Sickle cell anemia, a genetic blood disorder, is typically diagnosed at birth through newborn screening programs, which are mandatory in many countries. These programs involve collecting a small blood sample from the infant’s heel within the first 24 to 48 hours of life. The blood is then tested for the presence of abnormal hemoglobin (HbS), the hallmark of sickle cell anemia. Using techniques such as high-performance liquid chromatography (HPLC) or isoelectric focusing (IEF), laboratories can identify the specific types of hemoglobin present, including HbS. If the initial screening indicates the possibility of sickle cell anemia, confirmatory tests, such as DNA analysis or hemoglobin electrophoresis, are conducted to ensure an accurate diagnosis. Early detection is crucial, as it allows for prompt intervention, including preventive care, education, and treatment, to manage symptoms and improve long-term outcomes for affected infants.
| Characteristics | Values |
|---|---|
| Newborn Screening | Routine in many countries, including the U.S., U.K., and others. |
| Method | Blood spot test from a heel prick, typically collected 24–48 hours after birth. |
| Analyzed Biomarkers | Hemoglobin (Hb) types, including HbS (sickle hemoglobin). |
| Technology Used | Isoelectric focusing (IEF), high-performance liquid chromatography (HPLC), or DNA-based methods. |
| Detection | Identifies carriers (HbAS) and affected individuals (HbSS or HbSC). |
| Confirmation Testing | Follow-up tests (e.g., DNA analysis or hemoglobin electrophoresis) for positive screens. |
| Turnaround Time | Initial results within 1–2 weeks; confirmation may take additional time. |
| Parental Notification | Immediate notification for positive results to initiate early intervention. |
| Early Intervention | Prophylactic antibiotics, vaccinations, and education for affected infants. |
| Global Variability | Screening protocols and availability vary by country and healthcare system. |
| Advancements | Increasing use of DNA-based testing for more accurate and early detection. |
Explore related products






What You'll Learn
![]()
Newborn Screening Programs
The primary method used in newborn screening programs for sickle cell anemia is isoelectric focusing (IEF) or high-performance liquid chromatography (HPLC). These techniques analyze the types of hemoglobin present in the infant’s blood. Normal hemoglobin (HbA) is distinguished from abnormal forms such as hemoglobin S (HbS), which is associated with SCA. HPLC is particularly effective because it can detect not only HbS but also other hemoglobin variants, providing a comprehensive profile. If the initial screening indicates the presence of HbS or other abnormal hemoglobins, confirmatory testing is conducted to ensure accuracy. This may involve DNA-based tests to identify specific genetic mutations, such as the HBB gene mutation responsible for sickle cell anemia.
In addition to laboratory testing, newborn screening programs include a robust system for reporting and follow-up. Once a positive result is confirmed, healthcare providers are notified immediately to initiate further evaluation and management. Parents are also informed, and genetic counseling is often recommended to help families understand the implications of the diagnosis. Early intervention strategies, such as penicillin prophylaxis to prevent infections, folic acid supplementation, and comprehensive care plans, are implemented to mitigate the risks associated with SCA. These programs are supported by state and federal health departments, ensuring standardized protocols and quality control measures.
Education and awareness are integral components of newborn screening programs. Healthcare professionals are trained to explain the screening process and its importance to parents, addressing any concerns or misconceptions. Public health campaigns also play a role in raising awareness about sickle cell anemia, particularly in communities with higher prevalence rates, such as African American and Hispanic populations. By fostering understanding and cooperation, these programs enhance the likelihood of successful early detection and management.
Internationally, newborn screening for sickle cell anemia varies in availability and scope, but efforts are underway to expand access in regions with high disease prevalence, such as sub-Saharan Africa and parts of the Mediterranean. Collaborative initiatives between global health organizations, governments, and local healthcare providers aim to establish sustainable screening programs in resource-limited settings. These efforts often involve capacity building, technology transfer, and the development of cost-effective screening methods tailored to local needs. As newborn screening programs continue to evolve, their impact on reducing morbidity and mortality associated with sickle cell anemia remains a testament to the power of early diagnosis and intervention.
Avastin and Chemotherapy: Precautions for Hospitalized Patients
You may want to see also
Explore related products






![]()
Blood Sample Collection Methods
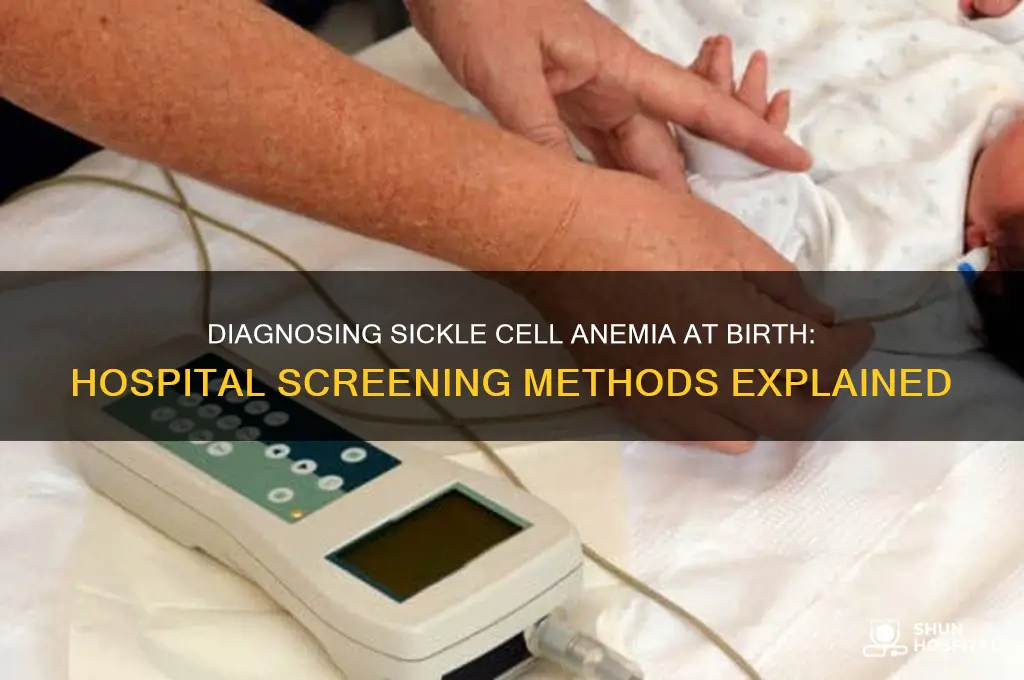
Hospitals employ specific blood sample collection methods to diagnose sickle cell anemia in newborns, ensuring accuracy and minimizing discomfort. One of the most common techniques is the heel stick method, also known as a Guthrie test. This procedure involves cleaning the baby’s heel with an antiseptic solution to prevent infection. A healthcare provider then uses a small, sterile lancet to prick the heel, drawing a few drops of blood. The blood is collected onto a specialized filter paper card, which is then sent to a laboratory for analysis. This method is widely used due to its simplicity, effectiveness, and minimal pain for the infant.
Another method utilized in some cases is venipuncture, though it is less common for newborns due to the difficulty of accessing small veins. If venipuncture is necessary, a trained phlebotomist or healthcare professional locates a suitable vein, typically in the scalp or hand, after cleaning the area with an antiseptic. A small needle is inserted to collect the blood directly into a tube. This method requires more skill and care to avoid complications and is generally reserved for situations where a larger blood sample is needed or when other methods are not feasible.
In certain regions or specialized settings, cord blood sampling may be used as an alternative method. Immediately after birth, a small amount of blood is collected from the umbilical cord before it is clamped and cut. This method is non-invasive for the newborn and provides a sufficient sample for testing. The blood is drawn using a needle and syringe or a specialized collection kit, ensuring sterility throughout the process. Cord blood sampling is particularly useful for early diagnosis and screening programs.
Regardless of the method chosen, proper handling and storage of the blood sample are critical. The collected blood must be promptly labeled with the infant’s identification details and transported to the laboratory under appropriate conditions to maintain sample integrity. For filter paper cards, the blood spots are allowed to air dry before being packaged and sent for analysis. In the case of cord blood or venipuncture samples, the tubes are sealed and stored according to laboratory protocols to prevent contamination or degradation.
Training and adherence to standardized protocols are essential for all blood collection methods. Healthcare providers must ensure that the procedure is performed quickly and efficiently to minimize stress and discomfort for the newborn. Parents are often informed about the process beforehand to alleviate concerns and ensure cooperation. These methods, when executed correctly, provide the necessary blood samples for diagnosing sickle cell anemia through specialized tests such as hemoglobin electrophoresis or DNA analysis.
Profit Hospitals in Minnesota: Are They Allowed?
You may want to see also
Explore related products





![]()
Hemoglobin Electrophoresis Testing
The process of hemoglobin electrophoresis begins with the collection of a small blood sample from the newborn, typically obtained via a heel prick. The sample is then processed in a laboratory, where the hemoglobin is extracted from the red blood cells. The extracted hemoglobin is placed on a gel or cellulose acetate medium and subjected to an electric current. Different hemoglobin types migrate at varying rates across the medium, creating distinct bands that correspond to specific hemoglobin variants. Normal adult hemoglobin (HbA), fetal hemoglobin (HbF), and abnormal hemoglobins like HbS are separated and visualized using staining techniques. The presence of HbS confirms the diagnosis of sickle cell anemia, while the presence of both HbS and HbC, for example, indicates sickle-hemoglobin C disease.
Hemoglobin electrophoresis is highly sensitive and specific, making it the gold standard for diagnosing sickle cell anemia and other hemoglobinopathies. It not only identifies the presence of abnormal hemoglobin but also quantifies the relative amounts of each hemoglobin type. This information is crucial for determining the severity of the condition and guiding treatment plans. For instance, newborns with a higher percentage of HbF may experience milder symptoms, as HbF inhibits the sickling of red blood cells. The test results are typically available within a few days, allowing healthcare providers to initiate appropriate care promptly.
In the context of newborn screening, hemoglobin electrophoresis is often performed as a follow-up to initial screening tests that detect abnormal hemoglobin levels. Many countries include sickle cell anemia in their mandatory newborn screening panels, using methods like isoelectric focusing or high-performance liquid chromatography (HPLC) as preliminary tests. If these initial screenings indicate the presence of abnormal hemoglobin, electrophoresis is conducted to confirm the diagnosis. This two-tiered approach ensures accuracy and minimizes false positives, providing families and healthcare providers with reliable information about the infant’s condition.
Early diagnosis through hemoglobin electrophoresis is essential for improving outcomes in children with sickle cell anemia. Once diagnosed, infants can begin receiving interventions such as penicillin prophylaxis to prevent infections, vaccinations, and education for caregivers about the condition. Additionally, early detection allows for genetic counseling and family planning discussions, as sickle cell anemia is an inherited disorder. By leveraging the precision of hemoglobin electrophoresis, hospitals play a vital role in identifying and managing sickle cell anemia from birth, setting the stage for lifelong care and support for affected individuals.
Oakland County's Hospitals: A Comprehensive Count
You may want to see also
Explore related products






![]()
DNA Analysis Techniques
Following PCR amplification, DNA sequencing is often employed to confirm the presence of the HbS mutation. Sanger sequencing, a traditional method, is commonly used to read the DNA sequence of the HBB gene and pinpoint the exact mutation. More recently, next-generation sequencing (NGS) has emerged as a powerful tool for diagnosing sickle cell anemia. NGS allows for the simultaneous analysis of multiple genes and can detect a broader range of mutations, including those associated with other hemoglobinopathies. This technique is particularly useful in populations with diverse genetic backgrounds, where additional mutations may be present.
Another critical DNA analysis technique is restriction fragment length polymorphism (RFLP), which identifies genetic variations by cutting DNA with specific enzymes and analyzing the resulting fragment lengths. While less commonly used today due to the advent of more advanced methods, RFLP remains a reliable technique for detecting the HbS mutation. It works by recognizing that the mutation alters the DNA sequence in a way that affects the enzyme’s ability to cut the DNA, resulting in distinct fragment patterns that indicate the presence of sickle cell anemia.
Allele-specific oligonucleotide (ASO) probes are also utilized in diagnosing sickle cell anemia. These probes are short, synthetic DNA fragments designed to bind specifically to the mutated HBB gene sequence. By hybridizing the ASO probe to the amplified DNA, laboratories can detect the presence of the HbS mutation with high accuracy. This method is often used in conjunction with PCR to enhance the specificity of the diagnosis.
Lastly, melting curve analysis is a rapid and cost-effective technique used to identify the HbS mutation. This method relies on monitoring changes in the fluorescence of double-stranded DNA as it melts into single strands at different temperatures. The presence of the mutation alters the melting profile, allowing for quick detection. While not as comprehensive as sequencing, melting curve analysis is valuable for initial screening and can be performed using real-time PCR instruments, making it accessible in many diagnostic settings.
In summary, DNA analysis techniques such as PCR, DNA sequencing, RFLP, ASO probes, and melting curve analysis are essential tools for diagnosing sickle cell anemia at birth. These methods provide accurate, early detection of the HbS mutation, enabling timely intervention and management of the condition. As technology advances, the integration of NGS and other innovative approaches continues to enhance the precision and efficiency of sickle cell anemia diagnosis.
Hospitality and Tourism: Exploring Industry Differences
You may want to see also
Explore related products




![]()
Confirmation and Follow-Up Procedures
Once an initial screening suggests the presence of sickle cell anemia in a newborn, confirmation and follow-up procedures are critical to ensure accurate diagnosis and timely intervention. The first step in confirmation is genetic testing, specifically through DNA analysis. This test identifies the specific mutations in the hemoglobin gene (HBB) that cause sickle cell anemia. Hospitals typically use polymerase chain reaction (PCR) or DNA sequencing to detect these mutations. This genetic confirmation is essential because it distinguishes sickle cell anemia (homozygous HbSS) from sickle cell trait (heterozygous HbAS) or other hemoglobinopathies. The results provide a definitive diagnosis, guiding appropriate medical management and counseling for the family.
Following genetic confirmation, additional laboratory tests are often conducted to assess the severity and implications of the condition. These include a complete blood count (CBC) to evaluate hemoglobin levels, red blood cell morphology, and signs of anemia. A peripheral blood smear may also be examined to identify sickle-shaped red blood cells, though this is less reliable in newborns due to the presence of fetal hemoglobin (HbF). Another important test is the hemoglobin electrophoresis, which quantifies the types of hemoglobin present in the blood. This test helps differentiate sickle cell anemia from other conditions and provides insights into disease progression.
Newborns diagnosed with sickle cell anemia are immediately enrolled in a comprehensive follow-up care program. This typically involves regular visits to a pediatric hematologist or a specialized sickle cell clinic. During these visits, healthcare providers monitor the child’s growth, development, and overall health. They also screen for complications such as infections, stroke risk, and organ damage. Prophylactic measures, such as daily penicillin administration until at least age 5, are initiated to prevent life-threatening infections, particularly from pneumococcus bacteria.
Parental education and support are integral to the follow-up process. Hospitals and healthcare providers educate families about sickle cell anemia, its management, and the importance of adhering to treatment plans. Parents are taught to recognize early signs of complications, such as fever, pain crises, or unusual fatigue, and are instructed on when to seek immediate medical attention. Genetic counseling is also offered to help families understand the hereditary nature of the condition and the risks in future pregnancies.
Finally, long-term management strategies are established to improve the child’s quality of life and reduce complications. This includes immunizations, folic acid supplementation to support red blood cell production, and hydration management. In some cases, hydroxylurea therapy may be initiated to increase fetal hemoglobin levels and reduce sickling episodes. Regular monitoring of blood parameters and organ function ensures early detection and intervention for any emerging issues. Through these confirmation and follow-up procedures, hospitals provide a robust framework for managing sickle cell anemia from birth, setting the stage for optimal health outcomes.
Prayers for Healing: Uplifting a Hospitalized Loved One
You may want to see also
Frequently asked questions
Sickle cell anemia is typically diagnosed at birth through newborn screening programs. A small blood sample is taken from the baby's heel within the first 24–48 hours of life and tested for the presence of abnormal hemoglobin (HbS), which is characteristic of sickle cell anemia.
If the newborn screening indicates a positive result, further tests such as hemoglobin electrophoresis or high-performance liquid chromatography (HPLC) are performed to confirm the diagnosis. These tests identify the specific types and amounts of hemoglobin present in the blood.
Yes, sickle cell anemia can be detected prenatally through tests like amniocentesis or chorionic villus sampling (CVS). These tests analyze fetal DNA to determine if the baby carries the genes for sickle cell anemia.
If a baby tests positive, they will be referred to a pediatrician or hematologist for further evaluation and management. Early intervention, including penicillin prophylaxis, vaccinations, and education for parents, is initiated to prevent complications and ensure proper care.