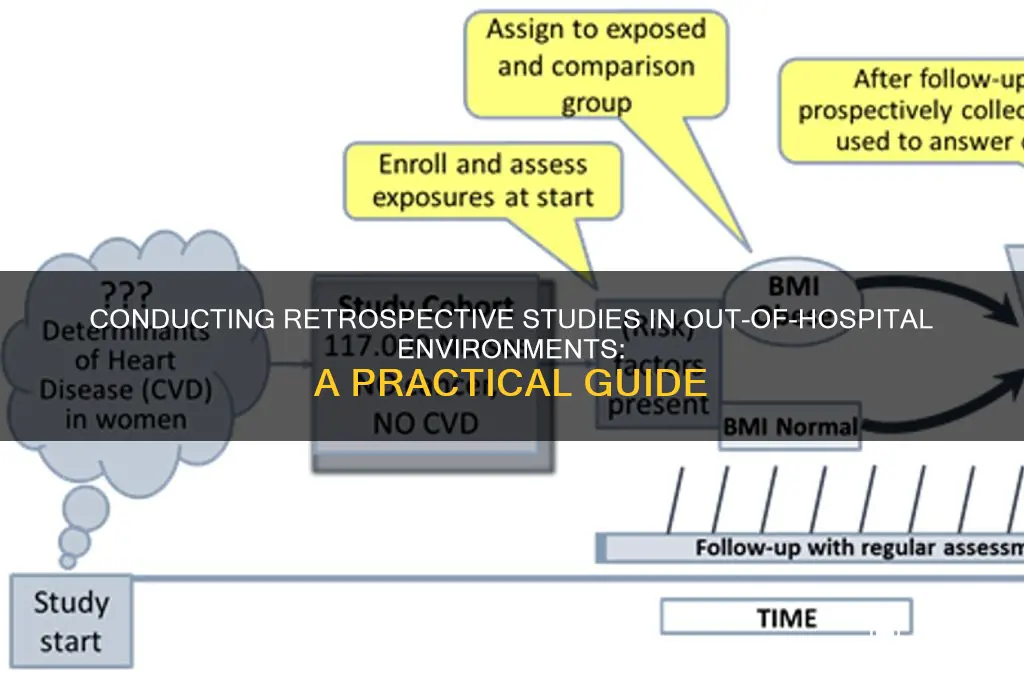
Conducting a retrospective study in an out-of-hospital setting involves analyzing existing data from past events or patient encounters to evaluate outcomes, identify trends, or assess interventions in non-clinical environments, such as emergency medical services, home care, or community health programs. Researchers typically rely on medical records, dispatch logs, or administrative databases to extract relevant information, ensuring data accuracy and completeness despite the challenges of decentralized record-keeping. Key steps include defining clear objectives, obtaining ethical approval, and employing rigorous methodologies to minimize bias, such as controlling for confounding variables and using appropriate statistical analyses. This approach allows for cost-effective insights into real-world practices, though limitations like data availability and retrospective design constraints must be carefully addressed to ensure meaningful and generalizable findings.
Explore related products






What You'll Learn
- Data Collection Methods: Identify sources, tools, and strategies for gathering retrospective data outside hospitals
- Ethical Considerations: Address privacy, consent, and confidentiality challenges in non-hospital settings
- Study Design: Define inclusion/exclusion criteria and timeframes for retrospective analysis
- Data Validation: Ensure accuracy and reliability of non-hospital data through cross-verification
- Outcome Measurement: Select appropriate metrics to evaluate outcomes in out-of-hospital contexts
![]()
Data Collection Methods: Identify sources, tools, and strategies for gathering retrospective data outside hospitals
Retrospective studies in out-of-hospital settings hinge on accessing historical data, often scattered across disparate sources. Medical records from primary care clinics, emergency medical services (EMS) agencies, and community health centers form the backbone of such studies. For instance, EMS run sheets provide critical details like patient demographics, chief complaints, interventions performed, and transport destinations. Similarly, electronic health records (EHRs) from clinics offer longitudinal data on diagnoses, medications, and follow-up care. However, these records are frequently siloed, requiring researchers to negotiate access with multiple stakeholders and ensure compliance with privacy regulations like HIPAA.
Beyond traditional medical records, alternative data sources can enrich retrospective studies. Pharmacies, for example, hold valuable information on prescription fills, which can proxy for disease prevalence or treatment adherence. Public health registries, such as cancer or immunization databases, provide population-level insights. Even non-medical sources like social services records or school health logs can shed light on social determinants of health. Leveraging these diverse sources demands creativity and persistence, as data formats and availability vary widely. Tools like data extraction templates and natural language processing (NLP) algorithms can streamline the process, though their effectiveness depends on the structure and quality of the source data.
A critical challenge in out-of-hospital retrospective studies is ensuring data accuracy and completeness. Unlike hospital settings, where records are often standardized, community-based data may suffer from inconsistencies in documentation. For example, EMS agencies might use different coding systems for patient acuity, while clinics may vary in their recording of vital signs. To mitigate this, researchers should employ validation techniques, such as cross-referencing multiple sources or conducting chart audits. Additionally, engaging local stakeholders—clinicians, administrators, or community health workers—can provide context to interpret ambiguous data and identify potential biases.
Strategically, researchers must balance depth and breadth in data collection. While comprehensive data from multiple sources strengthens a study, the logistical burden can be overwhelming. Prioritizing key variables based on the research question is essential. For instance, a study on asthma exacerbations might focus on medication refills, emergency visits, and environmental triggers rather than exhaustive clinical histories. Pilot testing data collection protocols in a subset of sites can identify bottlenecks early, allowing for iterative refinement. Collaboration with data custodians to co-design extraction tools or secure funding for data linkage initiatives can also enhance feasibility and efficiency.
Ultimately, successful retrospective data collection outside hospitals requires a blend of technical rigor and interpersonal finesse. Researchers must navigate fragmented data ecosystems, employ innovative tools, and foster partnerships to assemble a robust dataset. By thoughtfully identifying sources, validating data, and tailoring strategies to the study’s needs, researchers can unlock valuable insights into health outcomes and interventions in real-world, community settings. This approach not only advances scientific knowledge but also informs policies and practices that directly impact public health.
Community North Hospital: Induction Options for Birth Defects Explained
You may want to see also
Explore related products






![]()
Ethical Considerations: Address privacy, consent, and confidentiality challenges in non-hospital settings
Retrospective studies in non-hospital settings often rely on existing data collected for purposes other than research, such as medical records from clinics, pharmacies, or community health programs. Unlike hospital environments, these settings lack standardized data protection protocols, making privacy breaches a significant risk. For instance, a study using pharmacy records to analyze antibiotic prescribing patterns might inadvertently expose patient identities if names, addresses, or other identifiers are not properly anonymized. Researchers must implement rigorous de-identification techniques, such as removing direct identifiers and using unique study codes, to safeguard patient privacy while retaining data utility.
Obtaining informed consent in retrospective studies is inherently challenging, as data are collected after the fact. In non-hospital settings, this issue is compounded by the lack of a centralized patient population and the potential for data to be scattered across multiple sources. For example, a study examining diabetes management in community health fairs would need to consider whether participants were informed at the time of data collection that their information might be used for research. When consent is not feasible, researchers must seek ethical waivers or rely on broad consent frameworks, ensuring transparency and justifying the public health benefits of the study to ethics review boards.
Confidentiality in non-hospital settings is particularly vulnerable due to the informal nature of data storage and sharing. Community health workers, for instance, may keep records in unsecured formats or share them with third parties without formal agreements. Researchers must establish data-sharing agreements with all involved parties, ensuring that information is transmitted securely (e.g., encrypted emails or password-protected files) and stored in compliance with regulations like HIPAA or GDPR. Additionally, training data handlers on confidentiality best practices can mitigate risks of unauthorized access or disclosure.
A comparative analysis of hospital and non-hospital settings highlights the need for tailored ethical strategies. Hospitals typically have established ethics committees and data governance structures, whereas non-hospital settings often require researchers to proactively create these frameworks. For example, a study using school health records to investigate childhood obesity trends might need to collaborate with school boards to develop consent processes and data protection policies from scratch. By adopting a context-specific approach, researchers can navigate ethical challenges effectively while maintaining the integrity of their study.
In conclusion, addressing privacy, consent, and confidentiality in non-hospital retrospective studies demands a proactive and adaptive strategy. Researchers must balance the need for data accuracy with ethical obligations to protect participants. Practical steps include robust de-identification, seeking ethical waivers when consent is unattainable, securing data-sharing agreements, and educating stakeholders on confidentiality. By prioritizing these measures, researchers can ensure their studies contribute valuable insights without compromising patient trust or violating ethical standards.
Capturing the Complex Aroma of a Hospital Room: A Scent Guide
You may want to see also
Explore related products






![]()
Study Design: Define inclusion/exclusion criteria and timeframes for retrospective analysis
Defining clear inclusion and exclusion criteria is the backbone of any retrospective study, particularly in out-of-hospital settings where data heterogeneity is high. Start by identifying the population of interest based on specific characteristics such as age (e.g., adults aged 18–65), diagnosis (e.g., patients with suspected stroke), or intervention (e.g., those receiving prehospital thrombolysis). For instance, if studying the effectiveness of prehospital pain management, include patients with documented pain scores ≥7 on a 10-point scale and exclude those with contraindications to analgesics (e.g., active bleeding or allergy). Exclusion criteria might also involve incomplete medical records or cases where follow-up data is unavailable. These criteria ensure the study population is homogeneous enough to draw meaningful conclusions while maintaining external validity.
Timeframes are equally critical in retrospective studies, as they determine the scope and relevance of the analysis. Define a clear study period, such as a 5-year window (e.g., January 2018 to December 2022), to capture sufficient data while minimizing temporal bias. Consider the context of your out-of-hospital setting; for example, if analyzing prehospital trauma care, align the timeframe with changes in protocols or equipment (e.g., the introduction of a new tourniquet device in 2020). Subgroup analysis by year or season can also reveal trends, such as increased trauma cases during summer months. Ensure the timeframe allows for adequate follow-up data, especially if outcomes like 30-day mortality or hospital readmission are being assessed.
Practical tips for refining inclusion/exclusion criteria and timeframes include pilot testing on a small dataset to identify gaps or ambiguities. For instance, if "time to intervention" is a variable, clarify whether this refers to EMS arrival or medication administration. Engage stakeholders like EMS providers or emergency physicians to validate criteria, ensuring they are feasible and clinically relevant. Additionally, use electronic health records (EHRs) or prehospital databases to estimate the available sample size before finalizing criteria. For example, if studying pediatric seizures, verify that the dataset includes enough cases with documented seizure duration and treatment response to achieve statistical power.
A comparative approach highlights the trade-offs between broad and narrow criteria. Broad inclusion criteria (e.g., all patients with chest pain) increase sample size but may introduce noise from heterogeneous cases. Narrow criteria (e.g., patients with ST-elevation myocardial infarction confirmed by ECG) enhance internal validity but risk reducing generalizability. Similarly, longer timeframes capture more data but may include protocol changes or seasonal variations that confound results. For example, a study on prehospital sepsis management might exclude winter months if influenza cases skew infection rates. Balancing these factors requires iterative refinement and a clear rationale for each decision.
Finally, transparency in reporting criteria and timeframes is essential for reproducibility. Document the exact definitions used (e.g., "hypotension" defined as systolic blood pressure <90 mmHg) and justify any deviations from initial plans. For instance, if excluding patients with missing data, report the percentage excluded and assess whether this introduces bias. Tools like flow diagrams can visually depict how the final study population was derived from the initial dataset. This rigor not only strengthens the study’s credibility but also provides a roadmap for future researchers conducting similar out-of-hospital retrospective analyses.
Dana-Farber: The Leading Cancer Hospital?
You may want to see also
Explore related products





![]()
Data Validation: Ensure accuracy and reliability of non-hospital data through cross-verification
Retrospective studies in out-of-hospital settings often rely on data from diverse sources, such as electronic health records, emergency medical services reports, and patient surveys. Ensuring the accuracy and reliability of this data is critical, as errors can lead to flawed conclusions and potentially harmful interventions. Cross-verification, the process of comparing data from multiple sources to identify inconsistencies, is a cornerstone of data validation in these scenarios. For instance, if a study examines out-of-hospital cardiac arrest survival rates, cross-verifying EMS records with hospital discharge data can confirm the accuracy of survival outcomes and identify discrepancies that may arise from misreporting or data entry errors.
To implement cross-verification effectively, begin by identifying key variables that require validation, such as patient demographics, intervention details, and outcomes. For example, in a study on prehospital pain management, cross-verify the type and dosage of analgesics administered (e.g., 0.1 mg/kg of intranasal fentanyl for children aged 2–12) against both EMS logs and patient self-reports. Discrepancies, such as a recorded dose of 2 mg for a 10-kg child (0.2 mg/kg, exceeding the recommended 0.1 mg/kg), can then be flagged for further investigation. Tools like data linkage software or manual audits can streamline this process, but ensure that all sources are independently credible to avoid validating errors from a single flawed dataset.
A comparative approach highlights the importance of triangulating data from disparate sources. For example, when studying out-of-hospital stroke management, compare prehospital stroke scales (e.g., Cincinnati Prehospital Stroke Scale) documented by EMS with hospital CT scan results to validate the accuracy of field diagnoses. If 15% of cases initially flagged as strokes are later confirmed as non-stroke events, this discrepancy underscores the need for ongoing EMS training and protocol refinement. Such comparisons not only validate data but also provide actionable insights for improving care delivery.
Practical tips for successful cross-verification include standardizing data collection formats across sources to facilitate comparison and establishing clear criteria for resolving discrepancies. For instance, if a patient’s age is recorded as 65 in one dataset and 70 in another, use birthdates or identification numbers to reconcile the inconsistency. Additionally, involve stakeholders from all data-contributing entities (e.g., EMS agencies, clinics, and registries) to ensure alignment on validation protocols. Finally, document the validation process transparently, as this enhances the study’s credibility and allows for replication in future research.
In conclusion, cross-verification is not merely a technical step but a strategic imperative for ensuring the integrity of retrospective studies in out-of-hospital settings. By systematically comparing data from multiple sources, researchers can identify and rectify errors, strengthen confidence in their findings, and ultimately contribute to evidence-based improvements in prehospital care. Whether examining medication dosages, diagnostic accuracy, or patient outcomes, this methodical approach transforms raw data into reliable insights.
Hospitals and Delivery: Shaving - An Outdated Practice?
You may want to see also
Explore related products


![]()
Outcome Measurement: Select appropriate metrics to evaluate outcomes in out-of-hospital contexts
In out-of-hospital settings, outcome measurement hinges on selecting metrics that capture real-world complexities. Unlike controlled clinical environments, these contexts involve variables like patient self-management, caregiver involvement, and resource limitations. Metrics must therefore balance clinical rigor with practicality, focusing on indicators that reflect both health improvements and system efficiency. For instance, in a study of post-discharge medication adherence, metrics like percentage of doses taken (measured via pill counts or digital trackers) or emergency department revisits within 30 days provide actionable insights into both patient behavior and care continuity.
Consider the population and intervention when choosing metrics. For pediatric populations, outcomes like school attendance post-treatment or caregiver-reported quality of life may be more relevant than traditional clinical markers. In contrast, geriatric studies might prioritize metrics such as fall rates or functional independence measured by the Katz Index. For interventions like community-based diabetes management, HbA1c levels remain critical, but pairing them with patient-reported outcomes (e.g., Diabetes Distress Scale scores) offers a holistic view of success. Always align metrics with the study’s primary objectives, ensuring they are feasible to collect retrospectively without compromising validity.
A common pitfall is over-relying on administrative data, which often lacks granularity. For example, ICD-10 codes in medical records may indicate a diagnosis but fail to capture disease severity or patient-specific factors. To mitigate this, triangulate data sources—combine claims data with electronic health records (EHRs) or survey responses. In a retrospective study of out-of-hospital stroke care, linking ambulance run sheets (time to thrombolysis) with 90-day modified Rankin Scale scores from follow-up calls can reveal both process and outcome effectiveness. However, ensure data linkage complies with privacy regulations like HIPAA or GDPR.
Finally, prioritize metrics that drive actionable change. In a study of out-of-hospital palliative care, survival rates are less useful than metrics like symptom burden (measured by Edmonton Symptom Assessment Scale) or place of death (home vs. hospital). Such outcomes directly inform policy decisions, such as allocating resources to community palliative teams. Pilot testing metrics in a small sample can identify collection challenges early, ensuring scalability. For instance, if tracking pain management in home-based cancer care, test whether caregivers can reliably record pain scores using a standardized tool like the Numerical Rating Scale before full-scale implementation.
In summary, effective outcome measurement in out-of-hospital retrospective studies requires metrics tailored to population needs, data source triangulation, and a focus on actionable results. By grounding selection in these principles, researchers can transform raw data into evidence that improves care delivery beyond clinical walls.
Marshfield Hospital: Staff Strength and Healthcare Services
You may want to see also



















