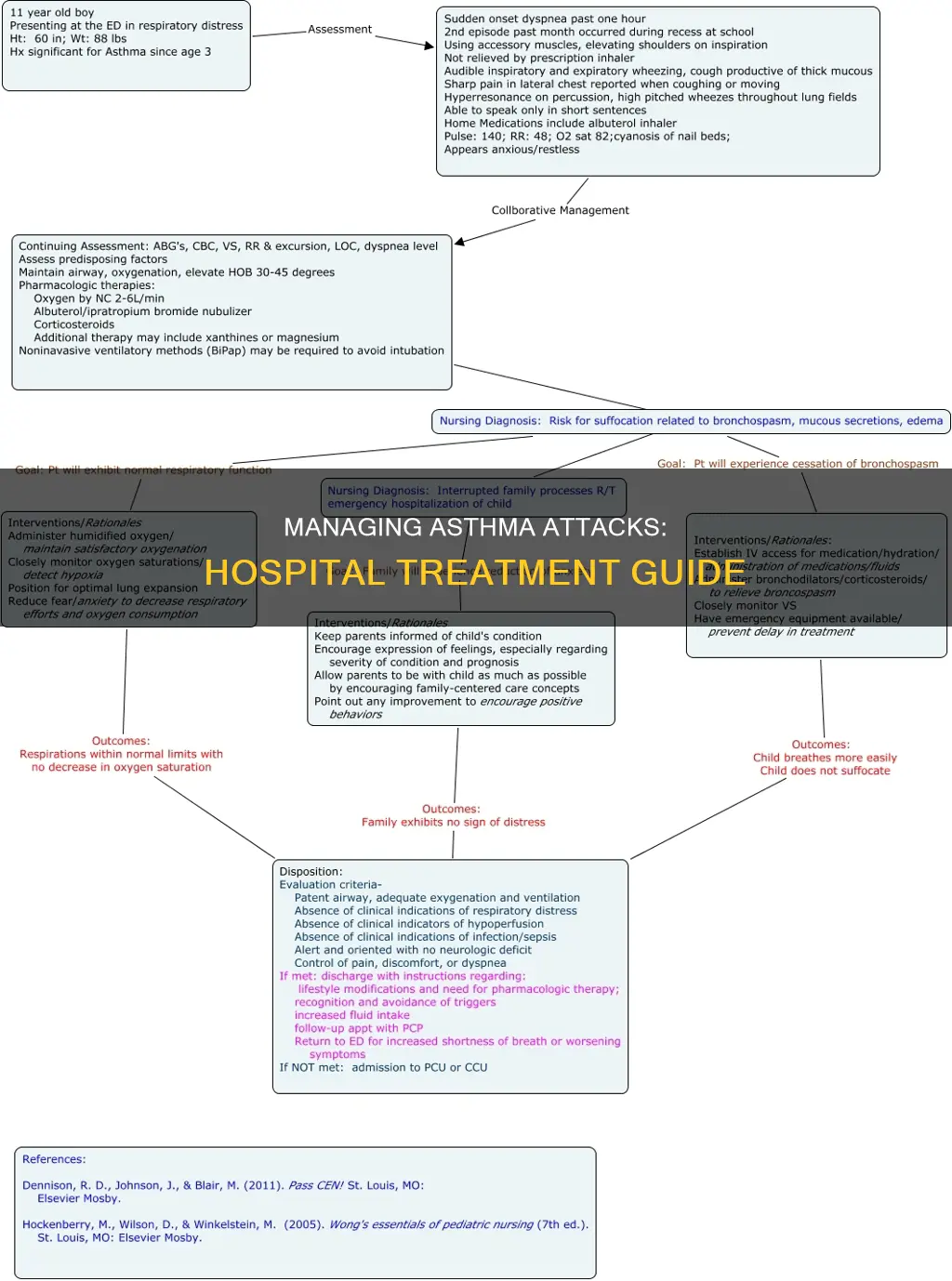
Asthma attacks can quickly become medical emergencies, so it's important to know how to manage them in a hospital setting. The first step is to assess the severity of the attack, which can be done using scoring systems like the Pediatric Respiratory Assessment Measure (PRAM). This is followed by frequent assessments to evaluate the patient's response to treatment. The optimal treatment time is within the first hour, and medications should be adjusted according to the progression, severity, and response to asthma therapy. This includes the administration of magnesium sulfate for patients who did not respond well initially and the use of aminophylline in severe cases.
| Characteristics | Values |
|---|---|
| Asthma attack symptoms | Shortness of breath, coughing, wheezing, chest tightness, reduced lung function |
| Action required | Asthma Action Plan, asthma first aid, reliever medication |
| Action in case of emergency | Call emergency services, administer adrenaline autoinjector if anaphylaxis, give 4 puffs of reliever puffer, repeat until breathing returns to normal |
| Assessment in hospital | Static assessment to determine severity, frequent assessments to evaluate response to treatment |
| Treatment in hospital | Inhaled steroids, magnesium sulfate, aminophylline, heliox, non-invasive ventilation, intubation |
Explore related products






What You'll Learn
![]()
Administer first aid and seek urgent medical attention
If you or someone you know is experiencing an asthma attack, it is important to remain calm and know that asthma attacks can quickly become asthma emergencies. If you are experiencing any of the following symptoms, follow your asthma action plan and provide yourself with first aid:
- A progressive increase in shortness of breath
- Coughing
- Wheezing
- Chest tightness
- A decrease in exercise tolerance
- Impairment of daily activities
- Progressive reduction in lung function
If you do not have an asthma action plan, or are assisting someone who is experiencing an asthma attack, start asthma first aid immediately. Do not wait until asthma symptoms become severe. If the person is known to have anaphylaxis, ALWAYS GIVE AN ADRENALINE AUTO-INJECTOR FIRST, and then a reliever, even if there are no skin symptoms.
If the person does not have anaphylaxis, give 4 separate puffs of a blue/grey reliever puffer:
- Shake the puffer.
- Put 1 puff into the spacer.
- Get the person to take 4 breaths from the spacer.
- Repeat until 4 puffs have been taken.
If there is no improvement, give 4 more separate puffs of the blue/grey reliever, repeating steps 1-4. If breathing does not return to normal, call an ambulance and keep giving the person 4 separate puffs, taking 4 breaths for each puff, every 4 minutes until emergency assistance arrives.
Spinal Research Hospital in Ohio: Where Is It?
You may want to see also
Explore related products






![]()
Use a reliever puffer
If you or someone you know is experiencing an asthma attack, it is important to remain calm and know how to use a reliever puffer. Relievers are medicines used to ease asthma symptoms and usually come in a blue or grey inhaler (puffer) device. The most common short-acting bronchodilator is salbutamol, also known as the 'blue puffer'. Terbutaline is another reliever medication.
To use a reliever puffer, follow these steps:
- Shake the puffer.
- Put 1 puff into the spacer.
- Get the person experiencing asthma symptoms to take 4 breaths from the spacer.
- Repeat steps 2 and 3 until a total of 4 puffs have been taken.
If you do not have a spacer, follow these steps instead:
- Shake the puffer.
- Give 1 puff as the person takes 1 slow, deep breath.
- Hold the breath for as long as comfortable.
- Repeat steps 1 to 3 until all puffs are taken.
It is important to remember that a reliever puffer should start working within 4 minutes and usually lasts at least 4 hours. If there is no improvement after using the reliever puffer, give 4 more puffs as instructed above. If breathing does not return to normal, seek urgent medical attention and continue to give the person 4 separate puffs, taking 4 breaths for each puff, every 4 minutes until emergency assistance arrives.
Dilated and Hospitalized: What's the Connection?
You may want to see also
Explore related products






![]()
Assess the severity of the attack
Asthma exacerbations can be classified as mild, moderate, severe, or life-threatening. The severity of an asthma attack is determined by a patient's symptoms, physical examination, lung function, and oxygen saturation. Lung function is a useful method of assessment, with a peak expiratory flow (PEF) of 40% or less of the predicted function indicating a severe attack in patients over five years old.
When assessing the severity of an asthma attack, it is important to consider the patient's medical history and background chronic asthma severity. A history of hospital admissions for asthma, previous ICU admissions, and increasing use of β-agonist inhalers are all markers of an increased baseline risk of death. The amount of β-agonist used during the exacerbation is also informative, as increasing use is associated with a greater likelihood of hospital admission and/or risk of death.
In terms of symptoms, it is important to note that not all people wheeze during an asthma attack. Anxiety and worry are common emotional symptoms that can make it harder to make decisions. Patients should be encouraged to act on warning signs and take action if something doesn't feel right, rather than waiting for symptoms to become severe.
Pulse oximetry is a suitable means of assessing ventilatory status in patients with severe asthma. It measures oxygen saturation and can help identify concurrent arterial desaturation and hypercarbia, which normally only develop in life-threatening asthma. Analysis of arterial blood gases can be reserved for patients with oxygen saturations below 92% or those who do not respond to initial treatment. A normal Paco2 value in a breathless asthmatic is a warning sign of impending hypoventilation, and values above 6 kPa indicate a life-threatening attack and the probable need for ICU transfer.
Medicaid Coverage at U of M Hospital: What You Need to Know
You may want to see also
Explore related products






![]()
Administer magnesium sulfate if the patient doesn't respond to initial therapy
If a patient experiencing an asthma attack does not respond to initial therapy, a doctor may administer magnesium sulfate. This is because magnesium sulfate is a bronchodilator, meaning it relaxes the bronchial muscles and expands the airways, allowing more air to flow in and out of the lungs. This can relieve symptoms of asthma, such as shortness of breath.
Magnesium sulfate can be administered in a few different ways. It can be inhaled using a nebulizer, or it can be given intravenously. The dosage of intravenous magnesium sulfate typically ranges from 1.2 g to 2 g, although this may vary depending on the patient's weight and age. For example, the dosage for children ranged from 25 to 75 mg per kg in the studies reviewed by Cochrane.
The scientific evidence for the effectiveness of magnesium sulfate in treating asthma attacks is inconsistent. While some studies have shown that it can reduce the number of hospitalizations and improve lung function in people with acute asthma, others have failed to demonstrate a "clinically worthwhile benefit". However, it is still a recommended treatment for patients with acute asthma exacerbations who have not responded to first-line therapy, which typically includes bronchodilators and corticosteroids.
It is important to note that there can be adverse effects associated with the administration of magnesium sulfate. The most commonly reported adverse effects include flushing, fatigue, nausea, headache, and tingling or burning at the administration site. There is also a risk of hypotension and vasodilation, although these effects are less common.
Hospitals and Perinatal Units: Who Has Them?
You may want to see also
Explore related products





![]()
Intubate only as a last resort
Intubation is a procedure performed to keep patients from dying due to respiratory exhaustion, which can lead to apnea and hypoxemia. However, it should be viewed as a last resort for treating asthma attacks in a hospital setting.
The main goal of non-invasive ventilation for acute asthma is to avoid intubation by reducing the load on respiratory muscles, allowing the patient to rest and giving other therapies time to work. Non-invasive ventilation has several advantages over intubation: less sedation is required, the patient can talk and drink fluids, and there is a lower risk of ventilator-associated pneumonia.
In most cases of respiratory failure complicating acute asthma, the standard approach is to sedate, intubate, and start mechanical ventilation. However, this should be avoided if possible due to the risk of serious complications. For example, aggressive bagging can cause severe gas-trapping in the lungs, which may lead to pneumothorax or hypotension.
Before considering intubation, it is recommended to first attempt non-invasive ventilation using a tight-fitting, full-face mask. If the patient does not relax within 15-30 minutes and remains in distress, short-acting opiates and sedatives may be administered, and intubation considered.
In summary, while intubation can be life-saving in severe cases of asthma, it should be approached with caution due to the risk of complications. Non-invasive ventilation and other therapies should always be explored first as a last resort.
Best Hospitals in Phoenix: Your Top Choices
You may want to see also
Frequently asked questions
If someone is having an asthma attack, start asthma first aid immediately. Give them 4 separate puffs of their blue/grey reliever puffer. If they don't have a spacer, instruct them to take one puff as they take one slow, deep breath, holding it for as long as they can. Repeat this process until all puffs are taken. If there is no improvement, give 4 more puffs. If breathing still hasn't returned to normal, call an ambulance.
An asthma attack can come on gradually over hours or days, or it can get worse very quickly, in seconds or minutes. Signs include a progressive increase in shortness of breath, coughing, wheezing, chest tightness, and a reduction in lung function. Not everyone wheezes during an asthma attack.
If the person has an anaphylaxis action plan, follow the instructions. Always give an adrenaline injector first, then an asthma reliever.
Commence asthma first aid. Ensure the person takes their reliever medication. If they don't have an asthma action plan, they should see a doctor as soon as possible.
In the hospital, the severity of the asthma attack will be assessed, and treatment will be adjusted according to progression, severity, and response to asthma therapy. Inhaled steroids are not used in exacerbation cases. Instead, magnesium sulfate administration may be used, and in severe cases, aminophylline may be administered in the PICU.