Insulin dosing in hospitals is a complex process that requires careful consideration of various factors. The goal is to maintain optimal blood glucose levels for patients with diabetes, preventing complications such as hypoglycemia or hyperglycemia. The dosing regimen typically consists of basal, nutritional, and correctional insulin components, tailored to individual needs. Factors influencing insulin requirements include renal function, infection, glucocorticoid use, and nutritional intake. Initial dosing is determined by diabetes type, previous insulin experience, and glycemic control, with daily reevaluations to adjust doses based on blood glucose patterns. The use of oral diabetes medications in hospitals is controversial due to the risk of renal or hepatic failure, while the preference for scheduled doses over sliding-scale insulin is emphasized.
| Characteristics | Values |
|---|---|
| Type of insulin | Basal, nutritional, correctional |
| Patient type | Type 1, type 2, insulin-naive |
| Patient history | Previous insulin experience, diabetes control, renal function, oral intake, comorbidities, other medications |
| Patient status | NPO, renal impairment, tissue hypoxia, IV contrast, hypoglycemia, hyperglycemia, blood glucose targets |
| Insulin regimen | Basal-bolus, basal-only, short-acting premeal, long-acting, scheduled doses, sliding scale |
| Insulin type | Glargine, NPH, detemir, lispro, aspart, glulisine, regular |
| Insulin dose | Dependent on BMI, nutritional intake, blood glucose levels, patient weight, home regimen |
| Dose frequency | Daily, before meals, at bedtime |
Explore related products






What You'll Learn
- Insulin dosing depends on the patient's insulin experience, diabetes control, and renal function
- Basal, nutritional, and correctional insulin requirements must be met
- Total daily dose of insulin needed varies for type 1 and type 2 patients
- Adjust insulin doses based on BG patterns
- Selecting initial insulin doses in the hospital
![]()
Insulin dosing depends on the patient's insulin experience, diabetes control, and renal function
Insulin dosing in a hospital setting is a complex process that requires careful consideration of various factors, including the patient's insulin experience, diabetes control, and renal function. These factors play a crucial role in determining the appropriate insulin regimen and dosage for each individual patient.
Firstly, a patient's previous experience with insulin is a key consideration. For insulin-naive patients, lower doses are generally recommended when initiating therapy. This is because they may not have built up a tolerance to insulin, and starting with a lower dose helps to avoid potential complications. On the other hand, patients with prior insulin use may have a different starting dose, adjusted based on their level of pre-hospitalization glycemic control.
Secondly, baseline diabetes control is essential in determining insulin dosing. Patients with poorly controlled diabetes as outpatients may require higher basal doses of insulin, ranging from 0.5 to 0.8 units/kg body weight/day. Conversely, patients with well-controlled diabetes or frequent hypoglycemia may need a reduced basal dose. Assessing home BG control is an important aspect of understanding a patient's diabetes control.
Lastly, renal function is a critical factor in insulin dosing. Renal impairment can affect insulin metabolism and excretion, leading to adjustments in insulin dosage. For example, in patients with type 2 diabetes and renal impairment, initiating insulin therapy with a lower dose of 0.25 units/kg/day instead of 0.5 units/kg/day can reduce the incidence of hypoglycemia without compromising the glucose-lowering effect. Additionally, studies have shown that insulin dosage requirements can vary depending on renal function, with lower dosages needed as eGFR decreases.
Other considerations in insulin dosing include the patient's current oral intake, comorbidities, and other medications. Some patients may only require a basal insulin dose, while others may benefit from additional short-acting premeal doses. Correctional insulin doses may also be necessary, depending on the patient's BMI. Furthermore, the selection of an insulin regimen, such as the basal-bolus approach or sliding-scale regimen, should be based on the patient's diabetes control and renal function to optimize glycemic control and reduce complications.
In summary, insulin dosing in hospitalized patients requires a personalized approach that takes into account their insulin experience, diabetes control, and renal function. By carefully considering these factors, healthcare providers can determine the most appropriate insulin regimen and dosage to effectively manage blood glucose levels and improve patient outcomes.
Special Surgery Hospital: Top-Ranked in the Nation
You may want to see also
Explore related products






![]()
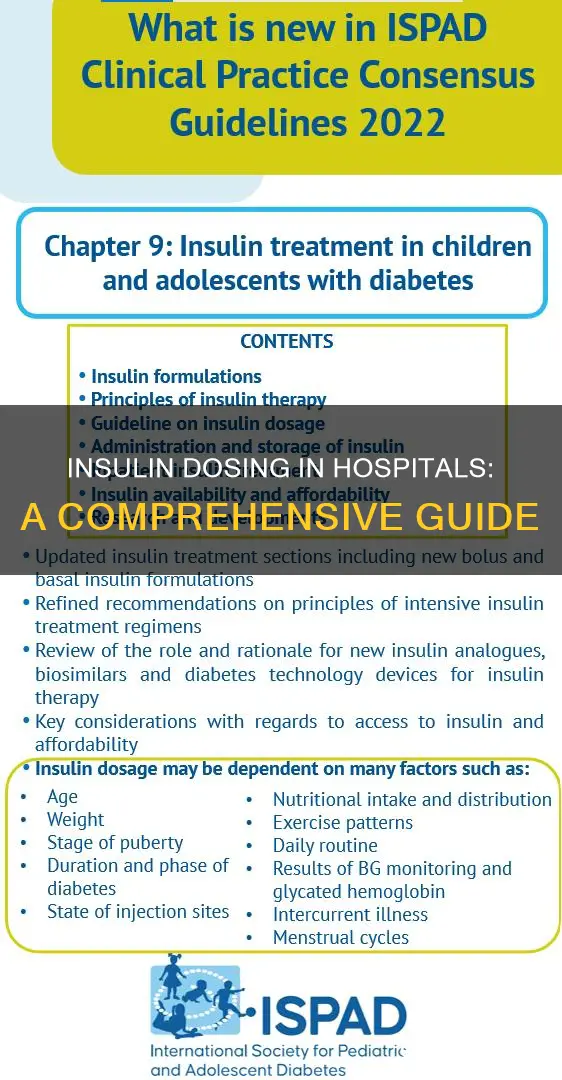
Basal, nutritional, and correctional insulin requirements must be met
All patients have basal, nutritional, and correctional insulin requirements that must be met with endogenous insulin or with insulin provided to them.
Basal insulin is needed even when the patient is not eating to control gluconeogenesis. It is typically administered once daily in the AM or at bedtime using glargine, NPH (at bedtime or AM and bedtime), or detemir (once daily or every 12 hours). Alternatively, a continuous insulin infusion can be used. Approximately half of the daily dose should be given as basal insulin.
Nutritional insulin is used to cover carbohydrate intake from food, dextrose in IV fluid, tube feeds, and TPN. It is administered using rapid-acting insulin (aspart, lispro, or glulisine) or short-acting insulin (regular). The nutritional insulin dose is determined based on meal consumption and titrated up as necessary. It is typically given within 30 minutes before a meal for regular insulin and within 15 minutes for rapid-acting insulin.
Correctional insulin is given to bring high blood glucose levels down to the target range (typically below 150 mg/dL pre-meal and below 200 mg/dL at bedtime). It is also administered using rapid-acting insulin (aspart, lispro, glulisine) or short-acting insulin (regular). The correctional dose is selected based on the patient's BMI, with sensitive, average, and resistant categories.
It is important to note that the insulin regimen may vary depending on the patient's previous experience with insulin, baseline diabetes control, renal function, current oral intake, comorbidities, and other medications. Additionally, the basal insulin regimen can be continued from home if the patient has been well-controlled, but the dose may need to be adjusted to reduce the risk of hypoglycemia.
Bacteria Implicated in Hospital Infections: A Common Threat
You may want to see also
Explore related products






![]()
Total daily dose of insulin needed varies for type 1 and type 2 patients
The total daily dose of insulin needed varies depending on whether a patient has type 1 or type 2 diabetes. For type 1 diabetes, patients generally require approximately 0.4 to 1.0 units of insulin per kg per day, with a typical starting dose of 0.5 units/kg/day. This total daily dose can be divided into basal insulin, which is given when the patient is not eating, and premeal insulin, which is given in thirds before each meal.
For type 2 diabetes, the insulin dose varies depending on the patient's insulin resistance, ranging from 0.5 to 2 units per kg per day. Type 2 patients with renal impairment may require a lower starting dose of 0.25 units per kg per day.
For both type 1 and type 2 diabetes, the basal insulin dose is typically given at night and works for 24 hours or more. The premeal insulin, also known as nutritional insulin, is usually a rapid-acting or short-acting insulin taken within 30 minutes before a meal to help the body process carbohydrates from food. The specific insulin regimen and doses should be determined in consultation with a doctor, taking into account the patient's weight, lifestyle, and other individual factors.
Additionally, correctional insulin may be required based on the patient's BMI and blood glucose levels. It is important to monitor blood glucose levels closely, especially when initiating insulin therapy, to prevent hypoglycemia and ensure effective glucose management.
Blood Supply: Hospitals' Constant Need
You may want to see also
Explore related products






![]()
Adjust insulin doses based on BG patterns
Adjusting insulin doses based on BG patterns involves several considerations, including the types of insulin, the patient's glucose levels, and individual factors such as appetite, renal function, and risk for hypoglycaemia.
Firstly, it is crucial to differentiate between the types of insulin: basal, nutritional, and correctional. Basal insulin is typically adjusted based on fasting glucose levels. It is considered appropriately dosed when it maintains glucose readings within a stable range from night to morning, assuming the patient has not consumed any food. If a patient is taking just basal insulin and experiences high fasting readings, an increase in the basal dose may be necessary. However, it is also important to address high bedtime readings first, as they can contribute to high fasting levels.
Nutritional insulin, on the other hand, is adjusted based on pre-meal glucose levels. If there is a significant increase in glucose levels from before breakfast to before lunch, the total insulin dose (nutritional plus correctional) at breakfast should be increased and become the new nutritional dose for the next day's breakfast. If the glucose level before breakfast is high but the level at lunch is within the target range, no change in the nutritional dose is required for the following day. Additionally, if the glucose level after breakfast or before lunch is low, the breakfast nutritional dose should be decreased for the subsequent day.
Correctional insulin is used to bring high blood glucose levels down to the target range. When adjusting correctional insulin, it is essential to consider the patient's BMI and insulin sensitivity. For example, a sensitive BMI is considered <20 or requiring <50 units/day, while a resistant BMI is >30 or requiring >90 units/day.
When adjusting insulin doses, it is important to address patterns of lows or frequent hypoglycaemia first for safety reasons. If a patient experiences lows before supper, the lunch bolus may need to be reduced. If there are significant low readings throughout the day, a decrease in basal insulin may be warranted, especially if basal insulin exceeds 60% of the total daily dose of insulin.
It is also crucial to monitor blood glucose levels regularly. In general, BG levels should be checked before meals and at bedtime. For patients who are NPO (nothing by mouth) or receiving continuous tube feeds, BG levels should be checked every 4 to 6 hours. Additionally, if a patient is starting a continuous tube feed, insulin infusion therapy may be considered, following hospital-specific standardized protocols.
Griffin Hospital: Hartford Healthcare Affiliate?
You may want to see also
Explore related products






![]()
Selecting initial insulin doses in the hospital
Selecting the initial insulin dose for hospitalised patients with diabetes requires careful consideration of various factors. The insulin regimen depends on the patient's insulin history, diabetes control, and renal function. Lower doses are generally recommended for insulin-naive patients or those with renal impairment.
For patients new to insulin therapy, a starting dose of 0.1-0.2 units per kilogram of body weight is recommended. This can be administered using an insulin pen or a vial and syringe. The use of a vial and syringe may be challenging for individuals with poor vision or dexterity. Insulin pens, on the other hand, offer ease of use and dose accuracy.
For patients with type 2 diabetes and renal impairment, initiating insulin therapy with a lower dose of 0.25 units per kg per day has been shown to effectively lower glucose levels while reducing the risk of hypoglycaemia.
If a patient has been well-controlled with a home insulin regimen, it is generally recommended to continue this regimen in the hospital. However, to reduce the risk of in-hospital hypoglycaemia, it may be advisable to reduce the total dose by 20-30% or start with bedtime insulin (such as glargine, detemir, or NPH) at a dose of 0.2 units/kg.
For patients who are eating, insulin injections should be aligned with meals. Pre-meal blood glucose testing is recommended within 30 minutes of the start of a meal, and rapid-acting insulin should be administered within 10 minutes before or after the meal. For patients with diabetes who are fasting, blood glucose testing is recommended every four to six hours.
Get Admitted to a Hospital: A Step-by-Step Guide
You may want to see also
Frequently asked questions
There are three types of insulin doses: basal, nutritional, and correctional. Basal insulin is needed even when the patient is not eating to control gluconeogenesis. Nutritional insulin covers carbohydrate intake from food, dextrose in IVF, tube feeds, and TPN. Correctional insulin is selected based on BMI and is either rapid or short-acting.
The insulin dose depends on the patient's previous experience with insulin, baseline diabetes control, and renal function. Other factors to consider include the patient's current oral intake, comorbidities, and other medications. The total daily dose of insulin needed varies with the type of diabetes: type 1 patients require approximately 0.4-0.5 units/kg/day, while type 2 patients may require 0.5 to 2 units/kg/day due to varying insulin resistance.
Insulin doses should be re-evaluated on a daily basis to achieve goals and adapt to the patient's changing clinical situation.