respiratory distress syndrome (ARDS). In such cases, high-flow nasal cannulas (HFNC) or non-invasive ventilation (NIV) can bridge the gap before intubation becomes necessary. HFNC systems, delivering heated and humidified oxygen at flows up to 60 liters per minute, have shown promise in reducing intubation rates in some COVID-19 patients. However, caution is advised with NIV in COVID-19, as aerosolization of viral particles poses risks to healthcare workers if proper protective measures are not in place.
Practical considerations are critical in administering oxygen therapy. Monitoring for signs of deterioration, such as increasing respiratory rate or declining SpO2 levels, is essential to prevent delays in escalating care. Positioning patients in prone or semi-prone positions can improve oxygenation in severe cases, a technique known as awake prone positioning. For ventilated patients, lung-protective strategies, including low tidal volumes (4–8 mL/kg of predicted body weight) and limiting plateau pressures to under 30 cm H2O, are vital to minimize ventilator-induced lung injury. Pediatric and elderly patients require tailored approaches, with lower oxygen saturation targets for children (e.g., 90–94%) and careful monitoring for frail older adults, who may decompensate rapidly.
Despite its life-saving potential, oxygen therapy is not without risks. Prolonged use of high-flow oxygen can lead to hyperoxia, which may exacerbate lung injury in some patients. Over-reliance on non-invasive methods in critically ill patients can delay necessary intubation, worsening outcomes. Resource constraints, particularly in low-income settings, further complicate access to oxygen therapy, highlighting the need for innovative solutions like oxygen concentrators and decentralized oxygen generation systems. Ultimately, oxygen therapy in COVID-19 is a delicate balance of art and science, requiring vigilant monitoring, individualized care, and a readiness to adapt strategies as the patient’s condition evolves.
Hospital Pre-Registration: A Simple Guide for Patients
You may want to see also
Explore related products






![]()
Antiviral Medications: Using drugs like remdesivir to inhibit viral replication and reduce disease severity
Antiviral medications have emerged as a cornerstone in the fight against COVID-19, with drugs like remdesivir leading the charge. Remdesivir, a broad-spectrum antiviral originally developed for Ebola, works by inhibiting viral RNA polymerase, effectively disrupting the virus’s ability to replicate within the body. This mechanism not only slows the progression of the disease but also reduces the severity of symptoms, particularly in hospitalized patients with moderate to severe COVID-19. Administered intravenously, remdesivir is typically given in a 200 mg loading dose on the first day, followed by 100 mg once daily for up to 5 days, depending on the patient’s condition and response to treatment.
The efficacy of remdesivir lies in its ability to target the virus directly, unlike supportive therapies that focus on managing symptoms. Clinical trials have shown that it can shorten recovery time by several days, particularly in patients requiring oxygen support. However, it is most effective when administered early in the disease course, ideally within 7 days of symptom onset. This underscores the importance of prompt diagnosis and hospitalization for eligible patients. While remdesivir is not a cure, its role in reducing the burden on healthcare systems by decreasing hospitalization duration and the need for invasive ventilation cannot be overstated.
Despite its benefits, the use of remdesivir is not without limitations. It is not recommended for patients with severe kidney impairment or those under 12 years of age, as safety and efficacy in these populations remain uncertain. Additionally, its intravenous administration requires hospitalization, limiting its use to clinical settings. This has sparked discussions about the development of oral antiviral agents, such as molnupiravir and paxlovid, which offer similar benefits but can be taken at home. These alternatives are particularly valuable for high-risk individuals who may not have immediate access to hospital care.
In practice, the integration of remdesivir into COVID-19 treatment protocols requires careful consideration of patient profiles and disease progression. Healthcare providers must weigh factors like comorbidities, oxygen saturation levels, and symptom duration before initiating treatment. For instance, patients with pre-existing liver conditions should be monitored closely, as remdesivir can cause transient elevations in liver enzymes. Combining remdesivir with other therapies, such as dexamethasone for inflammation or monoclonal antibodies for high-risk outpatients, has also shown promise in optimizing outcomes.
Ultimately, antiviral medications like remdesivir represent a critical tool in the multifaceted approach to COVID-19 treatment. Their ability to directly target viral replication offers a unique advantage in reducing disease severity and improving recovery rates. As research continues, the development of more accessible and versatile antiviral options will further enhance our ability to combat this pandemic. For now, remdesivir remains a vital resource in hospitals worldwide, offering hope to patients and clinicians alike in the ongoing battle against COVID-19.
When Staph Infections Demand Hospital Care: Key Indicators and Risks
You may want to see also
Explore related products






![]()
Corticosteroids: Prescribing dexamethasone to reduce inflammation and improve outcomes in hospitalized patients
Hospitals worldwide have turned to corticosteroids, particularly dexamethasone, as a critical intervention for severe COVID-19 cases. This shift followed the RECOVERY trial, which demonstrated a significant reduction in mortality among hospitalized patients requiring oxygen support. Dexamethasone, a potent anti-inflammatory, mitigates the cytokine storm—an overactive immune response often fatal in COVID-19. Its efficacy is most pronounced in patients on mechanical ventilation, where it reduces mortality by up to one-third. This breakthrough has cemented dexamethasone’s role as a standard of care in critical cases, offering a lifeline to those at highest risk.
Prescribing dexamethasone requires precision. The recommended dosage is 6 mg once daily, administered orally or intravenously, for up to 10 days. This regimen is tailored to hospitalized patients requiring supplemental oxygen, including those on ventilators. For children and adolescents, dosing is weight-based, typically 0.15 mg/kg per day, capped at 6 mg. It’s crucial to avoid prolonged use beyond the 10-day window, as extended corticosteroid therapy can lead to complications like hyperglycemia, immunosuppression, or secondary infections. Clinicians must balance the drug’s benefits against these risks, particularly in patients with comorbidities like diabetes or hypertension.
While dexamethasone’s anti-inflammatory properties are transformative, its use is not without caution. It is contraindicated in patients with active untreated infections, as it can exacerbate these conditions. Additionally, it should not be used in mild or moderate COVID-19 cases not requiring oxygen, as studies show no benefit and potential harm in these populations. Monitoring for adverse effects, such as fluid retention or psychiatric disturbances, is essential. Practical tips include co-prescribing proton pump inhibitors to prevent gastrointestinal bleeding and closely tracking blood glucose levels, especially in diabetic patients.
Comparatively, dexamethasone stands out among corticosteroids for its cost-effectiveness and widespread availability, making it accessible even in resource-limited settings. Unlike other treatments like remdesivir or monoclonal antibodies, which target viral replication or specific immune pathways, dexamethasone addresses the broader inflammatory cascade, offering a more universal benefit. Its adoption has significantly influenced global COVID-19 treatment protocols, reducing mortality rates and easing the burden on intensive care units. As the pandemic evolves, dexamethasone remains a cornerstone of therapy, exemplifying how evidence-based medicine adapts to meet urgent clinical needs.
Best Fish Hospital in Orange City, Florida
You may want to see also
Explore related products


![Bed Pads with Adhesive Strip 30"x36" Thicken Elderly Adults Incontinence Underpads Disposable,Heavy Duty Absorbent Chucks Waterproof,XL Extra Large Puppy Pee Training Pad[25 Pads]](https://m.media-amazon.com/images/I/718d1g4T4NL._AC_UL320_.jpg)



![]()
Monoclonal Antibodies: Delivering lab-made antibodies to block viral entry and prevent severe illness
Monoclonal antibodies have emerged as a targeted therapy in the fight against COVID-19, offering a unique approach to neutralize the virus before it wreaks havoc on the body. Unlike vaccines, which train the immune system to recognize and combat the virus, monoclonal antibodies are lab-engineered proteins designed to mimic the body’s natural defenses. These antibodies bind directly to the spike protein of the SARS-CoV-2 virus, blocking its ability to enter human cells and replicate. This intervention is particularly crucial for high-risk individuals, such as the elderly, immunocompromised patients, or those with underlying health conditions, who are more susceptible to severe illness.
Administering monoclonal antibodies involves a precise protocol, typically delivered via intravenous infusion over 20 to 30 minutes. The treatment is most effective when given early in the course of the disease, ideally within 10 days of symptom onset. For example, the FDA-approved monoclonal antibody cocktail casirivimab and imdevimab (Regeneron) is administered at a dose of 1,200 mg of each antibody, while sotrovimab is given as a single 500 mg dose. These treatments are not intended for hospitalized patients already on oxygen therapy, as their effectiveness diminishes in later stages of the disease. Instead, they are reserved for outpatient settings to prevent progression to severe COVID-19, reducing the likelihood of hospitalization or death.
One of the challenges with monoclonal antibodies is their limited accessibility and the need for specialized healthcare settings for administration. Infusion centers or hospitals must be equipped to handle potential allergic reactions, though these are rare. Additionally, the treatment is not a substitute for vaccination, as it provides only temporary protection. However, for those who are unvaccinated or at high risk, monoclonal antibodies offer a critical lifeline. Practical tips for patients include scheduling the infusion as soon as possible after testing positive and ensuring transportation arrangements, as the treatment can cause mild side effects like fatigue or nausea.
Comparatively, monoclonal antibodies stand out as a proactive measure in COVID-19 treatment, distinct from reactive therapies like antiviral medications or corticosteroids. While antivirals such as Paxlovid target viral replication within the body, monoclonal antibodies act as a preemptive strike, neutralizing the virus before it gains a foothold. This distinction makes them a valuable tool in the early stages of infection, particularly as new variants emerge with increased transmissibility. However, their efficacy can wane against certain mutations, necessitating ongoing research to develop updated formulations.
In conclusion, monoclonal antibodies represent a groundbreaking advancement in COVID-19 treatment, offering a targeted and effective solution for high-risk individuals. Their ability to block viral entry and prevent severe illness underscores their importance in the pandemic response toolkit. While logistical challenges and variant-specific limitations exist, their role in reducing hospitalizations and saving lives cannot be overstated. For those eligible, early access to this treatment can make a significant difference in the course of the disease, highlighting the importance of awareness and timely intervention.
Setting Up Stress Echo: A Comprehensive Hospital Implementation Guide
You may want to see also
Explore related products


![Vakly Male Urinal with Glow in The Dark Cover [32oz Pack of 2] Portable Pee Bottles for Men Used for Hospitals, Incontinence, Emergency and Travel (2)](https://m.media-amazon.com/images/I/71zEIGo5CFL._AC_UL320_.jpg)



![]()
Supportive Care: Managing symptoms, fluids, nutrition, and preventing complications like blood clots or infections
Hospitals have shifted their focus to supportive care as a cornerstone of COVID-19 treatment, recognizing that managing symptoms and preventing complications can significantly improve patient outcomes. This approach is particularly crucial for patients with moderate to severe illness, where the body’s response to the virus can be as damaging as the infection itself. Supportive care is tailored to address the multifaceted needs of these patients, encompassing symptom management, fluid and nutritional support, and proactive measures to prevent secondary issues like blood clots or infections.
Symptom management begins with alleviating the most common and distressing manifestations of COVID-19, such as fever, cough, and shortness of breath. For fever, acetaminophen is typically recommended, with dosages adjusted based on age and weight (e.g., 10–15 mg/kg every 4–6 hours for children, up to 1000 mg every 6 hours for adults). Cough suppressants like dextromethorphan or expectorants like guaifenesin may be used, though their efficacy is often limited. Oxygen therapy is critical for patients with hypoxia, starting with nasal cannulas (1–5 L/min) and escalating to high-flow systems or ventilatory support as needed. Pain management, particularly in severe cases, may involve opioids, but caution is exercised to avoid respiratory depression.
Fluid and nutritional support are equally vital, as COVID-19 can lead to dehydration, electrolyte imbalances, and malnutrition, especially in critically ill patients. Intravenous fluids are administered to maintain hydration, with rates tailored to the patient’s condition (e.g., 1–2 mL/kg/hr for maintenance, adjusted for deficits or ongoing losses). Nutritional needs are addressed through enteral feeding whenever possible, with protein-rich formulas (1.2–1.5 g/kg/day) to support immune function and wound healing. For patients unable to tolerate oral intake, parenteral nutrition may be initiated within 7–10 days of hospitalization. Monitoring for refeeding syndrome is essential, particularly in malnourished patients, with close observation of electrolytes like phosphorus and potassium.
Preventing complications is a proactive aspect of supportive care, with blood clots and secondary infections posing significant risks. Anticoagulation therapy, such as low-molecular-weight heparin (e.g., enoxaparin 40 mg daily for prophylaxis, or higher doses for treatment), is widely used to mitigate the risk of thromboembolic events, which are elevated in COVID-19 patients due to inflammation and immobilization. Infection prevention includes strict adherence to hand hygiene, personal protective equipment, and early identification of bacterial or fungal superinfections. Empiric antibiotics are reserved for patients with clear signs of secondary infection, as overuse can lead to antibiotic resistance and disrupt the gut microbiome.
In practice, supportive care requires a multidisciplinary approach, involving physicians, nurses, dietitians, and physical therapists. Early mobilization, even in ventilated patients, is encouraged to prevent muscle atrophy and reduce the risk of clots. Practical tips for caregivers include monitoring urine output to assess hydration status, using incentive spirometry to prevent lung complications, and providing emotional support to patients who may feel isolated due to infection control measures. By addressing these elements comprehensively, hospitals can optimize recovery and minimize long-term complications in COVID-19 patients.
Trump Hospitalized: What We Know So Far
You may want to see also
Frequently asked questions
Hospitals primarily focus on supportive care, including oxygen therapy for breathing difficulties, intravenous fluids, and medications like dexamethasone (a corticosteroid) to reduce inflammation. For severe cases, mechanical ventilation and monoclonal antibody treatments may be used.
Yes, remdesivir, an antiviral medication, is still used in hospitals for hospitalized patients with mild to moderate COVID-19, particularly those at high risk of severe disease. Its use is based on guidelines from health organizations like the WHO and CDC.
Hospitals tailor treatment plans for patients with comorbidities like diabetes, heart disease, or obesity. This includes closely monitoring symptoms, adjusting medications to avoid interactions, and providing specialized care to address both COVID-19 and underlying conditions.
Yes, monoclonal antibodies are used for high-risk, non-hospitalized patients with mild to moderate COVID-19 to prevent severe illness. However, their effectiveness varies with emerging variants, and hospitals follow updated guidelines for their use.



![Chucks MAX Hospital Bed Pads Disposable Adult 36 x 36 Breathable Incontinence Pads - XXX-Large Pee Pads for Adults - Heavy Duty Absorbency Underpads - 400 Lbs. Patient Repositioning [20 Count]](https://m.media-amazon.com/images/I/81q9DQQ6TAL._AC_UL320_.jpg)