Putting on hospital ECG leads correctly is essential for obtaining accurate cardiac readings. The process begins by ensuring the patient’s chest is clean and dry to improve electrode adhesion. Start by identifying the standard 12-lead ECG placement: place the right arm (RA) lead on the right shoulder or arm, the left arm (LA) lead on the left shoulder or arm, and the left leg (LL) lead on the left leg or ankle. For the chest leads, position V1 on the fourth intercostal space to the right of the sternum, V2 on the fourth intercostal space to the left of the sternum, V3 midway between V2 and V4, V4 on the fifth intercostal space in the midclavicular line, V5 horizontally even with V4 in the anterior axillary line, and V6 horizontally even with V4 and V5 in the midaxillary line. Ensure each electrode is firmly attached and connected to the ECG machine to avoid signal interference. Proper placement guarantees reliable results for diagnosing cardiac conditions.
Explore related products





What You'll Learn
- Lead Placement Locations: Identify V1-V6, RA, LA, RL, LL positions on the chest
- Skin Preparation: Clean and dry skin for better electrode adhesion
- Electrode Attachment: Secure leads firmly to ensure accurate readings
- Lead Wire Connection: Attach wires to ECG machine correctly
- Patient Positioning: Ensure patient is supine and relaxed during placement
![]()
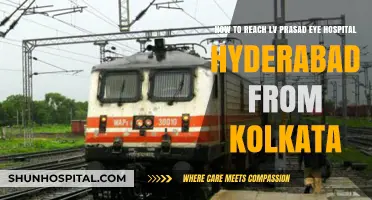
Lead Placement Locations: Identify V1-V6, RA, LA, RL, LL positions on the chest
When placing ECG leads on the chest, it’s crucial to accurately identify the positions for V1-V6, RA (Right Arm), LA (Left Arm), RL (Right Leg), and LL (Left Leg) to ensure precise readings. The V leads (V1-V6) are placed on the anterior chest wall and are essential for assessing the heart’s electrical activity in the frontal plane. V1 is positioned on the fourth intercostal space (ICS) at the right sternal border, while V2 is placed on the fourth ICS at the left sternal border, directly opposite V1. These two leads provide a view of the heart’s septal and anterior walls. To locate V3, draw an imaginary line connecting V2 and V4 (which will be placed later), and position V3 at the midpoint of this line, typically in the fourth ICS.
Moving to the lateral chest wall, V4 is placed on the fifth ICS in the midclavicular line, offering a view of the anterior and lateral walls of the heart. V5 is positioned horizontally level with V4 but in the anterior axillary line, while V6 is placed on the fifth ICS at the midaxillary line. V5 and V6 provide insights into the lateral and left ventricular activity. Proper alignment of these leads is critical to avoid misinterpreting the ECG results.
The limb leads—RA, LA, RL, and LL—are placed on the extremities but are referenced here for completeness. RA is positioned on the right upper arm, typically near the deltoid or biceps, while LA is placed on the left upper arm in a similar fashion. RL and LL are placed on the right and left lower limbs, respectively, usually on the ankles or wrists if lower limb placement is not feasible. These leads help assess the heart’s electrical axis and are essential for a 12-lead ECG.
When placing the leads, ensure the patient’s chest is clean and dry to improve electrode adhesion. Use anatomical landmarks to confirm correct placement, such as the sternal border and intercostal spaces. For V1 and V2, feel the sternal notch and count down to the fourth ICS. For V4-V6, locate the midclavicular, anterior axillary, and midaxillary lines, respectively, while maintaining the correct ICS.
Finally, double-check all lead positions before starting the ECG to avoid artifacts or incorrect readings. Proper lead placement is fundamental to obtaining accurate diagnostic information, so take the time to verify each electrode’s location. This meticulous approach ensures the ECG reflects the heart’s true electrical activity.
Hospital Bound: Packing Newborn Outfits
You may want to see also
Explore related products






![]()
Skin Preparation: Clean and dry skin for better electrode adhesion
Before applying ECG electrodes to a patient's chest, proper skin preparation is essential to ensure accurate readings and comfortable adhesion. The first step in this process is to clean the skin thoroughly. Use a mild soap or a skin-cleansing wipe to remove any dirt, oil, or residue that may interfere with electrode contact. Gently rub the soapy solution onto the areas where the electrodes will be placed, typically the chest, shoulders, and sides. Ensure that you cover a slightly larger area than where the electrodes will be positioned to guarantee a clean surface. This step is crucial as any impurities on the skin can create a barrier, reducing the quality of the ECG signal.
After cleaning, it is imperative to dry the skin completely. Moisture left on the skin can affect electrode adhesion and may cause discomfort to the patient. Use a soft, lint-free towel to pat the skin dry, being careful not to irritate the area. Avoid rubbing, as this can cause skin abrasion and potentially affect the ECG results. Proper drying ensures that the skin's surface is ready for the adhesive electrodes, promoting better contact and reducing the chances of the electrodes falling off during the procedure.
In some cases, especially with hairy individuals, shaving the chest area might be necessary. Hair can interfere with electrode adhesion and signal transmission. If shaving is required, do so gently and carefully, ensuring the skin is not irritated or damaged. Shaving should be done prior to cleaning to avoid any potential issues with soap and hair removal. Always prioritize patient comfort and ensure they are informed about the process to alleviate any concerns.
For patients with particularly dry or flaky skin, consider using a skin prep gel or adhesive spray. These products can enhance electrode adhesion and improve the overall quality of the ECG tracing. Apply a small amount of the gel or spray to the cleaned and dried skin, following the manufacturer's instructions. Allow it to dry completely before proceeding with electrode placement. This additional step can be beneficial for ensuring a secure and long-lasting electrode attachment.
Proper skin preparation is a critical aspect of obtaining accurate ECG readings. By cleaning and drying the skin effectively, healthcare professionals can ensure optimal electrode adhesion, leading to reliable results. This process contributes to the overall success of the ECG procedure and patient satisfaction. It is a simple yet vital step that should not be overlooked in the electrode application process.
Santa Rosa Sutter Hospital: A Trauma Center?
You may want to see also
Explore related products






![]()
Electrode Attachment: Secure leads firmly to ensure accurate readings
Proper electrode attachment is crucial for obtaining accurate ECG readings. Begin by ensuring the patient’s chest is clean, dry, and free of oils or lotions, as these can interfere with conductivity. Use alcohol wipes to gently clean the areas where the electrodes will be placed, allowing the skin to dry completely before proceeding. This step ensures optimal contact between the electrodes and the skin, reducing the risk of signal interference.
Next, identify the correct placement of the ECG leads on the chest. The standard 12-lead ECG requires six electrodes: RA (right arm), LA (left arm), RL (right leg), LL (left leg), V1, and V2. For the precordial leads (V1-V6), place V1 in the fourth intercostal space to the right of the sternum and V2 in the fourth intercostal space to the left of the sternum. Ensure each electrode is firmly pressed onto the skin, with the adhesive side making full contact. Proper placement minimizes movement and ensures consistent signal capture.
When attaching the leads, peel the backing from the adhesive electrode and place it directly onto the prepared skin site. Press firmly around the edges to secure it in place. Avoid stretching the skin, as this can cause discomfort and affect readings. For limb leads (RA, LA, RL, LL), wrap the electrodes securely around the designated areas, ensuring they are tight enough to stay in place but not so tight as to restrict circulation. Double-check that all electrodes are flat and securely attached before proceeding.
To further ensure stability, use ECG lead wires with clips or snaps that firmly connect to the electrodes. Attach each wire to its corresponding electrode, ensuring a snug fit. Loose connections can result in poor signal transmission and inaccurate readings. Once all leads are connected, gently tug on each wire to confirm they are securely attached to the electrodes. This step is essential for maintaining signal integrity throughout the ECG recording.
Finally, instruct the patient to remain still during the procedure, as movement can dislodge the electrodes or introduce artifacts into the reading. If any electrode appears loose or falls off during the test, pause the recording, reattach it securely, and resume. Consistent and firm electrode attachment is the foundation of a reliable ECG, ensuring the healthcare provider can accurately interpret the heart’s electrical activity.
Henry Ford Hospitals: A Comprehensive Healthcare Network
You may want to see also
Explore related products






![]()
Lead Wire Connection: Attach wires to ECG machine correctly
Before attaching the ECG leads to the patient’s chest, it is crucial to correctly connect the lead wires to the ECG machine. Start by identifying the ports on the ECG machine labeled for the specific leads (e.g., RA, LA, RL, LL, V1-V6). Each lead wire corresponds to a specific port, typically color-coded or labeled for easy identification. Ensure the ECG machine is turned off or in standby mode to avoid any interference during the connection process. Carefully insert each lead wire into its designated port, matching the colors or labels on the wires to those on the machine. For example, the red wire is usually for RA (right arm), yellow for LA (left arm), green for RL (right leg), black for LL (left leg), and the remaining wires for the chest leads (V1-V6). Double-check that all wires are securely connected to prevent loose connections, which can result in inaccurate readings.
Once the wires are attached to the ECG machine, inspect the connectors for any signs of damage or wear. Faulty connectors can compromise the quality of the ECG tracing. If any issues are detected, replace the wires or connectors before proceeding. Ensure the clips or pins on the wires are functioning properly, as these will be used to attach the electrodes to the patient’s skin. Gently tug on each wire to confirm it is firmly connected to the machine. Proper connection at this stage is essential, as it ensures the electrical signals from the patient’s heart are accurately transmitted to the ECG machine for interpretation.
Next, organize the lead wires to avoid tangling, which can cause discomfort to the patient and interfere with the placement of the electrodes. Some ECG machines have wire holders or clips to keep the wires neatly arranged. If available, use these to secure the wires in place. If not, carefully drape the wires over the patient’s body in a way that allows easy access to each electrode site. Ensure the wires are not pulled too tightly, as this can dislodge the electrodes or cause discomfort during the procedure. Proper wire management not only facilitates smooth lead placement but also reduces the risk of accidental disconnection during the ECG recording.
After organizing the wires, turn on the ECG machine and verify that all leads are functioning correctly. Most machines display a lead status indicator or perform an automatic check to ensure all connections are active. If any leads are not recognized, recheck the wire connections at both the machine and the electrode ends. Sometimes, a loose connection or incorrect placement can cause a lead to appear inactive. Resolving these issues before placing the electrodes on the patient saves time and ensures a seamless ECG recording process.
Finally, before proceeding to place the electrodes on the patient’s chest, confirm that the ECG machine is ready to record. Ensure the paper or digital display is set up correctly and that the machine is calibrated if necessary. Once everything is in order, you can proceed with attaching the electrodes to the patient’s chest, following the standard lead placement guidelines. Correct lead wire connection is the foundation of a successful ECG, ensuring accurate and reliable results for proper diagnosis and patient care.
VCA Animal Hospital: Drug Testing Policy for Employees
You may want to see also
Explore related products






![]()
Patient Positioning: Ensure patient is supine and relaxed during placement
When preparing to place ECG leads on a patient's chest, proper patient positioning is crucial for accurate readings and patient comfort. Begin by ensuring the patient is in a supine position, lying flat on their back on a comfortable surface such as an examination table or bed. This position allows easy access to the chest and ensures the leads adhere correctly to the skin. The supine position also helps maintain consistent lead placement, which is essential for obtaining reliable ECG results. If the patient has difficulty lying flat, use pillows to support their head and lower back, but ensure the chest remains unobstructed.
Next, create a relaxed environment to help the patient remain calm and still during the procedure. Encourage the patient to breathe normally and avoid unnecessary movement, as tension or fidgeting can interfere with lead placement and signal quality. Dim the lights if possible and maintain a quiet atmosphere to minimize distractions. If the patient is anxious, explain the process in simple terms and reassure them that the procedure is non-invasive and painless. A relaxed patient is more likely to remain still, making it easier to position the leads accurately.
Before beginning, ensure the patient’s chest is exposed and free of any clothing or obstructions that could interfere with lead placement. Gently drape a sheet or gown to maintain modesty while keeping the chest area accessible. If the patient has excessive hair on the chest, consider gently shaving or clipping the area to improve electrode adhesion, though this should only be done with the patient’s consent. Clean the skin with alcohol wipes to remove oils or dirt, as this ensures the leads stick securely and maintain proper contact with the skin.
During placement, communicate clearly with the patient to maintain their cooperation. Instruct them to keep their arms resting comfortably at their sides, avoiding any upward movement that could strain the chest muscles. If the patient tends to shift or move, ask them to focus on a fixed point in the room or close their eyes to help them stay still. Maintain a gentle and reassuring tone throughout the process to keep the patient at ease. Proper positioning and relaxation not only facilitate accurate lead placement but also enhance the overall quality of the ECG recording.
Finally, verify the patient’s comfort once they are positioned. Check that the table or bed is not too hard and that the room temperature is pleasant. If the patient feels cold, offer a warm blanket, but ensure it does not cover the chest area. Comfort is key to ensuring the patient remains supine and relaxed throughout the procedure. Once the patient is correctly positioned and at ease, proceed with placing the ECG leads, following the standard lead placement guidelines for accurate readings.
Hospitals' Emergency Response to Anirestic Shock
You may want to see also
Frequently asked questions
Place the RA lead on the right side of the chest, just below the clavicle (collarbone), ensuring it adheres firmly to the skin for accurate readings.
Position the LA lead on the left side of the chest, also below the clavicle, mirroring the placement of the RA lead for symmetry and proper signal capture.
The RL lead is not placed on the chest; instead, it should be attached to the right leg, typically on the calf or ankle, to serve as a grounding electrode.
Place V1 in the 4th intercostal space (between the 4th and 5th ribs) at the right sternal border, and V2 in the same space but at the left sternal border.
V3 is placed midway between V2 and V4. V4 is in the 5th intercostal space at the midclavicular line. V5 is in the same horizontal plane as V4 but at the anterior axillary line. V6 is in the same horizontal plane as V4 and V5 but at the midaxillary line.