The United States healthcare system is vast and complex, comprising numerous hospital groups that play a critical role in delivering medical services across the country. Understanding how many hospital groups exist in the U.S. requires examining the diverse landscape of healthcare providers, which includes nonprofit, for-profit, and public hospitals, as well as large integrated health systems. As of recent data, there are over 6,000 hospitals in the U.S., many of which are organized into larger groups or networks, such as HCA Healthcare, CommonSpirit Health, and Ascension. These groups vary in size, scope, and ownership, reflecting the fragmented yet interconnected nature of American healthcare. Determining the exact number of hospital groups involves considering consolidation trends, regional differences, and the evolving structure of the industry, making it a dynamic and multifaceted topic.
Explore related products




$19.99 $49.95


What You'll Learn
![]()
Total Number of Hospital Groups
The United States healthcare landscape is fragmented, with hospital groups playing a pivotal role in delivering care. As of recent data, there are approximately 6,100 hospitals in the U.S., but these are not standalone entities. Many are consolidated under larger hospital groups or health systems, which manage multiple facilities across regions. For instance, HCA Healthcare operates over 180 hospitals, while CommonSpirit Health oversees nearly 140. This consolidation trend has accelerated, reducing the number of independent hospitals and increasing the dominance of large groups. Understanding this structure is crucial for patients, policymakers, and healthcare professionals navigating the system.
Analyzing the data reveals a significant shift toward consolidation over the past two decades. In the early 2000s, smaller, independent hospitals were more common, but financial pressures and the need for economies of scale have driven mergers and acquisitions. Today, the top 10 hospital groups control over 20% of all U.S. hospitals, a statistic that underscores the concentration of power in the industry. This trend has implications for competition, pricing, and access to care, as larger groups often negotiate better rates with insurers but may limit patient choice in certain regions.
For those seeking care, knowing which hospital group operates in their area can be practical. For example, Kaiser Permanente operates in specific states like California and Colorado, offering integrated care models, while Tenet Healthcare has a broader national presence. Patients can use tools like the American Hospital Directory to identify hospital affiliations and make informed decisions. Additionally, understanding a group’s specialty—whether it’s pediatric care, trauma services, or rural health—can guide treatment choices.
From a policy perspective, the consolidation of hospital groups raises concerns about monopolistic practices and healthcare disparities. While larger groups can invest in advanced technologies and streamline operations, they may also drive up costs in areas with limited competition. Policymakers must balance the benefits of scale with the need to protect patient access and affordability. Initiatives like antitrust enforcement and transparency laws are critical to addressing these challenges.
In conclusion, the total number of hospital groups in the U.S. reflects a healthcare system in transition, marked by consolidation and centralization. While this trend offers efficiencies, it also poses risks that require careful management. Patients, providers, and policymakers must stay informed about these dynamics to ensure a balanced and equitable healthcare ecosystem.
Does John Peter Smith Hospital Offer Coronary Calcium Scanning?
You may want to see also
Explore related products



$63.58 $79.95



![]()
Largest Hospital Groups by Revenue
The United States healthcare landscape is dominated by a handful of hospital groups that generate billions in revenue annually. Among these, HCA Healthcare stands out as the largest by revenue, reporting over $60 billion in 2022. With nearly 185 hospitals and 2,000 sites of care across 20 states, HCA’s scale allows it to negotiate favorable contracts with insurers and suppliers, a critical advantage in a cost-driven industry. Its focus on operational efficiency and technology integration, such as AI-driven patient flow systems, has further solidified its market leadership.
While HCA leads, CommonSpirit Health and Ascension are close contenders, each generating around $30 billion annually. CommonSpirit’s revenue is bolstered by its extensive network of 142 hospitals and 1,500 care sites, primarily in the western U.S. Ascension, with 139 hospitals, leverages its Catholic-affiliated mission to attract both patients and philanthropic funding. Both groups face challenges, however, including rising labor costs and the need to modernize aging infrastructure, which can erode profit margins if not managed strategically.
A notable trend among the largest hospital groups is their diversification beyond acute care. Kaiser Permanente, with $90 billion in revenue, operates as both a provider and insurer, creating a unique integrated model that reduces administrative waste. This dual role allows Kaiser to align incentives between payers and providers, improving patient outcomes while controlling costs. For smaller hospital groups, emulating this model could be a pathway to sustainability, though it requires significant upfront investment in technology and workforce training.
Revenue alone doesn’t tell the full story; profitability and patient outcomes are equally critical. Tenet Healthcare, with $20 billion in revenue, has struggled with profitability due to high debt levels and underperforming facilities. In contrast, Mayo Clinic, though smaller in revenue at $15 billion, boasts some of the highest patient satisfaction and clinical outcomes in the nation. This highlights the importance of operational excellence over sheer size, a lesson for hospital groups aiming to thrive in a competitive market.
For healthcare stakeholders, understanding these revenue dynamics is essential for strategic planning. Hospital groups with higher revenue often have greater resources for innovation, such as telehealth expansion or precision medicine initiatives. However, smaller groups can compete by focusing on niche services, like rural healthcare or specialized treatments, where larger systems may overlook opportunities. Ultimately, the revenue landscape reflects not just financial health but also the evolving priorities of the U.S. healthcare system.
Hershey's Geisinger Medical: A Comprehensive Hospital
You may want to see also
Explore related products






![]()
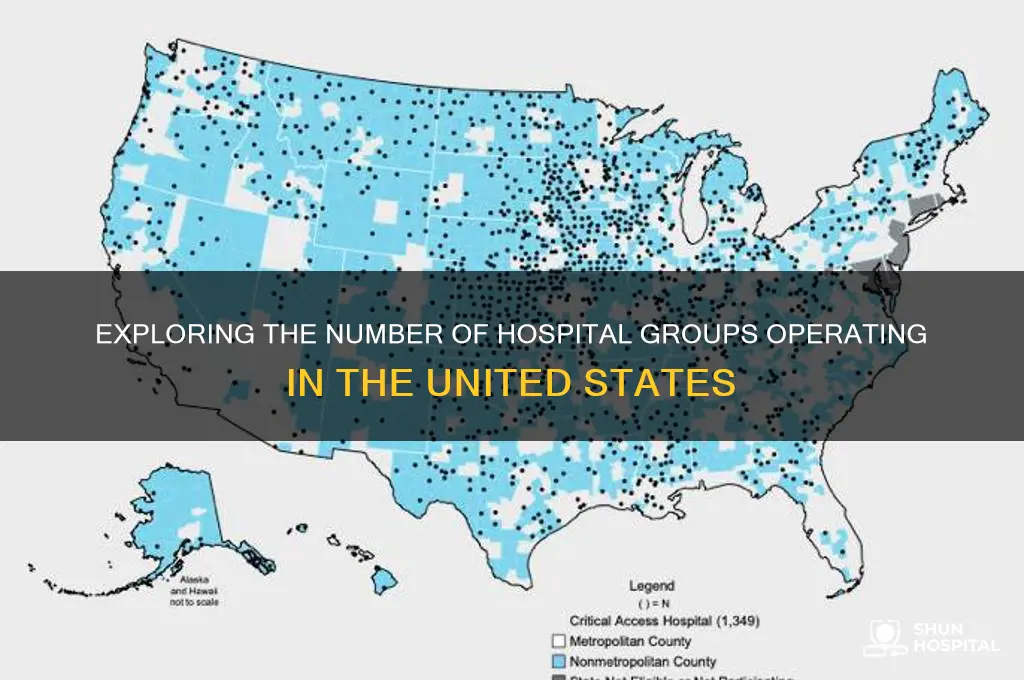
Regional Distribution of Hospital Groups
The United States is home to over 6,000 hospitals, many of which are consolidated into larger hospital groups or systems. These groups vary significantly in size, scope, and regional distribution, reflecting demographic, economic, and healthcare demand disparities across the country. For instance, states like California and Texas host some of the largest hospital groups, such as Kaiser Permanente and HCA Healthcare, due to their dense populations and diverse healthcare needs. In contrast, rural states like Wyoming and Vermont have fewer, smaller hospital groups, often operating as independent or regional systems to serve dispersed populations.
Analyzing the regional distribution reveals a clear urban-rural divide. Urban areas, particularly in the Northeast and Midwest, are dominated by large, multi-state hospital groups that leverage economies of scale and specialized services. For example, New York-Presbyterian Hospital and Cleveland Clinic are flagship institutions in their respective regions, drawing patients from across state lines. In the South and Midwest, hospital groups like Ascension and Baptist Health Systems have expanded through acquisitions, creating extensive networks that cater to both urban and suburban populations. This consolidation often improves access to advanced care but can also reduce competition, impacting costs and patient choice.
Rural regions face unique challenges in hospital group distribution. Many rural hospitals operate independently or as part of small, localized systems due to lower patient volumes and limited funding. However, some larger groups, such as LifePoint Health and Community Health Systems, have strategically expanded into rural areas to fill service gaps. These groups often focus on essential services like emergency care and primary care, with specialized treatments centralized in urban hubs. Despite these efforts, rural hospital closures remain a concern, with over 130 closures since 2010, underscoring the fragility of healthcare infrastructure in these areas.
A comparative analysis of regional distribution highlights the influence of state policies and funding models. States with Medicaid expansion under the Affordable Care Act, such as California and New York, have seen greater investment in hospital group infrastructure, enabling broader service offerings. Conversely, non-expansion states like Texas and Florida often rely on federal programs like Medicare, limiting resources for rural and underserved areas. This disparity is evident in the concentration of hospital groups in expansion states, where systems like Kaiser Permanente and Mayo Clinic thrive, compared to the more fragmented landscape in non-expansion states.
To address regional disparities, policymakers and hospital groups must prioritize targeted strategies. For urban areas, the focus should be on managing consolidation to maintain competition and affordability. In rural regions, incentives for telehealth adoption, workforce development, and partnerships between small hospitals and larger systems can enhance sustainability. Practical steps include leveraging federal grants like the Rural Hospital Closure Grant Program and encouraging state-level initiatives to support rural healthcare infrastructure. By tailoring approaches to regional needs, the U.S. can move toward a more equitable distribution of hospital groups, ensuring access to quality care for all populations.
Santa Fe, NM: Hospitals and Healthcare Options
You may want to see also
Explore related products






![]()
Non-Profit vs. For-Profit Groups
The United States healthcare landscape is dominated by approximately 6,100 hospitals, many of which are consolidated into larger systems or groups. Among these, a critical distinction exists between non-profit and for-profit hospital groups, each operating under different financial models and priorities. Non-profit hospitals, which constitute the majority, reinvest their revenues into patient care, community health programs, and medical research, often qualifying for tax exemptions. For-profit hospitals, on the other hand, prioritize shareholder returns, which can influence their operational decisions and service offerings. This fundamental difference shapes not only their financial structures but also their impact on patient care and community health.
Consider the financial incentives driving these groups. For-profit hospitals often focus on high-margin services, such as elective surgeries or specialty care, which can lead to higher revenues but may limit access to essential services in underserved areas. Non-profit hospitals, while also seeking financial sustainability, are more likely to provide low-margin or unprofitable services, such as emergency care or charity care, due to their mission-driven approach. For instance, non-profit systems like Kaiser Permanente and Mayo Clinic are renowned for their comprehensive care models, whereas for-profit chains like HCA Healthcare are often criticized for prioritizing profitability over accessibility. Understanding these incentives is crucial for patients and policymakers when evaluating healthcare options.
From a community perspective, non-profit hospitals are typically more integrated into the regions they serve. They are required to conduct community health needs assessments and reinvest a portion of their revenues into local programs, such as health education, preventive care, and support for vulnerable populations. For-profit hospitals, while not exempt from community responsibilities, often allocate fewer resources to these initiatives. For example, non-profit systems like Cleveland Clinic and Intermountain Healthcare are celebrated for their community-focused initiatives, whereas for-profit hospitals may face scrutiny for reducing services in low-income areas. This disparity highlights the broader societal impact of each model.
For patients, the choice between a non-profit and for-profit hospital can have tangible implications. Non-profit hospitals often offer more affordable care, particularly for uninsured or underinsured individuals, due to their commitment to charity care and sliding-scale payment options. For-profit hospitals, while competitive in certain services, may charge higher prices to maximize profits. A 2019 study by the RAND Corporation found that prices at for-profit hospitals were 28% higher than at non-profit facilities for similar services. Patients should consider these cost differences, along with factors like service quality and accessibility, when choosing a healthcare provider.
In conclusion, the distinction between non-profit and for-profit hospital groups is not merely semantic but reflects deeper differences in mission, operation, and impact. Non-profit hospitals prioritize community health and accessibility, often at the expense of maximizing revenues, while for-profit hospitals balance patient care with financial returns to shareholders. As the consolidation of hospital groups continues in the U.S., understanding these models is essential for patients, policymakers, and healthcare advocates alike. By recognizing the strengths and limitations of each, stakeholders can make informed decisions that align with their values and needs.
Lucia's Return: Southern Hospitality's Reunion
You may want to see also
Explore related products





![The Hospital [DVD]](https://m.media-amazon.com/images/I/61oQ2sBPcmL._AC_UY218_.jpg)
![]()
Growth Trends in Hospital Consolidation
The number of hospital groups in the U.S. has been steadily declining over the past two decades, a trend driven by the accelerating pace of hospital consolidation. In 2000, there were over 5,000 hospitals operating independently or within small networks. By 2023, this number has shrunk to approximately 3,500 hospitals, with the majority now belonging to larger health systems. This consolidation is reshaping the healthcare landscape, creating both opportunities and challenges for patients, providers, and policymakers.
One of the most significant growth trends in hospital consolidation is the rise of mega-health systems. These entities, often spanning multiple states, are formed through mergers and acquisitions that combine hospitals, clinics, and specialty care centers. For example, CommonSpirit Health, formed by the merger of Dignity Health and Catholic Health Initiatives, operates over 140 hospitals across 21 states. Such consolidations are driven by the need to achieve economies of scale, streamline operations, and negotiate better contracts with insurers. However, critics argue that these mega-systems can reduce competition, leading to higher prices for consumers and limited choices in underserved areas.
Another trend is the increasing involvement of private equity firms in hospital consolidation. Private equity has injected billions of dollars into the healthcare sector, acquiring struggling hospitals and physician practices. While this influx of capital can modernize facilities and improve efficiency, it also raises concerns about profit-driven decision-making at the expense of patient care. A 2022 study found that hospitals acquired by private equity firms experienced a 5% increase in Medicare patient readmission rates, suggesting potential trade-offs between financial performance and clinical outcomes.
Geographically, rural hospitals are disproportionately affected by consolidation trends. As larger health systems focus on urban and suburban markets, many rural hospitals face financial instability and closure. Since 2010, over 130 rural hospitals have shut down, leaving vast regions without access to emergency care. Consolidation can sometimes save these facilities by integrating them into larger networks, but it often comes with the trade-off of reduced local autonomy and changes in service offerings.
To navigate these trends, stakeholders must balance the benefits of consolidation with its potential drawbacks. Policymakers can play a critical role by implementing regulations that promote transparency, protect competition, and ensure access to care in vulnerable communities. Hospitals considering consolidation should conduct thorough due diligence, focusing on cultural alignment and long-term sustainability. Patients, meanwhile, should stay informed about changes in their local healthcare landscape and advocate for policies that prioritize affordability and quality of care. As hospital consolidation continues to evolve, its impact on the U.S. healthcare system will depend on how effectively these challenges are addressed.
Where is Valley Hospital in New Jersey? Location Guide
You may want to see also
Frequently asked questions
As of recent data, there are over 6,000 hospitals in the U.S., but the exact number of hospital groups (or health systems) is around 700 to 800, as many hospitals are part of larger networks or systems.
The largest hospital group in the U.S. is HCA Healthcare (Hospital Corporation of America), which operates over 180 hospitals and approximately 2,000 sites of care across the country.
No, hospital groups (or health systems) are networks of multiple hospitals and healthcare facilities operating under a single organization, while independent hospitals are standalone entities not affiliated with a larger system.







![The Hospital [DVD]](https://m.media-amazon.com/images/I/414R6Z04R6L._AC_UY218_.jpg)


















