The closure of rural hospitals has become a pressing issue across the United States, and North Carolina has not been immune to this trend. Over the past decade, numerous rural hospitals in the state have shut their doors, leaving communities with limited access to essential healthcare services. Factors such as declining populations, financial strain, and the challenges of maintaining outdated infrastructure have contributed to these closures. Understanding the scope and impact of these shutdowns is crucial, as they not only affect patient care but also have broader economic and social implications for rural areas in North Carolina.
| Characteristics | Values |
|---|---|
| Total Rural Hospital Closures (NC) | 18 (since 2005) |
| Recent Closures (2020-2023) | 4 |
| Primary Reasons for Closures | Financial distress, declining reimbursements, workforce shortages |
| Impacted Counties | Primarily in eastern and western NC (e.g., Bertie, Montgomery) |
| Population Affected | Over 100,000 rural residents |
| State Response | NC Rural Health Initiative, funding for rural hospitals |
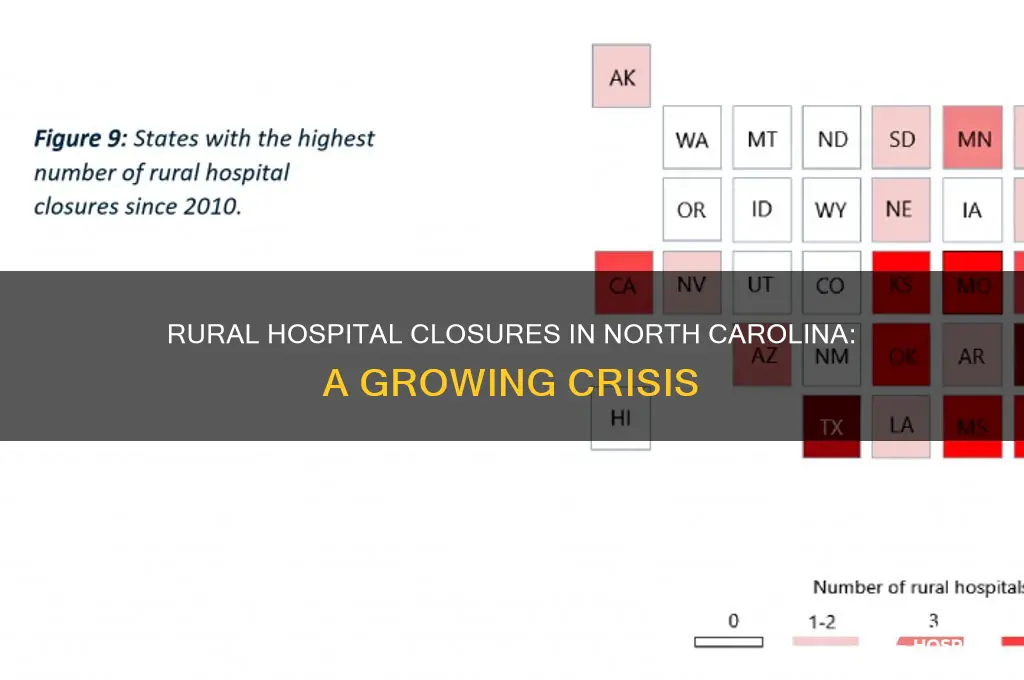
| National Context | NC ranks among top states with rural hospital closures |
| Latest Closure (as of 2023) | Washington County Hospital (closed in 2023) |
| Ongoing Challenges | Limited access to healthcare, increased travel distances for patients |
Explore related products






What You'll Learn
- Closure Trends Over Time: Annual shutdown rates of rural hospitals in North Carolina from 2000 to 2023
- Causes of Closures: Financial struggles, low patient volumes, and lack of state funding contributing to shutdowns
- Impact on Communities: Loss of healthcare access, increased travel times, and economic decline in rural areas
- Regional Distribution: Counties most affected by hospital closures in North Carolina’s rural regions
- Policy Responses: State and federal initiatives to prevent further closures and support rural healthcare
![]()
Closure Trends Over Time: Annual shutdown rates of rural hospitals in North Carolina from 2000 to 2023
Between 2000 and 2023, North Carolina witnessed a steady but accelerating closure of rural hospitals, with annual shutdown rates reflecting broader national trends in healthcare economics and policy shifts. Data reveals that the state lost an average of 1.2 rural hospitals per year during this period, though the rate was not uniform. The early 2000s saw sporadic closures, often tied to financial insolvency or lack of modernization. However, the post-2010 era marked a sharp increase, coinciding with the implementation of the Affordable Care Act (ACA) and subsequent changes in reimbursement models. By 2020, the annual closure rate had nearly doubled, with five rural hospitals shutting down in a single year, underscoring the deepening crisis in rural healthcare access.
Analyzing the data, several factors emerge as drivers of this trend. First, declining populations in rural areas reduced patient volumes, making it harder for hospitals to sustain operations. Second, the shift from fee-for-service to value-based care models disproportionately impacted rural hospitals, which often lacked the infrastructure to adapt. Third, the state’s decision not to expand Medicaid until 2023 left many rural hospitals without critical funding, as uninsured patients accounted for a significant portion of their uncompensated care. These closures were not merely numbers; they represented the loss of emergency services, maternity care, and primary care for thousands of residents, exacerbating health disparities in already underserved communities.
A comparative analysis with neighboring states highlights North Carolina’s unique challenges. While states like Virginia and Tennessee experienced similar closure trends, North Carolina’s slower adoption of Medicaid expansion amplified its struggles. For instance, rural hospitals in states with expanded Medicaid saw a 50% reduction in uncompensated care costs, a benefit North Carolina’s hospitals missed for over a decade. This delay not only accelerated closures but also hindered efforts to transition to alternative care models, such as rural health clinics or telemedicine, which require upfront investment.
To address this crisis, policymakers and healthcare leaders must take targeted steps. First, prioritize Medicaid expansion’s full implementation to stabilize hospital finances. Second, incentivize public-private partnerships to fund infrastructure upgrades and technology adoption in rural hospitals. Third, establish grant programs for transitioning hospitals into community health hubs, offering a mix of urgent care, mental health services, and preventive care. Finally, leverage telemedicine to bridge gaps in access, ensuring rural residents can connect with specialists without traveling long distances. Without such interventions, the closure trend will persist, leaving rural North Carolinians increasingly isolated from essential healthcare services.
Incident Reports: Saving Lives in Hospitals
You may want to see also
Explore related products




![The Hospital [DVD]](https://m.media-amazon.com/images/I/61oQ2sBPcmL._AC_UY218_.jpg)

![]()
Causes of Closures: Financial struggles, low patient volumes, and lack of state funding contributing to shutdowns
Rural hospitals in North Carolina are facing a crisis, with financial struggles at the forefront of their challenges. Since 2010, at least 15 rural hospitals in the state have closed their doors, leaving communities without critical healthcare access. These closures are not isolated incidents but part of a broader trend exacerbated by economic pressures. Operating costs for rural hospitals have skyrocketed, driven by rising expenses for medical supplies, technology, and staffing. Meanwhile, reimbursement rates from Medicare and Medicaid often fall short of covering these costs, creating a financial gap that many facilities cannot bridge. For instance, a 2021 report by the North Carolina Rural Health Association highlighted that rural hospitals in the state operate on razor-thin margins, with some losing millions annually. Without a sustainable financial model, these hospitals are forced to shut down, leaving residents with limited or no access to emergency care.
Low patient volumes further compound the financial woes of rural hospitals. Unlike urban hospitals, which benefit from dense populations and higher patient traffic, rural facilities often serve sparsely populated areas. This demographic reality means fewer patients seeking routine care, elective procedures, or emergency services. As a result, hospitals struggle to generate sufficient revenue to maintain operations. For example, a hospital in eastern North Carolina reported an average of only 10 emergency room visits per day, far below the threshold needed to sustain its services. When patient volumes are this low, even small fluctuations in demand can have devastating financial consequences. This vicious cycle of low revenue and high costs leaves hospitals with no choice but to close, further isolating rural communities from essential healthcare services.
The lack of state funding plays a critical role in the closure of rural hospitals, exacerbating their financial and operational challenges. While some states have implemented programs to support rural healthcare, North Carolina’s funding mechanisms have been criticized for being inadequate. For instance, the state’s Medicaid expansion, which could have provided a financial lifeline to struggling hospitals, was only implemented in 2023, years after other states took similar steps. Additionally, rural hospitals often miss out on grants and subsidies due to complex application processes or eligibility criteria that favor larger, urban institutions. Without targeted financial support, these hospitals are left to fend for themselves in an increasingly hostile economic environment. A 2022 study found that rural hospitals in states with robust funding programs were 50% less likely to close, underscoring the impact of state-level intervention.
Addressing the closure of rural hospitals in North Carolina requires a multi-faceted approach that tackles financial struggles, low patient volumes, and inadequate state funding. Policymakers must prioritize increasing Medicaid reimbursement rates and simplifying access to grants for rural hospitals. Additionally, innovative solutions like telemedicine and mobile clinics can help bridge the gap in patient volumes by expanding access to care in underserved areas. For communities, advocating for local hospitals and supporting legislative efforts to bolster rural healthcare funding can make a tangible difference. The closure of even one rural hospital can have devastating consequences, from increased travel times for emergencies to higher mortality rates. By understanding and addressing these root causes, North Carolina can work toward preserving its rural healthcare infrastructure and ensuring that all residents have access to the care they need.
Radiation Oncology: Hospital-Based Specialty Explained
You may want to see also
Explore related products



![The Hospital [DVD]](https://m.media-amazon.com/images/I/414R6Z04R6L._AC_UY218_.jpg)
![]()
Impact on Communities: Loss of healthcare access, increased travel times, and economic decline in rural areas
The closure of rural hospitals in North Carolina has left gaping holes in the healthcare safety net, particularly for the state's most vulnerable populations. Since 2010, at least 10 rural hospitals have shuttered their doors, leaving behind communities struggling to access essential medical services. This trend is not unique to North Carolina, but the state's experience highlights the devastating consequences of hospital closures on rural residents.
Consider the case of a 65-year-old diabetic patient in a rural North Carolina county. With the nearest hospital now 45 minutes away, managing her condition becomes a logistical nightmare. Regular check-ups, insulin adjustments, and emergency care are no longer convenient or timely. This scenario is not hypothetical; it's the reality for thousands of rural North Carolinians. The loss of local healthcare access disproportionately affects the elderly, low-income families, and those with chronic conditions, who often rely on public transportation or family members for travel.
Increased travel times to healthcare facilities exacerbate existing health disparities. A study by the North Carolina Rural Health Research Program found that rural residents face, on average, a 30% longer travel time to the nearest hospital compared to urban dwellers. This delay can be critical in emergency situations, such as heart attacks or strokes, where every minute counts. For instance, the 'golden hour' – the critical time period for treating trauma patients – becomes a luxury for those living in areas with limited healthcare access. As a result, rural residents are more likely to experience adverse health outcomes, including higher mortality rates.
The economic repercussions of hospital closures ripple through rural communities, further exacerbating the healthcare crisis. Hospitals are often the largest employers in rural areas, providing stable jobs and contributing significantly to the local tax base. When a hospital closes, the loss of jobs and revenue can lead to a downward economic spiral. Local businesses suffer as healthcare workers relocate, and the community's ability to attract new investments diminishes. This economic decline creates a vicious cycle, making it even more challenging to restore healthcare services or attract alternative industries.
To mitigate these impacts, communities must explore innovative solutions. Telemedicine, for instance, can bridge the gap in healthcare access by providing remote consultations and monitoring. However, this requires robust broadband infrastructure, which is often lacking in rural areas. Mobile health clinics and community health worker programs can also play a vital role in delivering primary care and health education. Policy interventions, such as financial incentives for healthcare providers serving rural areas and investments in rural healthcare infrastructure, are essential to stem the tide of hospital closures and ensure that rural communities have access to the care they need.
Bronx Lebanon Hospital's Health and Wellness Gyn Services for Infertility Treatment
You may want to see also
![]()
Regional Distribution: Counties most affected by hospital closures in North Carolina’s rural regions
North Carolina’s rural hospital closures are not evenly distributed; certain counties bear a disproportionate burden. Since 2010, 14 rural hospitals have closed in the state, with clusters in the northeastern and western regions. Counties like Bertie, Northampton, and Graham exemplify this trend, where closures have left residents with limited access to emergency care. These areas often share common challenges: high poverty rates, aging populations, and a reliance on Medicaid or uninsured patients, which strain hospital finances. Understanding this regional concentration is critical for targeted interventions.
Consider Bertie County, where the closure of Bertie Memorial Hospital in 2017 left 20,000 residents without a local emergency department. The nearest hospital is now 30 miles away, a distance that can be life-threatening in emergencies. Similarly, in Graham County, the closure of Mission Hospital’s rural outpost forced residents to travel to Asheville, a 70-mile journey through mountainous terrain. These examples illustrate how closures in specific counties exacerbate health disparities, particularly for vulnerable populations like the elderly and low-income families. Policymakers must prioritize these regions when allocating resources to prevent further closures.
To address this crisis, a multi-pronged approach is necessary. First, increase Medicaid reimbursement rates to rural hospitals, as North Carolina’s rates are among the lowest nationally. Second, expand telehealth services in affected counties, though this requires broadband infrastructure improvements. Third, incentivize healthcare providers to practice in these areas through loan forgiveness programs or tax incentives. For instance, the North Carolina Rural Health Leadership Program has shown promise in retaining rural clinicians. Finally, community health workers can bridge gaps by providing preventive care and health education in underserved counties.
Comparatively, counties with successful rural hospital models, like Cherokee County, offer lessons. Cherokee’s hospital thrives due to partnerships with larger health systems and innovative revenue streams, such as urgent care services. Replicating such strategies in hard-hit counties could mitigate closures. However, caution is needed: one-size-fits-all solutions often fail in rural settings. Each county’s unique demographics, economic conditions, and healthcare needs must inform tailored interventions. For example, a county with a large elderly population may require more geriatric services, while another with high maternal mortality needs obstetrics support.
In conclusion, the regional distribution of hospital closures in North Carolina’s rural counties demands targeted, data-driven solutions. By focusing on the most affected areas and learning from successful models, stakeholders can reverse this trend. Practical steps include policy reforms, technological investments, and community-based initiatives. Without urgent action, the health and economic well-being of these counties will continue to deteriorate, widening the urban-rural divide in healthcare access.
Why Hospitals Struggle to Learn from Mistakes and Improve
You may want to see also
![]()
Policy Responses: State and federal initiatives to prevent further closures and support rural healthcare
North Carolina has seen a troubling rise in rural hospital closures, with over 15 facilities shuttering since 2010. This trend threatens access to care for hundreds of thousands of residents, exacerbating health disparities in already underserved communities. To combat this crisis, state and federal policymakers have launched targeted initiatives aimed at stabilizing rural healthcare systems. These efforts range from financial incentives to innovative care delivery models, each designed to address the unique challenges faced by rural hospitals.
One key federal initiative is the Rural Hospital Closure Relief Act, which provides direct financial assistance to hospitals at risk of closure. This act allocates funds based on factors like patient volume, operating margins, and community need. For example, eligible hospitals can receive up to $12 million in grants over three years, provided they demonstrate a commitment to improving financial sustainability through cost-cutting measures or revenue diversification. Additionally, the act expands Medicare reimbursement rates for rural hospitals, ensuring they receive fair compensation for the critical services they provide.
At the state level, North Carolina has implemented the Rural Health Care Access Program (RHCAP), a multifaceted approach to supporting rural hospitals. RHCAP offers low-interest loans to hospitals for infrastructure upgrades, such as modernizing outdated equipment or expanding telehealth capabilities. The program also funds workforce development initiatives, including scholarships for nursing students who commit to working in rural areas. By addressing both financial and staffing challenges, RHCAP aims to create a more resilient rural healthcare system.
Another innovative policy response is the adoption of the Rural Emergency Hospital (REH) model, which allows struggling hospitals to downsize and refocus on emergency and outpatient services. This model reduces operational costs while maintaining essential care access. Hospitals converting to REHs receive enhanced Medicare reimbursements and technical assistance to navigate the transition. For instance, a hospital in eastern North Carolina successfully converted to an REH in 2022, stabilizing its finances and ensuring continued access to emergency care for over 10,000 residents.
Despite these initiatives, challenges remain. Policymakers must ensure that funding reaches the most vulnerable hospitals and that programs are flexible enough to meet diverse community needs. For example, rural hospitals in areas with high poverty rates may require additional support for patient transportation or chronic disease management programs. Moreover, long-term sustainability depends on addressing systemic issues like workforce shortages and declining populations. By combining targeted financial assistance with innovative care models, state and federal policies can help stem the tide of rural hospital closures and safeguard healthcare access for North Carolina’s rural communities.
Pneumonia in Children: When Hospitalization is Necessary
You may want to see also
Frequently asked questions
As of recent data, North Carolina has seen the closure of at least 10 rural hospitals since 2010, with the trend continuing due to financial pressures and healthcare challenges.
Rural hospital closures in North Carolina are primarily attributed to financial strain, declining patient volumes, lack of reimbursement from Medicaid and Medicare, and the inability to sustain operations in underserved areas.
Counties such as Bertie, Franklin, and Montgomery have been significantly impacted by rural hospital closures, leaving residents with limited access to healthcare services.
North Carolina has implemented initiatives like the Rural Hospital Stabilization Fund and partnerships with healthcare organizations to provide financial support, improve telehealth services, and address workforce shortages in rural areas.