The issue of hospital visits resulting from incorrect medication doses is a significant public health concern, highlighting gaps in patient safety and healthcare delivery. Studies indicate that medication errors, particularly those involving improper dosing, account for a substantial number of preventable hospital admissions annually. Factors such as miscommunication between healthcare providers, patient misunderstanding of instructions, and systemic flaws in prescription processes contribute to this problem. Understanding the scope of these hospital visits is crucial for developing targeted interventions, improving medication management protocols, and reducing the burden on healthcare systems while ensuring better patient outcomes.
Explore related products

$61.99 $210

$117.93 $200




What You'll Learn
![]()
Common Medications Causing Hospital Visits
Incorrect medication doses account for a staggering number of hospital visits annually, with certain drugs emerging as repeat offenders. Among these, blood thinners like warfarin top the list. Their narrow therapeutic window—where the difference between a safe dose and a dangerous one is minimal—makes them particularly risky. For instance, a dose of 5 mg might be therapeutic for one patient, while 7.5 mg could lead to life-threatening bleeding in another. Elderly patients, often on multiple medications, are especially vulnerable due to age-related changes in metabolism and kidney function. A missed dose or an accidental double dose can quickly spiral into an emergency, underscoring the need for meticulous monitoring and patient education.
Another culprit is insulin, a lifeline for diabetics but a double-edged sword when mishandled. Hospital admissions related to insulin often stem from dosing errors, such as confusing U-100 and U-40 concentrations or miscalculating carbohydrate ratios. For example, a patient prescribed 10 units of U-100 insulin who mistakenly administers 10 units of U-40 would receive 2.5 times the intended dose, potentially triggering severe hypoglycemia. Pediatric patients are at heightened risk due to their smaller body mass and evolving insulin needs. Clear labeling, proper training, and the use of insulin pens with built-in dose calculators can mitigate these risks, but human error remains a persistent challenge.
Opioid painkillers, such as oxycodone and hydrocodone, also contribute significantly to hospital visits. These medications are often prescribed post-surgery or for chronic pain, but their potent effects and potential for misuse make overdoses common. A typical dose of oxycodone ranges from 5 to 15 mg every 4 to 6 hours, but patients may inadvertently exceed this, especially when combining it with other central nervous system depressants like alcohol or benzodiazepines. The elderly and those with respiratory conditions are particularly susceptible to opioid-induced respiratory depression, a leading cause of emergency admissions. Prescription monitoring programs and patient counseling on safe use are critical interventions to curb these incidents.
Lastly, antidepressants, particularly selective serotonin reuptake inhibitors (SSRIs), frequently lead to hospital visits due to dosing errors or adverse interactions. For example, sertraline (Zoloft) is typically started at 25–50 mg daily, but abrupt increases or concurrent use of other serotonergic drugs can precipitate serotonin syndrome, a potentially fatal condition. Symptoms like agitation, rapid heart rate, and confusion often prompt emergency care. Patients transitioning between medications or those on polypharmacy regimens require careful oversight to avoid such complications. Pharmacists play a pivotal role here, reviewing medication lists and flagging potential risks before they escalate.
Practical steps can reduce hospital visits tied to these medications. For blood thinners, regular INR testing and wearable dose-tracking apps can help patients stay within safe limits. Insulin users should adopt color-coded syringes and attend dosing workshops. Opioid prescriptions should be paired with naloxone kits and clear disposal instructions. Finally, antidepressant users must communicate openly with providers about all medications they’re taking. By targeting these high-risk drugs with tailored strategies, healthcare systems can significantly cut down on preventable admissions.
Mercy Health West Hospital: Distance and Directions from Norwood
You may want to see also
Explore related products






![]()
Age Groups Most Affected by Dosing Errors
Medication errors, particularly those involving incorrect doses, disproportionately affect specific age groups, often leading to hospital visits. Among these, pediatric patients are particularly vulnerable due to their developing physiology and weight-based dosing requirements. For instance, a study published in *Pediatrics* found that children under 5 years old accounted for 20% of medication errors, with common mistakes including administering adult doses or misinterpreting weight-based calculations. A 10-pound infant, for example, requires a dose of acetaminophen that is one-sixth of an adult’s, yet errors in milligram-per-kilogram calculations frequently occur, leading to overdoses or inadequate treatment. Parents and caregivers must use tools like oral syringes instead of spoons and double-check doses with healthcare providers to mitigate risks.
In stark contrast, older adults, particularly those over 65, face a different set of challenges due to age-related changes in metabolism and polypharmacy. The American Journal of Nursing reports that 30% of hospital admissions for adverse drug events in this group stem from dosing errors, often involving anticoagulants like warfarin or diabetes medications like metformin. For example, a 70-year-old patient with reduced renal function may accumulate toxic levels of metformin if dosed at standard levels, leading to lactic acidosis. Clinicians should adhere to guidelines like the Beer’s Criteria, which recommends avoiding or adjusting doses of high-risk medications in older adults, while patients should maintain updated medication lists and undergo regular medication reviews.
Adolescents and young adults represent another at-risk group, often due to self-medication, non-adherence, or miscommunication. A survey by the CDC revealed that 15% of emergency department visits for medication errors in this age group involved over-the-counter pain relievers like ibuprofen, with doses exceeding the 2,400 mg daily limit. This demographic also faces risks with prescription medications, such as ADHD treatments, where incorrect dosing can lead to cardiovascular complications. Education on label reading and clear communication with providers are critical interventions. For example, a teen prescribed 10 mg of Adderall twice daily should be explicitly instructed to avoid doubling doses if a morning dose is missed.
Comparatively, pregnant women and neonates form a unique subset where dosing errors can have intergenerational consequences. A study in *BMJ Open* highlighted that 10% of medication errors in pregnancy involved folic acid or thyroid hormone dosing, which can affect fetal development. Neonates, meanwhile, are susceptible to errors due to their small size and immature organ systems; for instance, a 10-fold overdose of heparin in a neonatal intensive care unit has been reported due to decimal point misinterpretation. Healthcare providers must use standardized dosing protocols and involve pharmacists in medication management for these populations.
In summary, dosing errors disproportionately affect age groups with unique physiological vulnerabilities or complex medication needs. Tailored strategies—such as weight-based dosing in children, renal function monitoring in older adults, education for adolescents, and standardized protocols for pregnant women and neonates—are essential to reducing hospital visits. By addressing these specific risks, healthcare systems can significantly improve patient safety across the lifespan.
Hospital vs. Community Health Center: What's the Difference?
You may want to see also
Explore related products






![]()
Role of Healthcare Providers in Mistakes
Medication errors, particularly those involving incorrect doses, are a significant contributor to hospital visits, with studies indicating that up to 1.3 million people in the U.S. alone are affected annually. Among these, healthcare providers play a dual role: they are both the primary line of defense against such errors and, inadvertently, a potential source of them. The complexity of medication regimens, coupled with high-pressure work environments, creates a fertile ground for mistakes. For instance, a provider might prescribe 500 mg of a medication twice daily instead of 250 mg twice daily, leading to toxicity in a patient with renal impairment. Such errors underscore the need for systemic changes and heightened vigilance within healthcare settings.
One critical area where healthcare providers contribute to dosing mistakes is during the prescribing phase. Electronic health records (EHRs) often lack intuitive interfaces, leading to selection errors, such as choosing the wrong medication strength or frequency. For example, a provider might accidentally select "50 mg/kg" instead of "5 mg/kg" for a pediatric patient, resulting in a tenfold overdose. To mitigate this, providers should adopt a "double-check" system, verifying dosages against standard guidelines like the *Pediatric Dosage Handbook* or using built-in EHR decision support tools. Additionally, clear communication with pharmacists and nurses can act as a secondary safeguard, ensuring that prescribed doses align with patient-specific factors like age, weight, and renal function.
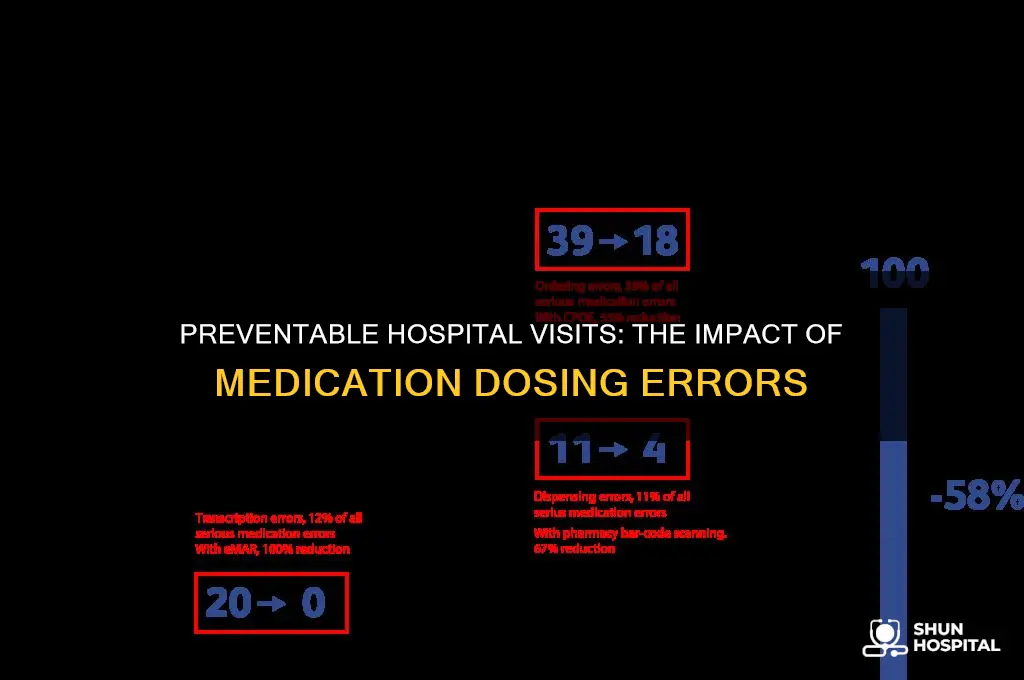
Another significant point of failure occurs during medication administration, where nurses and other caregivers play a pivotal role. Misinterpretation of handwritten prescriptions, confusion between similar-sounding medications, or simple miscalculations can lead to errors. For instance, a nurse might administer 10 mL of a liquid medication instead of 5 mL due to unclear labeling or rushed conditions. Implementing standardized protocols, such as the "five rights" of medication administration (right patient, drug, dose, route, and time), can reduce these risks. Furthermore, barcode scanning systems, which verify medications at the bedside, have been shown to decrease administration errors by up to 80% in some hospitals.
Education and training are equally vital in minimizing provider-related dosing mistakes. Many healthcare professionals receive limited pharmacology training, particularly in pediatrics or geriatrics, where dosing adjustments are critical. For example, a provider might overlook the need to reduce doses in elderly patients with diminished hepatic function, leading to drug accumulation and adverse effects. Continuous education programs, such as workshops on age-specific dosing or webinars on high-alert medications, can bridge these knowledge gaps. Hospitals should also encourage open reporting of near-misses, fostering a culture of learning rather than blame, which can lead to systemic improvements.
Finally, the role of healthcare providers extends to patient education, a frequently overlooked yet essential component of error prevention. Patients and caregivers often misinterpret dosing instructions, such as "take twice daily" as "take every 12 hours," leading to missed doses or overdoses. Providers should use clear, unambiguous language, such as specifying exact times (e.g., "take at 8 AM and 8 PM") and providing written instructions in the patient’s primary language. Visual aids, like dosing calendars or pre-measured medication cups, can further enhance understanding. By empowering patients to take an active role in their medication management, providers can significantly reduce the risk of errors that lead to hospital visits.
In summary, while healthcare providers are integral to patient care, their involvement in medication dosing mistakes is a multifaceted issue requiring targeted interventions. From improving prescribing practices and administration protocols to enhancing education and patient communication, each step can contribute to a safer medication environment. The goal is not to eliminate human error entirely but to create systems resilient enough to catch mistakes before they harm patients.
Strategic Timing for Building Hospitals in CK2: A Comprehensive Guide
You may want to see also
Explore related products






![]()
Impact of Self-Medication on Hospital Admissions
Self-medication, the practice of using medications without professional guidance, significantly contributes to hospital admissions globally. Studies indicate that up to 20% of emergency department visits in some regions are linked to adverse drug events, many stemming from incorrect dosages. For instance, over-the-counter pain relievers like acetaminophen, when taken in excess of the recommended 4,000 mg daily limit, can lead to severe liver damage, necessitating hospitalization. Similarly, misuse of antibiotics, such as taking incomplete courses or incorrect doses, not only fosters antibiotic resistance but also causes gastrointestinal complications requiring medical intervention.
The elderly population is particularly vulnerable to self-medication errors. Age-related changes in metabolism and kidney function mean that standard doses of medications like warfarin or digoxin can easily become toxic. A 2021 study found that 30% of hospital admissions in patients over 65 were due to medication mismanagement, often involving self-adjusted doses of chronic medications. For example, a patient might double their insulin dose to compensate for a missed one, leading to hypoglycemic episodes severe enough to require emergency care.
Children are another high-risk group, as even small deviations in dosage can have profound effects. Liquid medications, such as paracetamol suspensions, often require precise measurements (e.g., 5 mL for a 2-year-old vs. 10 mL for a 5-year-old). Parental errors in measuring doses account for a significant portion of pediatric hospital admissions, with symptoms ranging from mild sedation to life-threatening toxicity. A 2019 report highlighted that 60% of pediatric poisoning cases were due to incorrect administration of common household medications.
To mitigate these risks, practical steps can be taken. Always use calibrated measuring tools for liquid medications instead of household spoons, which can vary widely in size. For the elderly, medication organizers with daily compartments can prevent double-dosing, while regular pharmacist consultations can ensure dosages are adjusted for age and health status. Public health campaigns emphasizing the dangers of self-medication and the importance of adhering to prescribed dosages could also reduce hospital admissions. By addressing these specific vulnerabilities and implementing targeted interventions, the impact of self-medication on healthcare systems can be significantly reduced.
Hospital Seizure Management: Essential Steps for Patient Care and Safety
You may want to see also
Explore related products






![]()
Preventive Measures to Reduce Dosing Errors
Medication errors, particularly those involving incorrect doses, account for a staggering number of hospital visits annually. Studies indicate that dosing errors contribute to over 700,000 emergency department visits in the U.S. alone, with children under five and adults over 65 being the most vulnerable. These errors often stem from miscommunication, misinterpretation of prescriptions, or simple oversight. To combat this, implementing preventive measures is not just beneficial—it’s critical.
One of the most effective strategies is standardizing medication labels and prescriptions. Ambiguous abbreviations, such as "qd" (daily) or "qod" (every other day), can lead to confusion. Replacing these with clear, unambiguous language—for example, writing "once daily" instead of "qd"—reduces the risk of misinterpretation. Additionally, using bold or highlighted text for critical information, like dosage values (e.g., "5 mg, not 50 mg"), can serve as a visual cue for both healthcare providers and patients.
Another key preventive measure is leveraging technology. Electronic prescribing systems (e-prescribing) can automatically flag potential dosing errors based on patient age, weight, and medical history. For instance, a system might alert a physician if a prescribed dose of acetaminophen exceeds the recommended 75 mg/kg/day for a child. Similarly, barcode scanning systems in hospitals ensure that the right patient receives the right medication at the right dose, minimizing human error during administration.
Patient education plays a pivotal role in preventing dosing errors. Pharmacists should provide clear, verbal instructions alongside written labels, especially for medications with complex dosing regimens, such as warfarin or insulin. For example, explaining that "take 1 tablet twice daily" means one tablet in the morning and one in the evening can prevent double-dosing. Including visual aids, like diagrams or calendars, can further enhance understanding, particularly for elderly patients or those with limited literacy.
Finally, healthcare institutions must foster a culture of double-checking and accountability. Implementing the "independent double-check" system, where two nurses verify medication doses before administration, has proven effective in high-risk settings like intensive care units. Similarly, encouraging patients or caregivers to ask questions—such as "Is this the correct dose for my child?"—empowers them to act as a final safeguard. By combining technological tools, clear communication, and proactive education, dosing errors can be significantly reduced, ultimately saving lives and reducing hospital visits.
Exploring Ashika Island: Where's the Hospital?
You may want to see also
Frequently asked questions
Estimates vary, but studies suggest that incorrect medication doses account for approximately 1.3 million emergency department visits annually in the United States alone.
Medication errors, including dosing mistakes, contribute to about 5-10% of all hospital admissions, with dosing errors being a significant subset of these cases.
Children under 5 and adults over 65 are the most vulnerable to hospital visits caused by incorrect medication doses, due to factors like weight-based dosing challenges and polypharmacy.