Death is a common occurrence in hospitals, with over 700,000 patients dying in US hospitals in 2010. While the inpatient hospital death rate has decreased from 2.5 per 100 inpatients in 2000 to 2.0 per 100 inpatients in 2010, the number of deaths in hospitals remains high. The most common causes of death in hospitals are sepsis, medical malpractice, misdiagnosis, and other medical errors. Studies have shown that more than 250,000 people die from medical errors every year in the US, with the true number possibly being as high as 440,000 due to underreporting and a lack of clarity on death certificates. Additionally, a large proportion of hospital deaths occur after long admissions that begin with treatable problems, and aggressive life-prolonging interventions may be carried out even when a patient's death is expected.
| Characteristics | Values |
|---|---|
| Common causes of death in hospitals | Sepsis, medical malpractice, misdiagnosis, and other medical errors |
| Number of deaths in hospitals in the US, 2000 | 2.5 out of every 100 inpatients |
| Number of deaths in hospitals in the US, 2010 | 2 out of every 100 inpatients |
| Number of patients who died in US hospitals in 2010 | Over 700,000 |
| Percentage of deaths in US hospitals in 2000 | 48.0% |
| Percentage of deaths in US hospitals in 2018 | 35.1% |
| Percentage of expected deaths in Italian hospitals | 58% |
| Percentage of patients who experienced at least one "severe" symptom | 75% |
| Percentage of nurses who judged patients' global care as "good" or "very good" | 76% |
| Number of inpatients in 25 Scottish hospitals on March 31, 2010 | 10,743 |
| Number of patients in Scottish hospitals who died within 12 months | 3098 (28.8%) |
Explore related products






What You'll Learn
![]()
Misdiagnosis and medical errors
Medication errors are a frequent occurrence in hospitals, and while not all result in harm, those that do can be extremely costly. A study found that almost 2% of hospital admissions experienced a preventable adverse drug event, resulting in average increased hospital costs of $4,700 per admission, or about $2.8 million annually for a 700-bed teaching hospital. If these findings are generalizable, the increased costs of preventable adverse drug events for inpatients across the US could total about $2 billion.
Other examples of medical errors include wrong or delayed diagnoses, drug dosage miscalculations, surgical complications, and treatment delays. These errors can be attributed to inadequately skilled staff, errors in judgment or care, system defects, or preventable adverse effects such as computer breakdowns.
The issue of medical errors is compounded by a lack of accurate reporting and transparency. Death certificates and coroners' reports rarely list "medical errors" as the cause of death, making it difficult to determine the true extent of the problem. Additionally, studies tend to focus exclusively on hospitals rather than the broader healthcare system, and some errors may only have debilitating effects years later, making them harder to trace.
Despite these challenges, there is a growing movement towards improving patient safety and reducing errors. Many hospitals are implementing new technologies, such as electronic health records and fail-safe devices, to enhance patient safety. Additionally, most hospitals have active error-reduction programs, and medical care continues to improve through cutting-edge research. As a result, it is expected that in-hospital deaths will continue to decrease over time.
Drug Hospitalization: Patient Treatment and Care
You may want to see also
Explore related products






![]()
Inpatient death rates
The causes of inpatient deaths can be varied and complex. One of the most common causes is medical misdiagnosis or errors, which can lead to hundreds of thousands of deaths and permanent disabilities annually. These errors can include overlooking a disease, incorrect diagnosis, or delayed diagnosis. Other factors contributing to inpatient deaths include medical errors, such as medication errors, communication failures, and technical complications.
Additionally, sepsis, which is an inflammation throughout the body due to infection in the bloodstream, is a leading cause of death in hospitals. The treatment of sepsis is challenging due to the lack of a single definitive test, requiring doctors to rely on multiple factors for diagnosis. This complexity can lead to misallocation of medical resources and delayed treatment, often resulting in organ failure and other fatal complications.
It is important to note that the reduction in inpatient deaths may be attributed to improved treatment options and the availability of alternative care settings, such as hospice care. Patients and doctors are also becoming more aware that inpatient treatment is not always the best option, especially when considering the patient's quality of life. Furthermore, medical training is evolving to include topics like the futility of treatment and de-escalation, which can help reduce unnecessary inpatient interventions.
While inpatient death rates provide valuable insights into hospital performance and quality of care, they also highlight areas for improvement, such as reducing medical errors and improving diagnosis and treatment protocols for conditions like sepsis.
Hospitality Market: Growing Trends and Their Reasons
You may want to see also
Explore related products






![]()
Causes of death
Sepsis
Sepsis is the leading cause of death in hospitals. It is an inflammatory response to an infection in the bloodstream, often leading to organ failure and other fatal complications. The lack of a single test for sepsis makes diagnosis challenging, requiring a combination of medical history, symptoms, and various test results.
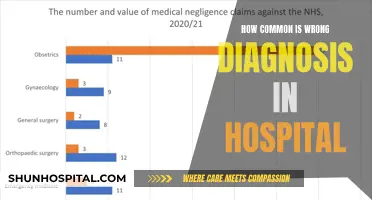
Medical Misdiagnosis and Errors
Medical misdiagnosis and errors are significant contributors to hospital deaths. Studies show that misdiagnoses lead to approximately 371,000 deaths annually, with 15 diseases accounting for about half of these cases. Additionally, other medical errors claim the lives of over 250,000 people each year, according to some estimates. These errors include issues like communication failures and preventable ailments during medical care.
Aggressive Life-Prolonging Interventions
In hospitals, aggressive life-prolonging interventions are sometimes administered even when a patient's death is expected. This can result in inadequate end-of-life care, as the focus of large hospitals is typically on healing and survival rather than palliative measures.
Age and Admission to a Medical Specialty
Statistical analyses have shown a correlation between the likelihood of death and factors such as age and admission to a medical specialty. In a Scottish study, it was found that out of 10,743 inpatients, 28.8% died during the follow-up period, with age being a significant predictor of mortality within 12 months.
Alternative Care Settings
The availability and acceptance of alternative care settings, such as hospice and community-based care, have contributed to the reduction of hospital deaths. A 2018 study found that compared to 2000, more people in 2015 chose to die at home or in community settings, while fewer people died in acute care hospitals.
Testing Strategies for the Delta Variant: A Hospital Guide
You may want to see also
Explore related products






![]()
End-of-life care
In the Western world, many healthcare providers lack knowledge about culturally and spiritually informed end-of-life care and report discomfort when engaging in religious discussions with people of differing beliefs. This may be why minorities access end-of-life care at lower rates than white people. However, engagement with end-of-life care services can improve when clinicians are educated on culturally and spiritually diverse beliefs, fostering better relationships and communication between healthcare providers, patients, and families.
The number of people admitted to the hospital during an end-of-life care program is unknown, and the impact of home-based end-of-life care on caregivers, healthcare staff, and health service costs is unclear. However, there is weak evidence that home-based end-of-life care may reduce healthcare costs. Not all groups have good access to end-of-life care, and people with severe mental illness, such as schizophrenia, bipolar disorder, or major depressive disorder, are unlikely to receive the most appropriate care.
In the United States, the number of patients who died in the hospital decreased from 2000 to 2010, with a significant drop from 2.5 deaths per 100 inpatients in 2000 to 2.0 deaths per 100 inpatients in 2010. However, there were still over 700,000 patients who died in the hospital in 2010. The decrease in inpatient hospital deaths may be due to improved treatment, increased availability and acceptability of alternative care sites, and a growing awareness that inpatient treatment is often futile in many situations.
Childbirth Reimbursement: Hospital, Lab, and Provider Expenses Covered
You may want to see also
Explore related products





![]()
Death certificates and reporting
Death certificates are a crucial component of the death reporting process, providing official documentation of an individual's death. In the United States, death certificates are typically obtained through the health department or the office of vital statistics in the relevant state or city. For instance, in Florida, death certificates can be obtained by visiting or mailing a request to the Florida Bureau of Vital Statistics, while in New York, death certificates are available from the local Registrar of Vital Statistics or the New York State Department of Health.
The process of obtaining a death certificate may vary slightly depending on the state and the applicant's relationship to the deceased. In some cases, only specific individuals, such as the spouse, parent, child, or sibling of the deceased, are eligible to receive a death certificate. Others may need to provide additional documentation, such as a will, insurance policy, or a notarized affidavit, to demonstrate their lawful right to the information.
The information required to obtain a death certificate includes the name of the deceased, the date of death or range of years to be searched, and valid photo identification of the applicant. There may be additional requirements or fees for requesting the cause of death, and in some states, death records with the cause of death are kept confidential for a specific period, such as 50 years in Florida.
Death certificates play a vital role in accurately reporting and recording deaths, which is essential for public health surveillance and understanding mortality trends. However, it is important to note that the accuracy of death certificates and coroners' reports has been called into question, particularly in cases of medical errors or misadventures, which may not always be noted as the cause of death.
The reduction in inpatient hospital deaths over the years could be attributed to improved treatments, increased availability of alternative care settings, and a growing awareness of the limitations of medical care in certain situations. As a result, patients and doctors are increasingly recognizing that more care is not always better care, and there is a growing movement to discuss end-of-life preferences and quality of life considerations.
Funding Not-for-Profit Hospitals: Where Does the Money Come From?
You may want to see also
Frequently asked questions
The percentage of deaths from all causes that occurred in a hospital decreased from 48% in 2000 to 35.1% in 2018. In 2010, 2 out of every 100 inpatients died in the hospital.
There could be several reasons for this, including improved treatment, increased availability of alternative care sites, and a growing awareness that more intensive treatment does not always lead to better outcomes.
Studies have shown that medical errors and adverse events are a leading cause of death in hospitals. As patient safety improves and doctors become better at recognizing when treatment is futile, inpatient hospital deaths are expected to decrease further.
Yes, late transitions of care, which occur when a patient is transferred to another care setting within three days of death, account for about 10% of cases. Additionally, death is often unpredictable, and inpatient deaths can occur after long admissions that begin with treatable problems.
Yes, drug complications, wound infections, technical complications, transfusion errors, adverse drug events, wrong-site surgery, surgical injuries, and more are all potential causes of preventable adverse events in hospitals.