The removal of bodily fluids, or fmuid, from hospital rooms is a critical aspect of maintaining a sterile and safe environment for patients and healthcare workers. This process involves a combination of specialized cleaning protocols, personal protective equipment (PPE), and advanced disinfection techniques. Hospital staff are trained to promptly clean and disinfect surfaces contaminated with blood, urine, or other fluids using EPA-approved disinfectants, while also ensuring proper disposal of biohazardous waste. Additionally, the use of barrier protection, such as gloves and gowns, minimizes the risk of exposure to infectious materials. Regular audits and adherence to infection control guidelines further ensure that hospital rooms remain free from harmful pathogens, promoting a healthier and safer healthcare setting.
Explore related products






What You'll Learn
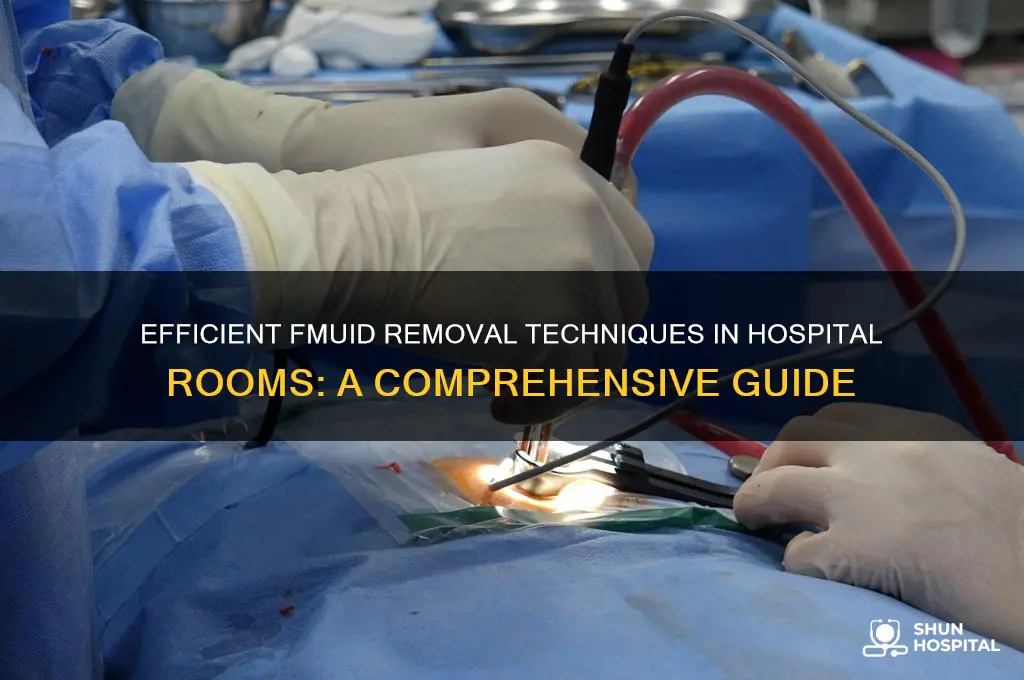
- Suction Devices: Use of portable or wall-mounted suction machines to remove fluids quickly and safely
- Chest Tubes: Insertion of tubes to drain fluid or air from the pleural cavity post-surgery
- Wound Drains: Placement of drains in surgical sites to collect and remove excess fluid
- Catheter Systems: Urinary or surgical catheters to drain fluids from the bladder or abdominal areas
- Manual Aspiration: Use of syringes or needles to extract localized fluid collections under sterile conditions
![]()
Suction Devices: Use of portable or wall-mounted suction machines to remove fluids quickly and safely
In hospital settings, the removal of fluids from patients' bodies is a critical procedure often facilitated by suction devices. These devices, whether portable or wall-mounted, are designed to efficiently and safely extract fluids such as blood, saliva, mucus, or other bodily secretions. Portable suction machines are particularly useful in emergency situations or when patients need to be transported, as they provide mobility and immediate access to suction capabilities. These units are battery-operated or electrically powered, ensuring they can function in various environments, including ambulances, patient rooms, and operating theaters. Wall-mounted suction machines, on the other hand, are stationary units commonly found in hospital rooms, intensive care units (ICUs), and surgical suites. They offer consistent, powerful suction and are directly connected to the hospital's vacuum system, eliminating the need for frequent maintenance or recharging.
The use of suction devices begins with selecting the appropriate equipment for the patient's needs. This includes choosing the correct catheter size and type, such as a Yankauer suction tip for oral secretions or a surgical suction catheter for deeper fluid removal. The catheter is connected to the suction device via tubing, and the machine is activated to create a vacuum. Healthcare providers must carefully regulate the suction pressure to avoid tissue damage, typically using a control mechanism on the machine. For portable devices, ensuring the unit is fully charged or connected to a power source is essential before initiating the procedure. Wall-mounted units require verification that the hospital's central vacuum system is operational and delivering adequate suction power.
During the suctioning process, the healthcare provider inserts the catheter into the patient's airway, wound, or surgical site, taking care to minimize discomfort and trauma. The suction is applied intermittently to prevent tissue damage and ensure effective fluid removal. In cases of airway clearance, such as in patients with respiratory distress, the provider may use a sterile technique to reduce the risk of infection. The duration and frequency of suctioning depend on the patient's condition and the volume of fluid to be removed. Continuous monitoring of the patient's vital signs, such as oxygen saturation and heart rate, is crucial to ensure safety during the procedure.
Maintenance and cleaning of suction devices are paramount to prevent cross-contamination and ensure optimal performance. After each use, the catheter and tubing must be disposed of or sterilized according to hospital protocols. Portable suction machines require regular checks of their battery life, filters, and overall functionality. Wall-mounted units should be inspected for any leaks in the vacuum system and cleaned to remove any debris or fluid buildup. Healthcare facilities often have dedicated staff or protocols for the routine maintenance of these devices to ensure they are always ready for use.
Training healthcare providers in the proper use of suction devices is essential to maximize safety and efficiency. This includes understanding the mechanics of the machine, selecting the right equipment, and applying suction techniques that minimize patient discomfort and risk. Hospitals often conduct regular training sessions and provide guidelines to ensure staff are competent in using both portable and wall-mounted suction machines. By adhering to best practices, healthcare providers can effectively manage fluid removal, improving patient outcomes and maintaining a high standard of care in hospital rooms.
Scripps Hospital: A Name, A Legacy
You may want to see also
Explore related products






![]()
Chest Tubes: Insertion of tubes to drain fluid or air from the pleural cavity post-surgery
Chest tubes are a critical intervention used to drain fluid or air from the pleural cavity, the space surrounding the lungs, particularly after surgical procedures. This process is essential to prevent complications such as pneumothorax (air in the pleural cavity) or pleural effusion (excess fluid accumulation), which can impair lung function and patient recovery. The insertion of chest tubes is a carefully executed procedure that requires precision and adherence to sterile techniques to minimize infection risk and ensure effective drainage. Typically, the procedure is performed in an operating room or at the bedside in critical care settings, depending on the patient's condition and the urgency of the intervention.
The insertion of a chest tube begins with the selection of the appropriate tube size and type, which depends on the patient's age, the nature of the fluid or air to be drained, and the specific surgical context. Common sites for chest tube insertion include the fifth or sixth intercostal space in the mid-axillary line, though the location may vary based on the underlying condition. Before insertion, the patient is positioned appropriately, often in a semi-seated or supine position, and the skin over the insertion site is cleaned with antiseptic solutions to reduce the risk of infection. Local anesthesia is administered to numb the area, ensuring patient comfort during the procedure.
Once the site is prepared, a small incision is made through the skin and muscle layers to access the pleural cavity. The chest tube is then carefully advanced into the cavity, guided by anatomical landmarks and, in some cases, imaging techniques like ultrasound to ensure proper placement. The tube is secured to the skin using sutures or specialized dressings to prevent dislodgment and maintain a watertight seal. The distal end of the tube is connected to a drainage system, which may include a water seal or digital drainage device, to facilitate the removal of fluid or air while preventing backflow into the pleural cavity.
Post-insertion care is crucial to the success of chest tube drainage. The drainage system must be monitored regularly to ensure it is functioning correctly and to measure the volume and characteristics of the drained fluid or air. Patients are also observed for signs of complications, such as infection, bleeding, or tube malposition. Pain management is an important aspect of care, as chest tubes can cause discomfort, particularly during coughing or deep breathing. Once the drainage decreases significantly and imaging confirms resolution of the pneumothorax or effusion, the chest tube can be removed in a controlled manner to avoid complications.
The removal of a chest tube involves clamping the tube, removing the sutures, and quickly pulling the tube out during expiration to minimize discomfort and the risk of air entering the pleural cavity. The insertion site is then covered with a sterile dressing, and the patient is monitored for any signs of recurrence or complications. Chest tube insertion and management are integral components of post-surgical care, particularly in thoracic and cardiac surgeries, where they play a vital role in promoting lung re-expansion and preventing respiratory complications. Proper technique, vigilant monitoring, and patient education are key to ensuring successful outcomes with this intervention.
Quarantine Preparedness: Are All NJ Hospitals Equipped?
You may want to see also
Explore related products






![]()
Wound Drains: Placement of drains in surgical sites to collect and remove excess fluid
Wound drains are essential tools in surgical care, designed to collect and remove excess fluid that accumulates in surgical sites. This fluid, which can include blood, serum, or other bodily fluids, may hinder the healing process if left unchecked. The placement of drains is a critical step in post-operative management, particularly in procedures where fluid buildup is anticipated, such as abdominal surgeries, orthopedic reconstructions, or procedures involving significant tissue dissection. Drains are typically inserted by the surgeon during the operation and positioned in areas where fluid is most likely to collect. The primary goal is to prevent complications such as hematomas, seromas, or infections, which can arise from fluid accumulation.
The process of placing wound drains involves careful consideration of the surgical site’s anatomy and the type of fluid expected. Drains come in various forms, including Jackson-Pratt (bulb) drains, Blake drains, and Penrose drains, each suited to different clinical scenarios. For example, Jackson-Pratt drains are commonly used for closed wound drainage, while Penrose drains are more suitable for open wounds. The drain is inserted through a small incision or existing surgical opening and secured in place with sutures to ensure it remains stable. The distal end of the drain is connected to a collection device, such as a bulb or vacuum-assisted system, which allows for continuous or intermittent drainage.
Proper placement of wound drains requires precision to ensure they are positioned in the area of highest fluid accumulation without causing additional tissue trauma. Surgeons often use imaging techniques, such as ultrasound or direct visualization, to guide drain placement. Once inserted, the drain is tested to confirm it is functioning correctly by applying gentle suction or squeezing the collection bulb to ensure fluid flows freely. The surgical team also ensures the drain is labeled and documented in the patient’s chart to monitor output and assess the need for removal.
Post-operative care of wound drains is crucial for their effectiveness and patient comfort. Nurses and healthcare providers monitor the drain output regularly, noting the volume, color, and consistency of the fluid. Excessive bleeding, foul odor, or sudden changes in output may indicate complications such as infection or drain malfunction, requiring immediate attention. Patients are educated on how to care for their drains at home, including emptying and recording output, maintaining cleanliness, and recognizing signs of problems. Pain management is also addressed, as drain sites can be tender.
The removal of wound drains is guided by clinical judgment and specific criteria, such as minimal output over 24 hours or evidence of adequate wound healing. Before removal, the drain site is assessed to ensure there is no ongoing fluid collection. The drain is then carefully extracted, and the site is dressed to prevent infection. Patients are monitored after drain removal to ensure there is no recurrence of fluid accumulation. Wound drains play a vital role in facilitating recovery by managing post-surgical fluid, but their success depends on precise placement, vigilant monitoring, and appropriate timing of removal.
Hospitals Need a Marshall Plan: Funding, Staffing, and Support
You may want to see also
Explore related products






![]()
Catheter Systems: Urinary or surgical catheters to drain fluids from the bladder or abdominal areas
In hospital settings, catheter systems play a crucial role in removing fluids from the body, particularly from the bladder or abdominal areas. Urinary catheters are commonly used to drain urine from the bladder when a patient is unable to urinate naturally due to conditions like urinary retention, surgery, or neurological disorders. These catheters are typically made of flexible materials like silicone or latex and are inserted through the urethra into the bladder. The process involves lubricating the catheter, carefully advancing it to the bladder, and then connecting it to a drainage bag that collects the urine. This system ensures continuous or intermittent drainage, preventing fluid buildup and reducing the risk of infection or discomfort.
Surgical catheters, on the other hand, are used to drain fluids from the abdominal cavity or other surgical sites. These catheters, often referred to as abdominal drains or surgical drains, are placed during or after surgical procedures to remove blood, pus, or other fluids that accumulate post-operation. They are typically inserted directly into the abdominal area or near the surgical site and connected to a collection device. The placement of these catheters requires precision to ensure effective drainage without causing damage to surrounding tissues. Surgical catheters are essential in preventing complications such as abscesses or hematomas, which can arise from fluid accumulation.
The insertion and management of both urinary and surgical catheters require strict adherence to sterile techniques to minimize infection risk. Healthcare providers must ensure proper hand hygiene, use sterile equipment, and follow protocols for catheter placement and maintenance. For urinary catheters, this includes securing the catheter to prevent movement and regularly emptying and cleaning the drainage bag. For surgical catheters, monitoring the type and amount of fluid drained is critical to assess the patient’s recovery progress and identify any abnormalities, such as excessive bleeding or infection.
Catheter systems are also designed with patient comfort and safety in mind. Modern catheters often feature rounded tips and smooth surfaces to minimize tissue irritation during insertion and use. Additionally, some urinary catheters are equipped with balloons that inflate inside the bladder to hold the catheter in place, reducing the risk of dislodgment. For long-term use, healthcare providers may opt for suprapubic catheters, which are inserted directly into the bladder through a small incision in the abdomen, bypassing the urethra and offering a more comfortable and discreet option for patients.
In summary, catheter systems are indispensable tools in hospital fluid management, particularly for draining the bladder or abdominal areas. Whether urinary or surgical, these catheters are carefully selected, inserted, and maintained to ensure effective fluid removal while minimizing complications. Proper training and adherence to protocols are essential for healthcare providers to optimize patient outcomes and ensure the safe and efficient use of catheter systems in clinical practice.
Hospital Car Seat Checks: What to Expect
You may want to see also
Explore related products





![]()
Manual Aspiration: Use of syringes or needles to extract localized fluid collections under sterile conditions
Manual aspiration using syringes or needles is a common and effective method for removing localized fluid collections from patients in hospital settings. This procedure is typically performed under sterile conditions to minimize the risk of infection and ensure patient safety. The process begins with a thorough assessment of the fluid collection site, including its size, location, and characteristics, to determine the most appropriate approach. Sterile gloves are worn, and the area is cleaned with an antiseptic solution, such as chlorhexidine or iodine, to reduce microbial contamination. A sterile drape may also be used to create a clean field around the aspiration site.
Once the area is prepared, a suitable needle or syringe is selected based on the size and depth of the fluid collection. For superficial collections, a fine-gauge needle (e.g., 22–25 gauge) attached to a syringe is often sufficient. For deeper or larger collections, a larger bore needle or catheter may be required to facilitate efficient drainage. The needle is inserted into the fluid collection using a steady, controlled motion, guided by palpation or ultrasound if necessary. Ultrasound guidance is particularly useful for deeper or less palpable collections, as it allows for real-time visualization of the needle and fluid pocket, reducing the risk of complications such as organ puncture or vascular injury.
After the needle is properly positioned, the syringe is used to create negative pressure, drawing the fluid into the syringe. The procedure is performed slowly to avoid tissue damage and ensure complete drainage. If the collection is large, multiple aspirations or a larger syringe may be needed. Once the fluid is extracted, the needle is carefully withdrawn, and pressure is applied to the site to prevent bleeding or leakage. The aspirated fluid may be sent for laboratory analysis, such as cell count, culture, or cytology, depending on the clinical context.
Sterile technique is maintained throughout the procedure to minimize infection risk. All equipment used, including needles, syringes, and dressings, is single-use and disposed of appropriately. The patient’s vital signs are monitored during and after the procedure, and they are observed for any signs of discomfort, bleeding, or adverse reactions. Manual aspiration is particularly useful for conditions such as abscesses, seromas, or localized edema, where prompt removal of fluid can alleviate symptoms and prevent complications.
While manual aspiration is generally safe, potential complications include infection, bleeding, pain, or injury to surrounding structures. Proper training and adherence to sterile protocols are essential to minimize these risks. In cases where the fluid collection is recurrent or difficult to access, alternative methods such as catheter drainage or surgical intervention may be considered. Overall, manual aspiration remains a valuable tool in hospital settings for the efficient and targeted removal of localized fluid collections.
Hospitals and Public Records: What's the Law?
You may want to see also
Frequently asked questions
FMUID stands for "Fluids of Microbial and Unknown Identity," which includes bodily fluids like blood, urine, or saliva that may contain pathogens. Removing FMUID is critical to prevent the spread of infections, maintain hygiene, and ensure patient safety in healthcare settings.
FMUID is removed using specialized cleaning protocols. This involves wearing personal protective equipment (PPE), using disinfectants approved for healthcare settings (e.g., bleach or hydrogen peroxide), and following a two-step process: cleaning visible soiling first, then disinfecting the area to kill pathogens.
Trained environmental services (EVS) staff or housekeeping personnel are responsible for removing FMUID. They follow strict guidelines from infection control teams and use appropriate tools and chemicals to ensure thorough decontamination.


![McKesson Bloodborne Pathogen Spill Kit [1 Kit]– Bodily Fluid Clean-Up Pack with Gloves, Hand Wipes, Disinfectant & Fluid Solidifier – First Response Spill Kit for Workplace, School & Medical Use](https://m.media-amazon.com/images/I/71k1+VU4QQL._AC_UL320_.jpg)