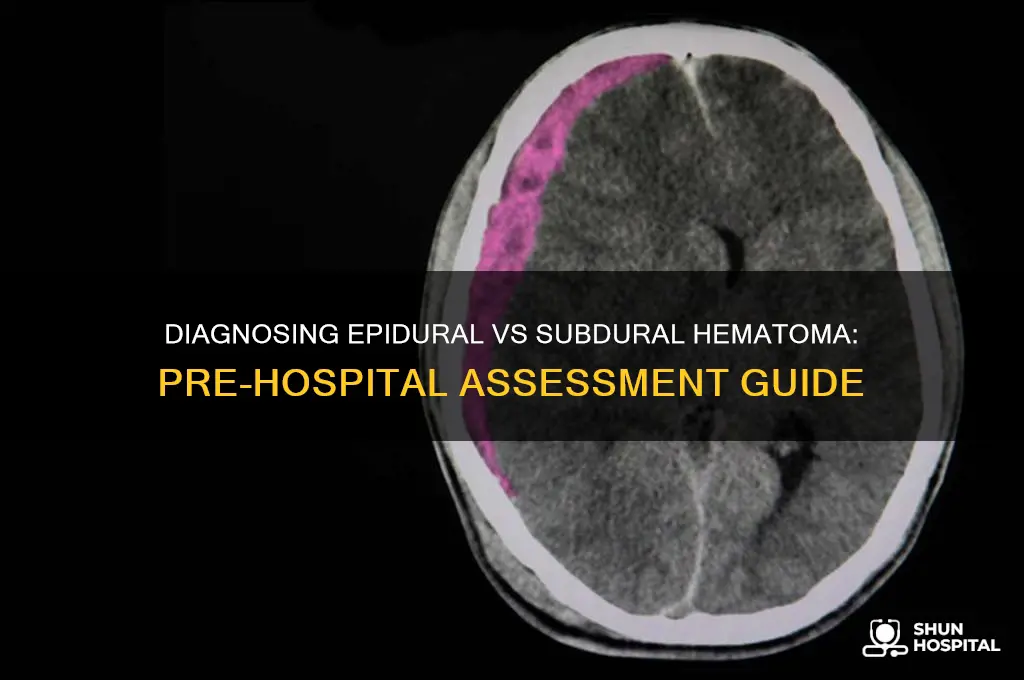
Diagnosing epidural versus subdural hematoma in the pre-hospital setting is a critical yet challenging task for emergency medical providers. Both conditions involve bleeding around the brain but differ in location, mechanism, and clinical presentation. Epidural hematomas typically result from arterial bleeding, often following a skull fracture, and are characterized by a rapid onset of symptoms, including severe headache, altered mental status, and potential neurological deficits. In contrast, subdural hematomas usually stem from venous bleeding, are more common in the elderly or those on anticoagulants, and may present with a slower progression of symptoms, such as confusion, lethargy, or focal neurological signs. Pre-hospital providers must rely on a combination of patient history, mechanism of injury, and clinical signs, such as pupillary changes or focal weakness, to differentiate between the two. While definitive diagnosis requires imaging, early recognition and appropriate triage are essential to ensure timely intervention and improve patient outcomes.
Explore related products






What You'll Learn
- Patient History: Focus on trauma mechanism, anticoagulant use, and symptom onset timing
- Neurological Signs: Assess for focal deficits, altered mental status, and pupillary changes
- Imaging Limitations: Recognize pre-hospital imaging constraints and rely on clinical judgment
- Symptom Differentiation: Epidural: rapid deterioration; Subdural: gradual symptoms, often in elderly
- Glasgow Coma Scale: Use GCS to evaluate consciousness level and track changes over time
![]()
Patient History: Focus on trauma mechanism, anticoagulant use, and symptom onset timing
Trauma mechanism is the cornerstone of differentiating between epidural and subdural hematomas in the pre-hospital setting. Epidural hematomas typically result from high-impact injuries, such as motor vehicle collisions or falls from significant heights, where the force causes the skull to fracture and the middle meningeal artery to rupture. In contrast, subdural hematomas often arise from lower-energy trauma, like minor falls in elderly patients, due to bridging vein tears in the context of brain atrophy. Understanding the nature and severity of the injury helps narrow the diagnostic possibilities early on.
Anticoagulant use is another critical factor in patient history that can influence the likelihood and severity of either hematoma. Patients on warfarin, direct oral anticoagulants (DOACs), or antiplatelet agents like aspirin are at increased risk of bleeding complications, even from seemingly minor trauma. For instance, a patient on warfarin with an INR > 2.0 who experiences a ground-level fall may develop a rapidly expanding subdural hematoma due to impaired clotting mechanisms. Pre-hospital providers should inquire about medication use, including dosages and last administration time, to assess bleeding risk and guide urgency of transport.
Symptom onset timing provides vital clues to the type and progression of the hematoma. Epidural hematomas often present with a classic "lucid interval," where the patient is initially asymptomatic or mildly symptomatic after trauma, followed by rapid deterioration within minutes to hours due to arterial bleeding. Subdural hematomas, however, typically manifest with a more gradual onset of symptoms, such as headache, confusion, or focal neurological deficits, over hours to days, reflecting the slower venous bleeding. Documenting the time from injury to symptom onset helps differentiate between these two conditions and informs the need for immediate intervention.
In practice, combining these historical elements—trauma mechanism, anticoagulant use, and symptom onset timing—creates a robust framework for pre-hospital diagnosis. For example, a young adult involved in a high-speed motorcycle accident without helmet use, who becomes unconscious at the scene, is highly suspicious for an epidural hematoma. Conversely, an 80-year-old on apixaban (5 mg twice daily) who fell from a standing position and developed confusion 12 hours later is more likely to have a subdural hematoma. Tailoring the history-taking process to these specifics ensures a focused and efficient assessment, enabling timely decision-making in critical situations.
Why Do Hospital Gowns Have Open Backs?
You may want to see also
Explore related products






![]()
Neurological Signs: Assess for focal deficits, altered mental status, and pupillary changes
Focal neurological deficits—weakness, numbness, or paralysis in specific body parts—can be early indicators of either epidural or subdural hematoma, but their presentation differs. In epidural hematomas, which often result from arterial bleeding, deficits typically appear suddenly and progress rapidly due to the high-pressure expansion of the hematoma. For instance, a patient might present with unilateral leg weakness or arm droop within minutes to hours of a head injury. Subdural hematomas, on the other hand, usually involve venous bleeding and progress more slowly, with deficits appearing over hours to days. A patient might initially complain of mild clumsiness in one hand, which gradually worsens. Always document the onset, location, and progression of these deficits, as they provide critical clues to the type and urgency of the hematoma.
Altered mental status is another hallmark of both epidural and subdural hematomas but manifests differently. Epidural hematomas often cause a classic "lucid interval"—a brief period of normal consciousness after the injury, followed by rapid deterioration into confusion, lethargy, or coma. This occurs because the hematoma compresses the brain, leading to increased intracranial pressure (ICP). In contrast, subdural hematomas typically present with more gradual changes in mental status, such as increasing confusion, disorientation, or somnolence. Use the AVPU scale (Alert, Voice, Pain, Unresponsive) or the Glasgow Coma Scale (GCS) to objectively assess mental status. A GCS score below 15 warrants immediate suspicion of a significant hematoma and requires urgent intervention.
Pupillary changes are among the most critical neurological signs to assess pre-hospital, as they directly reflect increased ICP. In epidural hematomas, unilateral or bilateral fixed, dilated pupils often indicate severe brainstem compression and are a late but ominous sign. Subdural hematomas may also cause pupillary abnormalities, but these are typically less pronounced and more gradual. Always use a penlight to evaluate pupil size, symmetry, and reactivity to light. Unequal pupils (anisocoria) or sluggish reactivity strongly suggest a mass effect from the hematoma. If pupillary changes are present, prepare for rapid transport and notify the receiving facility to ensure immediate neurosurgical evaluation.
In practice, combine these neurological assessments systematically. Start with a rapid mental status check using the AVPU or GCS, then evaluate for focal deficits by testing grip strength, limb movement, and sensation. Finally, examine the pupils. For example, a patient with a GCS of 12, right-sided arm weakness, and sluggishly reactive pupils likely has a subdural hematoma, whereas a patient with a GCS of 8, left leg paralysis, and a fixed, dilated right pupil likely has an epidural hematoma. These findings should guide your pre-hospital management, including immobilization, oxygenation, and rapid transport to a trauma center. Remember, early recognition of these neurological signs can be lifesaving, as both conditions require prompt surgical intervention to prevent irreversible brain damage.
Henderson, Nevada: Hospital Performance Review
You may want to see also
Explore related products




$18.34 $20


![]()
Imaging Limitations: Recognize pre-hospital imaging constraints and rely on clinical judgment
In the pre-hospital setting, the absence of advanced imaging modalities like CT scans forces clinicians to rely heavily on clinical judgment. This reliance is not a limitation but a necessity, as time is critical in managing traumatic brain injuries. For instance, a patient with a Glasgow Coma Scale (GCS) score of 8 or below, coupled with signs of increased intracranial pressure (e.g., Cushing’s triad: hypertension, bradycardia, abnormal breathing), should prompt immediate suspicion of a hematoma, regardless of imaging availability. The key takeaway is that clinical acumen must guide decision-making, as imaging is not an option in this phase of care.
Consider the practical constraints of pre-hospital imaging: portable ultrasound, while useful for focused assessments like eFAST, lacks the resolution to differentiate between epidural and subdural hematomas. Even if a portable CT scanner were available, the logistics of setup, radiation safety, and interpretation time would render it impractical in most emergency scenarios. For example, a paramedic team responding to a high-speed motor vehicle collision cannot afford the 15–20 minutes required for CT imaging when every minute counts in stabilizing the patient. Thus, clinicians must prioritize rapid assessment and intervention over diagnostic perfection.
A comparative analysis of epidural and subdural hematomas highlights why clinical judgment is paramount. Epidural hematomas, often lens-shaped on imaging, typically result from temporal bone fractures and arterial bleeding, leading to rapid deterioration. Subdural hematomas, conversely, are more common in venous bleeding, often crescent-shaped, and may present with a slower progression. However, without imaging, the clinician must focus on history (e.g., mechanism of injury, anticoagulant use) and physical exam findings (e.g., battle’s sign, rapid neurological decline) to differentiate between the two. For instance, a 70-year-old on warfarin with a GCS of 12 after a fall is more likely to have a subdural hematoma, whereas a 25-year-old with a GCS of 6 post-motorcycle accident is at higher risk for an epidural hematoma.
Finally, a persuasive argument for clinical reliance is the potential harm of delaying treatment. Waiting for confirmatory imaging in the pre-hospital phase can lead to irreversible brain damage or death. Instead, clinicians should focus on ABCs (airway, breathing, circulation), administer analgesia and antiemetics as needed, and prepare for rapid transport to a definitive care facility. For example, a patient with a suspected epidural hematoma should be intubated early to prevent hypoxia and hypercarbia, which exacerbate intracranial hypertension. The ultimate conclusion is clear: in the absence of imaging, clinical judgment is not just a fallback—it is the cornerstone of effective pre-hospital management.
Revenue-Generating Hospital Departments: Key Areas of Support and Impact
You may want to see also
Explore related products






![]()
Symptom Differentiation: Epidural: rapid deterioration; Subdural: gradual symptoms, often in elderly
In the critical moments before hospital arrival, distinguishing between epidural and subdural hematomas hinges on recognizing the pace of symptom onset. Epidural hematomas, often linked to arterial bleeding, manifest with alarming speed. Patients may appear stable initially but rapidly deteriorate within minutes to hours, presenting with severe headaches, altered consciousness, and focal neurological deficits. This abrupt decline is a red flag for first responders, signaling the need for immediate intervention to prevent herniation.
Contrastingly, subdural hematomas, typically venous in origin, unfold gradually, often over days or weeks. Elderly patients, particularly those on anticoagulants or with a history of falls, are at higher risk. Symptoms such as mild headaches, confusion, and subtle motor weakness may go unnoticed initially, only to worsen slowly as the hematoma expands. This insidious progression demands a high index of suspicion, especially in the absence of a clear traumatic event.
For pre-hospital providers, the temporal pattern of symptoms is a diagnostic cornerstone. Epidural hematomas require urgent imaging and surgical decompression, whereas subdural hematomas may allow for a more measured approach, though both necessitate rapid transport to a trauma center. Observing whether the patient’s condition worsens within minutes (epidural) or over days (subdural) can guide initial management and triage decisions.
Practical tips include assessing for risk factors like anticoagulant use or recent head trauma and correlating the patient’s history with their neurological exam. For instance, an elderly patient with a minor fall and gradual confusion is more likely to have a subdural hematoma, while a young adult with a severe headache and rapid unconsciousness post-trauma suggests an epidural hematoma. Recognizing these distinctions ensures timely and appropriate care, potentially saving lives.
Hospital Visitation Rights: Who Can Be With You?
You may want to see also
Explore related products




![]()
Glasgow Coma Scale: Use GCS to evaluate consciousness level and track changes over time
The Glasgow Coma Scale (GCS) is a critical tool in pre-hospital settings for assessing the level of consciousness in patients with suspected head injuries, including epidural and subdural hematomas. This 15-point scale evaluates three key areas: eye-opening response, verbal response, and motor response. By systematically scoring these components, first responders can quickly gauge the severity of a patient’s condition and monitor changes over time, which is vital for differentiating between epidural and subdural hematomas. For instance, a patient with an epidural hematoma may present with a rapidly declining GCS score due to the acute nature of the bleed, whereas a subdural hematoma might show a more gradual deterioration.
To effectively use the GCS, follow these steps: first, assess eye-opening response (4 points for spontaneous, 3 for to voice, 2 for to pain, and 1 for none). Second, evaluate verbal response (5 points for oriented, 4 for confused, 3 for inappropriate words, 2 for incomprehensible sounds, and 1 for none). Finally, test motor response (6 points for obeying commands, 5 for localizing pain, 4 for withdrawing from pain, 3 for abnormal flexion, 2 for extension to pain, and 1 for no response). Summing these scores provides a total GCS score ranging from 3 (worst) to 15 (best). Document the initial score and reassess every 15–30 minutes to track changes, as a declining GCS score in a head injury patient strongly suggests an evolving hematoma.
While the GCS is invaluable, it has limitations. For example, intubated patients cannot be scored for verbal response, and certain medications or pre-existing conditions (e.g., stroke) may skew results. Additionally, children under 2 years old require a modified version of the scale, as their responses differ from adults. Despite these caveats, the GCS remains a gold standard in pre-hospital care for its simplicity and reliability in assessing consciousness.
In the context of differentiating epidural vs. subdural hematomas, the GCS trend is particularly telling. Epidural hematomas often present with a classic "lucid interval"—a period of normal consciousness followed by rapid deterioration—whereas subdural hematomas typically show a more gradual decline. For instance, a patient with a GCS score dropping from 15 to 8 within an hour is more likely to have an epidural hematoma, while a score decreasing from 14 to 10 over several hours suggests a subdural hematoma. Recognizing these patterns can guide immediate interventions, such as rapid transport to a trauma center for surgical decompression.
Practical tips for using the GCS in the field include ensuring a quiet environment to accurately assess verbal responses, using firm but gentle stimuli to test motor responses, and avoiding repeated painful stimuli that could agitate the patient. Always document the GCS score clearly in your report, noting the time of assessment and any changes observed. By mastering the GCS and understanding its implications in hematoma diagnosis, pre-hospital providers can significantly improve patient outcomes through timely and targeted care.
Distance Guide: Allen Hospital to Jacobi Medical Center Travel Time
You may want to see also
Frequently asked questions
Epidural hematomas often present with a brief period of consciousness ("lucid interval") after trauma, followed by rapid deterioration, severe headache, and focal neurological deficits. Subdural hematomas typically show gradual onset of symptoms, such as confusion, lethargy, and progressive neurological decline, especially in older adults or those with chronic bleeding.
Epidural hematomas often cause unilateral pupil dilation (blown pupil) due to pressure on the brainstem, while subdural hematomas may cause bilateral pupil changes or no pupillary abnormalities, depending on the extent of brain compression.
Epidural hematomas are commonly associated with high-impact trauma, such as falls from height or motor vehicle accidents, often involving skull fractures. Subdural hematomas are more frequently seen in lower-energy trauma, especially in elderly patients or those on anticoagulants, and may occur without a significant fracture.



















