Hospitals play a crucial role in promoting bonding between parents and newborns, as well as among family members, by implementing various supportive practices and environments. From the moment of birth, hospitals often encourage skin-to-skin contact, also known as kangaroo care, which fosters immediate physical and emotional connection between the parent and baby. Additionally, many facilities offer private rooms or family-centered care models that allow families to stay together, providing uninterrupted time for bonding. Hospitals also provide educational resources, such as breastfeeding support and parenting classes, to empower families with the knowledge and confidence needed to nurture their relationships. By creating a nurturing and inclusive atmosphere, hospitals not only ensure the physical well-being of patients but also lay the foundation for strong, lasting familial bonds.
Explore related products






What You'll Learn
- Skin-to-skin contact initiatives for newborns and parents in the first hour after birth
- Rooming-in policies encouraging families to stay together throughout the hospital stay
- Breastfeeding support programs with lactation consultants and peer counseling services
- Parent education classes on newborn care, bonding techniques, and emotional support
- Quiet, family-centered environments minimizing disruptions to foster uninterrupted bonding moments
![]()
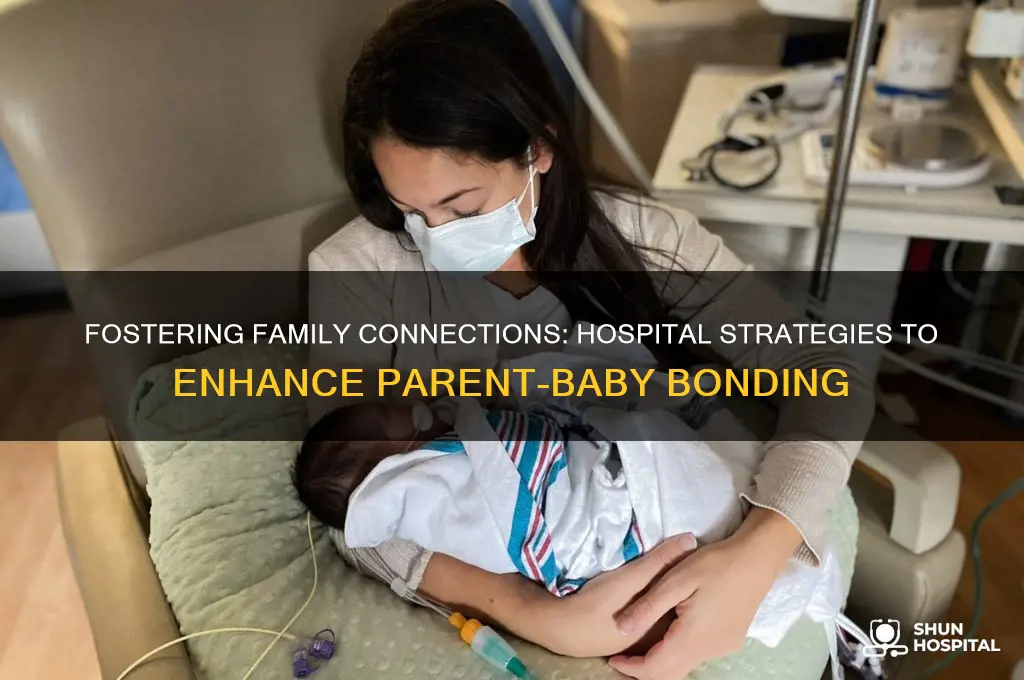
Skin-to-skin contact initiatives for newborns and parents in the first hour after birth
The first hour after birth is a critical window for newborns and parents, and skin-to-skin contact (SSC) during this period has been shown to have profound physiological and psychological benefits. Hospitals worldwide are increasingly adopting SSC initiatives as a standard practice, recognizing its role in promoting bonding, stabilizing vital signs, and fostering long-term health outcomes. For instance, the World Health Organization (WHO) recommends uninterrupted SSC for at least 60 minutes immediately after birth, regardless of delivery mode. This practice not only regulates the baby’s body temperature and heart rate but also releases oxytocin in parents, enhancing emotional connection and confidence in caregiving.
Implementing SSC initiatives requires careful planning and education. Healthcare providers must ensure the newborn is dried and placed prone on the parent’s bare chest, covered with a warm blanket, and monitored for signs of distress. For cesarean births, SSC should begin as soon as the parent is stable, often within 10–15 minutes post-delivery. Parents should be instructed to avoid using lotions or perfumes on their skin beforehand, as these can irritate the baby’s sensitive skin. Hospitals can support this practice by providing private, dimly lit spaces and encouraging partners or family members to participate, fostering a supportive environment for bonding.
One of the most compelling aspects of SSC is its impact on breastfeeding success. Studies show that newborns who experience SSC are more likely to latch effectively within the first hour, a critical factor in establishing breastfeeding. Hospitals can enhance this benefit by training staff to guide parents in recognizing feeding cues, such as lip-smacking or rooting, during SSC. Additionally, delaying routine procedures like weighing or bathing until after the first hour ensures uninterrupted contact, maximizing the benefits of this golden hour.
Despite its advantages, SSC initiatives face challenges, particularly in high-acuity settings or with premature infants. In such cases, modified SSC, where the baby is placed in an incubator with direct skin contact, can still promote bonding. Hospitals should develop protocols to address these scenarios, ensuring inclusivity for all families. For example, NICUs can encourage "kangaroo care," where parents hold their preterm infants skin-to-skin for extended periods, improving weight gain, sleep patterns, and overall development.
In conclusion, skin-to-skin contact initiatives in the first hour after birth are a powerful tool for hospitals to promote bonding and improve health outcomes. By prioritizing education, creating supportive environments, and adapting practices to diverse needs, healthcare providers can ensure that every family benefits from this simple yet transformative intervention. As hospitals continue to refine these initiatives, they not only enhance the immediate post-birth experience but also lay the foundation for strong, healthy parent-child relationships.
Managing a TB Outbreak in Hospitals: Protocols, Challenges, and Solutions
You may want to see also
Explore related products






![]()
Rooming-in policies encouraging families to stay together throughout the hospital stay
Hospitals increasingly adopt rooming-in policies, allowing families to stay with patients throughout their hospital stay, to foster emotional and physical healing. These policies, particularly in pediatric and maternity wards, recognize that family presence can significantly impact recovery. For instance, in neonatal intensive care units (NICUs), rooming-in enables parents to participate in their infant’s care, from feeding to monitoring vital signs, under professional guidance. This hands-on involvement not only strengthens the parent-child bond but also empowers families to care for their loved ones confidently post-discharge.
Implementing rooming-in policies requires careful planning to balance family needs with clinical protocols. Hospitals must provide adequate space, resources, and training for staff to support families effectively. For example, rooms should be equipped with sleeper chairs, privacy curtains, and educational materials to ensure comfort and engagement. Staff should receive training on how to involve families in care routines, such as medication administration or wound care, while maintaining safety standards. Clear communication about expectations and boundaries is essential to prevent misunderstandings and ensure a collaborative environment.
Critics argue that rooming-in policies may increase stress for families, particularly if they lack the physical or emotional capacity to stay overnight. Hospitals must address these concerns by offering flexible options, such as part-time rooming-in or access to nearby accommodations. Additionally, providing mental health support, such as counseling or support groups, can help families cope with the challenges of prolonged hospital stays. By acknowledging and mitigating potential drawbacks, hospitals can make rooming-in a positive experience for all involved.
The benefits of rooming-in extend beyond emotional bonding to include improved clinical outcomes. Studies show that patients with family present during their stay often experience reduced anxiety, better pain management, and shorter hospital durations. For example, in maternity wards, rooming-in promotes breastfeeding initiation and success, as mothers receive immediate support from nurses and partners. Similarly, pediatric patients with family involvement in their care report higher satisfaction and compliance with treatment plans. These outcomes highlight the transformative potential of rooming-in policies when thoughtfully implemented.
To maximize the effectiveness of rooming-in, hospitals should gather feedback from families and staff to continuously refine their approach. Surveys, focus groups, and regular meetings can identify areas for improvement, such as enhancing privacy or expanding educational resources. Hospitals might also consider offering incentives, like meal vouchers or discounted parking, to alleviate the financial burden of extended stays. By prioritizing family-centered care, rooming-in policies not only promote bonding but also redefine the hospital experience as a collaborative, healing journey for patients and their loved ones.
Where to Purchase Hospital-Grade Glass Bassinets: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Breastfeeding support programs with lactation consultants and peer counseling services
Hospitals increasingly recognize that breastfeeding support is a cornerstone of promoting early bonding between parents and newborns. Breastfeeding support programs, which often include lactation consultants and peer counseling services, address the physical, emotional, and practical challenges new parents face. These programs are designed to empower parents, ensuring they feel confident and supported during the critical early days and weeks of their baby’s life. By fostering successful breastfeeding, hospitals not only enhance infant health but also strengthen the emotional connection between parent and child.
Lactation consultants play a pivotal role in these programs, offering evidence-based guidance tailored to individual needs. Certified by the International Board of Lactation Consultant Examiners (IBLCE), these professionals assess latching techniques, milk transfer, and infant behavior to identify and resolve breastfeeding difficulties. For instance, a consultant might recommend specific positions, such as the football hold for small babies or side-lying for nighttime feeds, to improve comfort and efficiency. They also educate parents on topics like breast milk storage (up to 4 hours at room temperature, 4 days in the refrigerator, or 6 months in a deep freezer) and the signs of adequate milk intake (e.g., 6–8 wet diapers per day in the first month). This clinical expertise builds parental confidence, reducing anxiety and fostering a positive breastfeeding experience.
Peer counseling services complement the work of lactation consultants by providing emotional support and practical advice from individuals who have firsthand experience with breastfeeding. These counselors, often trained through programs like the *Special Supplemental Nutrition Program for Women, Infants, and Children (WIC)*, offer relatable insights and encouragement. For example, a peer counselor might share strategies for managing engorgement, such as applying cold cabbage leaves or expressing milk manually before latching. They also create safe spaces for parents to discuss concerns, from nipple pain to fears of insufficient milk supply. This combination of empathy and practical tips helps parents feel less isolated, reinforcing their commitment to breastfeeding and, by extension, their bond with their baby.
The integration of lactation consultants and peer counselors into hospital-based breastfeeding programs yields measurable benefits. Studies show that parents who receive such support are more likely to initiate breastfeeding within the first hour of life—a critical window for bonding and colostrum transfer. Additionally, these programs correlate with higher exclusive breastfeeding rates at 6 months, aligning with World Health Organization recommendations. Hospitals that invest in these services not only improve maternal and infant health outcomes but also lay the foundation for strong, nurturing relationships that last a lifetime. By addressing both the technical and emotional aspects of breastfeeding, these programs transform the hospital stay into a transformative bonding experience.
Beyond MRSA: Deadlier Hospital-Acquired Infections You Need to Know
You may want to see also
Explore related products


$17.14 $21.99

$12.5 $19.99



![]()
Parent education classes on newborn care, bonding techniques, and emotional support
Hospitals increasingly recognize that the first hours and days after birth are critical for establishing a strong parent-child bond. Parent education classes emerge as a proactive strategy to empower new families during this pivotal period. These classes, often integrated into postpartum care, cover essential newborn care skills, evidence-based bonding techniques, and emotional support strategies. By equipping parents with practical knowledge and confidence, hospitals foster a nurturing environment that strengthens early connections.
Consider the structure of these classes: typically, they are divided into modules addressing specific needs. Newborn care sessions might include demonstrations on diapering, bathing, and feeding, with hands-on practice using dolls or real-life scenarios. Bonding techniques often highlight skin-to-skin contact, babywearing, and responsive communication, emphasizing the science behind these practices. For instance, skin-to-skin contact for at least 60 minutes after birth stabilizes the baby’s temperature, heart rate, and breathing while releasing oxytocin in parents, promoting attachment. Emotional support modules focus on recognizing postpartum mood changes, stress management, and building a support network, ensuring parents feel prepared for the emotional demands of early parenthood.
The effectiveness of these classes lies in their tailored approach. Hospitals often adapt content to diverse family structures, cultural backgrounds, and individual learning styles. For example, visual aids, translated materials, and one-on-one sessions cater to non-English speakers or those with specific needs. Additionally, classes may incorporate partners or extended family members, acknowledging their role in the support system. This inclusivity ensures that all caregivers are equipped to contribute to the baby’s well-being and the family’s bonding process.
A critical aspect of these programs is their emphasis on practical application. Parents are encouraged to practice techniques in the hospital setting under guidance, such as swaddling or interpreting a baby’s cues. This immediate feedback loop builds confidence and reduces anxiety. Hospitals also provide take-home resources, like step-by-step guides or access to online tutorials, ensuring parents can reinforce skills once they return home. Such continuity bridges the gap between hospital care and independent parenting, fostering a smoother transition.
Ultimately, parent education classes serve as a cornerstone in hospital-led bonding initiatives. By combining evidence-based practices with personalized support, these programs not only educate but also empower families to navigate the complexities of newborn care. The result is a stronger foundation for parent-child relationships, setting the stage for long-term emotional and developmental health. Hospitals that invest in such classes demonstrate a commitment to holistic care, recognizing that bonding is as vital as physical health in the postpartum journey.
Hospital Environmental Services: Ensuring Sanitation and Safety
You may want to see also
Explore related products





![]()
Quiet, family-centered environments minimizing disruptions to foster uninterrupted bonding moments
Hospitals are increasingly recognizing the importance of creating environments that prioritize family-centered care, particularly in the context of fostering bonding between parents and newborns. One critical aspect of this approach is the design and management of quiet spaces that minimize disruptions, allowing families to focus on building emotional connections without unnecessary interruptions. For instance, some hospitals have implemented "quiet hours" during which non-essential activities, such as housekeeping or routine checks, are paused to ensure uninterrupted family time. These designated periods often align with peak bonding times, such as early mornings or late evenings, when parents are most likely to engage in skin-to-skin contact or breastfeeding.
To achieve this, hospitals must carefully consider the physical layout of their facilities. Rooms designed for family-centered care often feature soundproof walls, dimmable lighting, and comfortable seating areas to create a serene atmosphere. For example, the use of acoustic panels and soft furnishings can significantly reduce noise levels, while adjustable lighting allows families to customize the environment to their comfort. Additionally, hospitals are incorporating private bathrooms and sleeping accommodations for partners or family members, ensuring that caregivers can remain close to the newborn without sacrificing their own rest or privacy. These design choices not only enhance bonding but also reduce stress for both parents and infants.
A key challenge in maintaining quiet, family-centered environments is managing the flow of medical staff and visitors. Hospitals are addressing this by implementing clear communication protocols and training staff to respect the sanctity of family time. For instance, nurses are encouraged to consolidate care activities into fewer visits, minimizing disruptions while ensuring all necessary medical tasks are completed. Visitor policies are also being revised to limit the number of guests and establish specific visiting hours, often with exceptions for immediate family members. By balancing medical needs with the emotional needs of families, hospitals can create a harmonious environment that supports bonding.
Practical tips for families can further enhance the effectiveness of these quiet environments. Parents are often advised to bring personal items, such as familiar blankets or music, to create a sense of home within the hospital setting. Hospitals may also provide resources like white noise machines or guided meditation apps to help families relax and focus on bonding. For parents of preterm infants or those in NICUs, hospitals are offering specialized training on how to interact with their babies in ways that promote development and connection, even in a high-tech medical environment. These small but impactful measures ensure that every moment spent together contributes to a strong foundation for the family.
Ultimately, the goal of quiet, family-centered environments is to empower families to form deep, lasting bonds during their hospital stay. By minimizing disruptions and prioritizing emotional well-being, hospitals are not only improving the immediate experience of new parents but also laying the groundwork for healthier family dynamics in the long term. As healthcare continues to evolve, the emphasis on creating such environments underscores a broader shift toward holistic, patient-centered care that values the emotional and psychological aspects of healing as much as the physical.
Residents at Hahnemann: A Comprehensive Count
You may want to see also
Frequently asked questions
Hospitals promote immediate bonding by practicing skin-to-skin contact (also known as kangaroo care), encouraging breastfeeding, and allowing uninterrupted time for parents to hold and interact with their newborn in a quiet, private environment.
Rooming-in, where the baby stays in the same room as the parent(s) instead of a nursery, allows for constant proximity and opportunities for interaction, fostering emotional connection and confidence in caregiving.
Hospitals in the NICU promote bonding by encouraging parents to participate in caregiving (e.g., diaper changes, feeding), providing private spaces for skin-to-skin contact, and offering emotional support and education to help families stay connected with their baby.






























