Hospitals follow a rigorous and standardized protocol to determine brain death, a condition where all brain functions irreversibly cease. The process begins with a thorough clinical evaluation to rule out reversible causes of unresponsiveness, such as drug intoxication or hypothermia. If preliminary criteria are met, a neurologist or neurosurgeon performs a series of specific tests to confirm the absence of brainstem reflexes, such as pupil response to light, gag reflex, and corneal reflex. Additionally, an apnea test is conducted to assess the brain’s ability to control breathing. In some cases, ancillary tests like cerebral angiography, transcranial Doppler ultrasound, or EEG may be used to confirm the absence of blood flow or electrical activity in the brain. Two separate examinations, often performed by different physicians, are required to ensure accuracy, and the declaration of brain death must adhere to strict legal and ethical guidelines. This meticulous process ensures that the diagnosis is both definitive and compassionate, providing clarity for families and medical teams.
| Characteristics | Values |
|---|---|
| Clinical Evaluation | Absence of brainstem reflexes (e.g., pupillary, corneal, gag, cough reflexes). |
| Apnea Test | No respiratory effort observed when CO2 levels rise above a threshold. |
| Electroencephalogram (EEG) | Flat or isoelectric tracing, indicating no electrical activity in the brain. |
| Cerebral Angiography/Blood Flow Study | Absence of blood flow to the brain. |
| Transcranial Doppler (TCD) | No detectable blood flow in the brain vessels. |
| Somatosensory Evoked Potentials (SSEP) | No response to sensory stimuli. |
| Confirmation Period | Repeat tests after a specified time (e.g., 6–24 hours) to confirm irreversibility. |
| Exclusion of Reversible Causes | Rule out conditions like drug intoxication, hypothermia, or metabolic disorders. |
| Legal and Ethical Guidelines | Adherence to local laws and protocols for declaring brain death. |
| Neuroimaging (Optional) | CT or MRI may show irreversible brain damage, though not always required. |
Explore related products



$9.99



What You'll Learn
- Clinical Examination: Assessing reflexes, response to pain, and brainstem function through standardized neurological tests
- Apnea Test: Observing breathing cessation after CO2 buildup to confirm brainstem failure
- Imaging Studies: Using CT or MRI scans to detect brain herniation or irreversible damage
- EEG Monitoring: Recording brain electrical activity to confirm absence of neural function
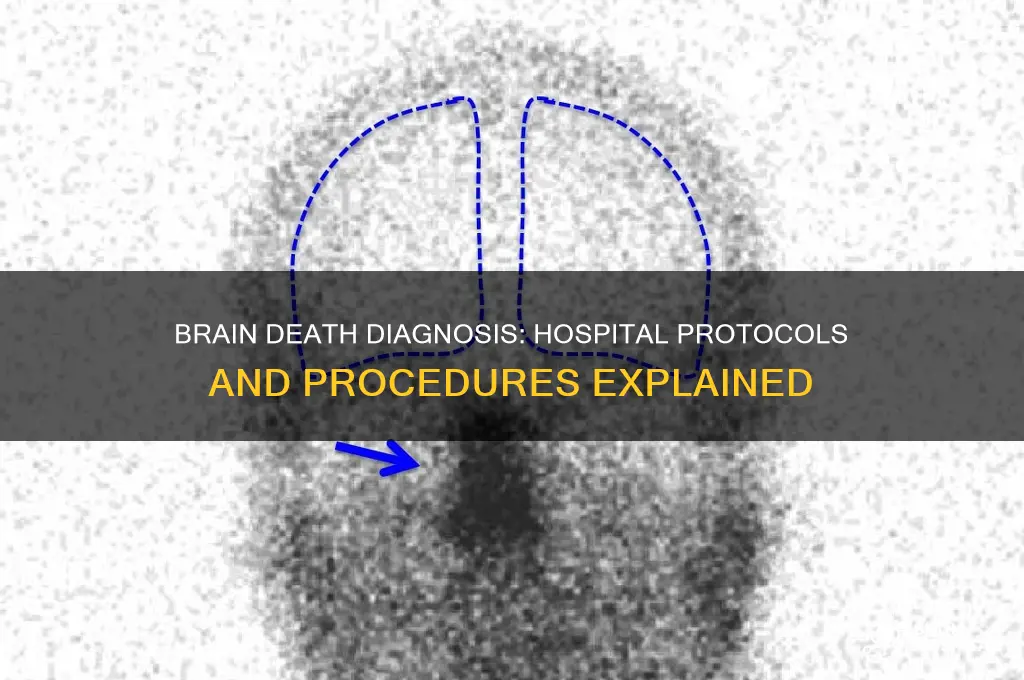
- Confirmatory Tests: Employing cerebral angiography or transcranial Doppler to verify absence of blood flow
![]()
Clinical Examination: Assessing reflexes, response to pain, and brainstem function through standardized neurological tests
When determining brain death, clinical examination plays a pivotal role in assessing the absence of brainstem function, reflexes, and response to pain. This process involves a series of standardized neurological tests conducted by trained medical professionals to ensure accuracy and consistency. The first step typically includes evaluating the patient’s reflexes, which are critical indicators of brainstem activity. The pupillary light reflex, for instance, is tested by shining a light into each eye to observe whether the pupils constrict. In brain death, the pupils are typically fixed and nonreactive to light due to the cessation of brainstem function. Similarly, the corneal reflex is assessed by gently touching the cornea with a sterile cotton swab; a normal response involves blinking, which is absent in brain-dead patients.
Another essential component of the clinical examination is the assessment of response to pain. Pain stimuli are applied to determine if the patient exhibits any motor responses mediated by the brainstem. This is done by applying firm pressure to the supraorbital ridge or nail bed, which would normally elicit a grimace, withdrawal, or other reflexive movements. In brain death, however, there is no observable response to these painful stimuli, as the brainstem no longer processes or reacts to such inputs. It is crucial to ensure that the absence of response is not due to sedation or neuromuscular blockade, which may require temporary suspension of such medications before testing.
The evaluation of brainstem function is further refined through additional standardized tests. The oculocephalic reflex, also known as the doll’s eye reflex, is performed by moving the patient’s head side to side while observing the eyes. In a normal individual, the eyes move in the opposite direction of the head movement, but in brain death, the eyes remain fixed. Similarly, the oculovestibular reflex (caloric test) involves irrigating the ear canal with ice-cold water, which should cause nystagmus (involuntary eye movement) in a functioning brainstem. Absence of nystagmus in both eyes confirms the loss of brainstem function.
Standardized neurological tests also include the assessment of respiratory drive, which is a key indicator of brainstem activity. The apnea test is conducted by temporarily removing mechanical ventilation and observing whether the patient makes any spontaneous respiratory effort. Pre-test conditions, such as specific blood gas levels and oxygen saturation, must be met to ensure the validity of the test. In brain death, there is no respiratory effort observed, even when carbon dioxide levels rise above a certain threshold. This test is often considered the gold standard for confirming the absence of brainstem function.
Throughout the clinical examination, it is imperative to rule out confounding factors such as drug intoxication, hypothermia, or severe metabolic abnormalities that might mimic brain death. Each test must be performed meticulously, and results must be consistently negative across multiple assessments to confirm the diagnosis. The process is repeated over time to ensure that the findings are irreversible. Clinical examination, when combined with other diagnostic modalities, provides a comprehensive and definitive determination of brain death, adhering to strict medical and ethical guidelines.
Hospital Rush: Alex Stokes' Health Scare Explained
You may want to see also
Explore related products





![]()
Apnea Test: Observing breathing cessation after CO2 buildup to confirm brainstem failure
The Apnea Test is a critical component of the brain death evaluation process, specifically designed to confirm the failure of the brainstem's respiratory centers. This test is conducted under strict medical supervision and involves a controlled environment to ensure accuracy and patient safety. The primary objective is to observe whether the patient exhibits any spontaneous respiratory effort after the buildup of carbon dioxide (CO2) in the bloodstream, which normally triggers the brainstem to initiate breathing. If no respiratory effort is detected, it provides strong evidence of brainstem failure, a key criterion for declaring brain death.
Before initiating the Apnea Test, the patient is pre-oxygenated to ensure adequate oxygen levels and to prevent hypoxia during the procedure. This is typically achieved by administering 100% oxygen for a sufficient period, usually 10 to 15 minutes, to saturate the lungs and blood with oxygen. Once pre-oxygenation is complete, the patient is disconnected from the ventilator, and a tracheal tube is inserted to maintain an open airway. A tight seal is ensured to prevent air leakage, as any external CO2 source could interfere with the test results.
The test begins by allowing the patient to breathe room air through the tracheal tube, without any mechanical assistance. Over time, the absence of ventilator support leads to a gradual increase in CO2 levels in the blood, a condition known as hypercapnia. Normally, the brainstem would detect this rise in CO2 and stimulate the diaphragm and intercostal muscles to initiate breathing. However, in cases of brainstem failure, this response is absent. Medical professionals closely monitor the patient's chest and abdomen for any signs of spontaneous breathing movements, using both visual observation and auscultation.
During the Apnea Test, additional parameters are continuously monitored to ensure patient safety and to validate the test results. These include oxygen saturation (SpO2), heart rate, blood pressure, and end-tidal CO2 (ETCO2) levels. The test is terminated if the patient's oxygen saturation drops below a predetermined threshold, typically 85%, or if other vital signs become unstable. If no respiratory effort is observed despite a significant rise in CO2 levels (usually confirmed by an ETCO2 above 60 mmHg), the test is considered positive, indicating brainstem failure.
It is important to note that the Apnea Test is just one part of a comprehensive brain death evaluation protocol, which also includes clinical examination for brainstem reflexes and, in some cases, ancillary tests such as cerebral blood flow studies. The Apnea Test must be performed meticulously, adhering to established guidelines, to ensure its reliability in confirming brain death. This procedure underscores the importance of a systematic and evidence-based approach in determining the irreversible cessation of brain function.
Preparing for a Hospital Stay: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Imaging Studies: Using CT or MRI scans to detect brain herniation or irreversible damage
Hospitals often employ advanced imaging techniques as a crucial step in determining brain death, providing visual evidence of severe and irreversible brain damage. Computed Tomography (CT) scans are frequently the initial imaging modality of choice due to their speed and availability in emergency settings. A CT scan can rapidly detect signs of brain herniation, a critical indicator of increased intracranial pressure and severe brain injury. This imaging technique uses X-rays to create detailed cross-sectional images of the brain, allowing doctors to identify shifts in brain tissue, compression of vital structures, and the presence of blood or fluid collections. For instance, the classic 'tonsillar herniation' can be visualized, where the cerebellar tonsils descend below the foramen magnum, a strong indicator of brainstem compromise.
Magnetic Resonance Imaging (MRI) is another powerful tool in the assessment of brain death, offering superior soft-tissue contrast and detailed anatomical visualization. MRI scans can detect subtle changes and provide a comprehensive evaluation of brain integrity. In the context of brain death, MRI is particularly useful in identifying irreversible damage, such as widespread cerebral edema, infarction, or hemorrhages. These scans can reveal the extent of brain injury, helping physicians determine if the damage is consistent with brain death. For example, the absence of blood flow in major cerebral vessels or the presence of diffuse axonal injury can be indicative of irreversible cessation of brain function.
Both CT and MRI scans play a pivotal role in supporting the clinical diagnosis of brain death by providing objective evidence of structural abnormalities. These imaging studies are essential in confirming the absence of brainstem reflexes and cortical function, which are key components in the neurological examination for brain death. By visualizing the brain's condition, these scans assist in ruling out conditions that might mimic brain death, ensuring an accurate and definitive diagnosis.
In practice, imaging studies are often performed after the initial clinical assessment, which includes a series of specific tests for brainstem reflexes and apnea evaluation. The results of CT or MRI scans, combined with the clinical findings, provide a comprehensive picture, enabling the medical team to make a confident determination of brain death. This multi-faceted approach ensures that the diagnosis is made with the utmost precision and care.
It is important to note that imaging alone cannot declare brain death; it is one of several critical components in the overall evaluation process. The interpretation of these scans requires specialized training, and radiologists play a vital role in analyzing the images and providing insights into the extent and nature of brain injuries. The use of CT and MRI scans in this context is a testament to the medical field's commitment to accuracy and the utilization of advanced technology in end-of-life assessments.
Strategies to Navigate Hospital Debt Collection
You may want to see also
Explore related products






![]()
EEG Monitoring: Recording brain electrical activity to confirm absence of neural function
Electroencephalography (EEG) monitoring is a critical tool used in hospitals to assess brain function, particularly when determining brain death. This non-invasive procedure involves recording the electrical activity of the brain through electrodes placed on the scalp. In cases of suspected brain death, EEG is employed to confirm the absence of neural function, providing essential data for clinical decision-making. The process begins with the careful placement of electrodes, ensuring optimal contact with the scalp to capture accurate signals. These electrodes detect the subtle electrical impulses generated by neurons, which are then amplified and recorded by the EEG machine.
During EEG monitoring for brain death, the primary goal is to identify whether there is any measurable brain activity. A normal EEG shows a variety of wave patterns corresponding to different states of consciousness, such as wakefulness or sleep. In contrast, a flat EEG, also known as a "silent" or "isoelectric" EEG, indicates a complete absence of electrical activity. This finding is a strong indicator of brain death, as it suggests that the cerebral cortex, the outer layer of the brain responsible for higher functions, is no longer functioning. However, a flat EEG alone is not sufficient to declare brain death; it must be corroborated by other clinical and diagnostic criteria.
The procedure for EEG monitoring in brain death cases is highly standardized to ensure reliability. The patient is typically disconnected from any sedative or paralytic medications that could suppress brain activity, as these can confound the results. The EEG recording is then performed for a minimum of 30 minutes, though longer durations may be necessary to rule out intermittent activity. Technologists and neurologists trained in interpreting EEGs analyze the results, looking for any signs of electrical discharge. If the EEG remains flat throughout the recording period, it provides compelling evidence of irreversible cessation of brain function.
EEG monitoring is particularly valuable because it directly assesses cortical activity, which is essential for consciousness and higher brain functions. While other tests, such as cerebral blood flow studies or clinical examinations, provide indirect evidence of brain death, EEG offers a direct measurement of neural activity. However, it is important to note that certain conditions, such as severe hypothermia or the use of specific medications, can mimic a flat EEG. Therefore, EEG results must always be interpreted in the context of the patient’s overall clinical picture and other diagnostic findings.
In summary, EEG monitoring plays a pivotal role in the evaluation of brain death by recording brain electrical activity to confirm the absence of neural function. A flat EEG, characterized by the complete absence of electrical impulses, is a key indicator of irreversible brain cessation. This procedure is conducted with precision, ensuring that all potential confounding factors are addressed. While EEG is a powerful tool, it is used in conjunction with other clinical and diagnostic criteria to definitively determine brain death. Its direct assessment of cortical activity makes it an indispensable component of the brain death evaluation process.
Where is the Good Doctor's Hospital Located?
You may want to see also
Explore related products






![]()
Confirmatory Tests: Employing cerebral angiography or transcranial Doppler to verify absence of blood flow
When determining brain death, confirmatory tests play a crucial role in verifying the absence of cerebral blood flow, a key indicator of irreversible brain function cessation. Two primary methods employed for this purpose are cerebral angiography and transcranial Doppler (TCD). These tests are highly specialized and provide definitive evidence to support the clinical diagnosis of brain death. Both techniques are designed to detect the absence of blood flow to the brain, which is a critical criterion for declaring brain death.
Cerebral angiography is an invasive but highly accurate procedure used to confirm brain death. It involves the injection of a contrast dye into the carotid and vertebral arteries, which supply blood to the brain. Under X-ray imaging, the flow of the contrast dye is observed in real time. In a brain-dead patient, there should be no detectable flow of the contrast dye into the intracranial vessels, indicating a complete absence of cerebral blood flow. This test is considered the gold standard for confirming brain death due to its precision, though it is reserved for cases where non-invasive methods are inconclusive or unavailable. The procedure requires expertise and careful monitoring, as it carries a small risk of complications, such as arterial injury or contrast reactions.
Transcranial Doppler (TCD) is a non-invasive alternative to cerebral angiography and is widely used as a confirmatory test for brain death. TCD employs ultrasound technology to measure blood flow velocity in the intracranial arteries. In a brain-dead patient, TCD should demonstrate a characteristic "flatline" or "zero-flow" pattern, indicating no detectable blood flow. This test is advantageous due to its ease of use, lack of radiation exposure, and ability to be performed at the bedside. However, its accuracy depends on the operator's skill and the patient's anatomical conditions, such as adequate temporal bone windows for ultrasound penetration. TCD is often used as an initial confirmatory test, with cerebral angiography reserved for cases where TCD results are ambiguous.
Both cerebral angiography and TCD are performed following a comprehensive clinical examination that establishes the absence of brainstem reflexes and unresponsiveness to stimuli. These tests are not standalone diagnostics but are used to corroborate clinical findings. The choice between the two methods depends on factors such as availability, patient condition, and institutional protocols. In all cases, the results must be interpreted by experienced professionals to ensure accuracy and adherence to brain death criteria.
In summary, cerebral angiography and transcranial Doppler are essential confirmatory tests for verifying the absence of cerebral blood flow in brain death determination. While cerebral angiography offers unparalleled accuracy, its invasiveness limits its use, making TCD a more practical and commonly employed option. Together, these tests provide critical evidence to support the diagnosis of brain death, ensuring a rigorous and ethical approach to this irreversible condition.
Understanding Incremental Unconscious Time Tracking in Hospital Settings
You may want to see also
Frequently asked questions
The process involves a series of clinical tests and observations to confirm the irreversible cessation of all brain function, including the brainstem. This includes checking for unresponsiveness, absence of brainstem reflexes (e.g., pupil reaction to light, gag reflex), and apnea (inability to breathe without mechanical support).
Brain death must be declared by a qualified physician, often a neurologist or intensivist, who follows strict guidelines and protocols. In some cases, a second physician may be required to confirm the diagnosis independently.
The process typically takes several hours to ensure accuracy. It involves repeated examinations, often with a waiting period between tests to rule out reversible conditions like drug intoxication or hypothermia.
No, brain death is irreversible. Once all brain function, including the brainstem, has ceased, there is no possibility of recovery.
After brain death is confirmed, the individual is legally and medically dead. The family may be approached about organ donation if the person is a registered donor or if the family consents. Life support is typically discontinued unless organ donation is pursued.































