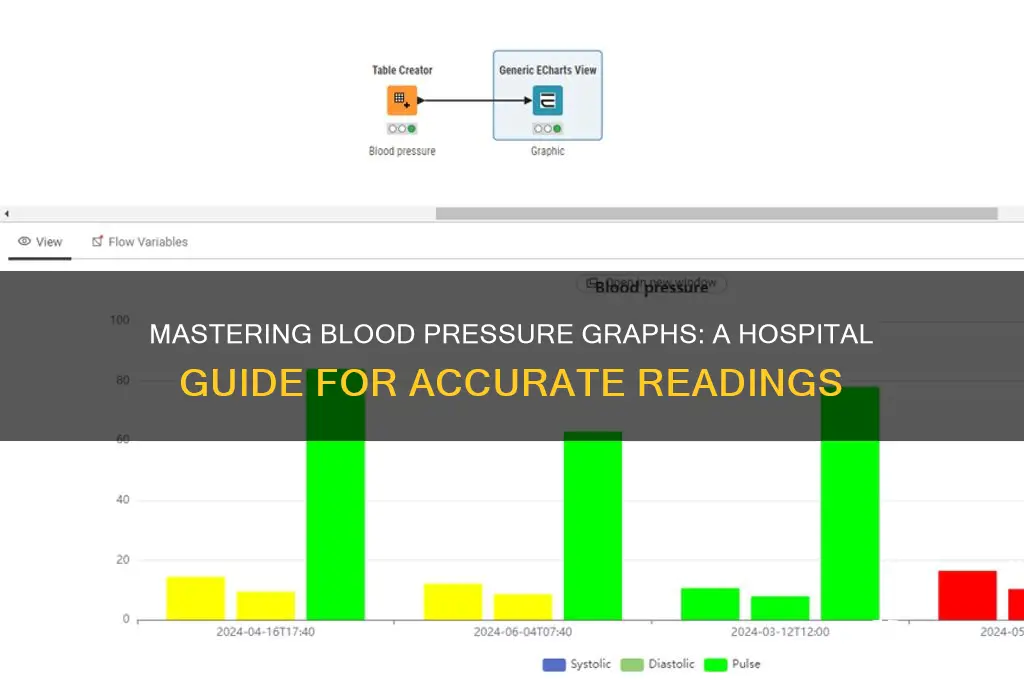
Reading a blood pressure graph in a hospital setting is a critical skill for healthcare professionals, as it provides essential insights into a patient’s cardiovascular health and overall condition. These graphs, often displayed on patient monitors or printed from electronic health records, typically plot systolic and diastolic blood pressure values over time, along with heart rate. Understanding how to interpret these graphs involves recognizing trends such as consistent elevations or drops in pressure, irregular patterns, or sudden spikes, which may indicate conditions like hypertension, hypotension, or arrhythmias. Key components to focus on include the baseline values, the range of fluctuations, and any correlations with patient activities or interventions. Accurate interpretation ensures timely and appropriate medical responses, making it a vital tool for monitoring and managing patient care.
| Characteristics | Values |
|---|---|
| Systolic Pressure | The higher number; represents the force at which your heart pumps blood into the arteries when it contracts. Normal range: 90-120 mmHg. |
| Diastolic Pressure | The lower number; represents the pressure in the arteries when the heart rests between beats. Normal range: 60-80 mmHg. |
| Trend Line | A line connecting data points over time, showing whether blood pressure is stable, rising, or falling. |
| Time Stamp | Indicates when each reading was taken, usually in hours and minutes. |
| Alarms/Thresholds | Set limits (e.g., high or low) that trigger alerts if blood pressure exceeds or falls below these values. |
| Pulse Rate | Often displayed alongside blood pressure; normal range: 60-100 beats per minute. |
| Waveform | Visual representation of blood flow, showing the pressure changes during each heartbeat (if available). |
| Hypertension Indicators | Readings consistently above 130/80 mmHg may indicate hypertension. |
| Hypotension Indicators | Readings consistently below 90/60 mmHg may indicate hypotension. |
| Annotations | Notes added by healthcare providers (e.g., medication administration, patient activity). |
| Graph Scale | Vertical axis represents pressure (mmHg), horizontal axis represents time. |
| Data Points | Individual readings plotted on the graph, often represented as dots or markers. |
Explore related products






What You'll Learn
- Understanding BP Graph Axes: Learn X-axis (time) and Y-axis (pressure) for accurate interpretation
- Identifying Systolic/Diastolic Trends: Spot patterns in high and low pressure values over time
- Recognizing Alarms: Decode alerts for hypertension, hypotension, or irregular readings
- Analyzing Waveforms: Interpret shape and amplitude for cardiac function insights
- Comparing Baseline Data: Use historical graphs to track patient progress or deterioration
![]()
Understanding BP Graph Axes: Learn X-axis (time) and Y-axis (pressure) for accurate interpretation
When interpreting a blood pressure (BP) graph in a hospital setting, understanding the axes is fundamental to accurate analysis. The X-axis represents time, typically plotted horizontally. This axis shows the duration over which blood pressure measurements were taken, often in hours or minutes. It allows healthcare providers to track BP trends over time, identifying patterns such as fluctuations, stability, or responses to interventions. For example, a sudden spike or drop in BP can be correlated with specific events, such as medication administration or patient activity, by referencing the time on the X-axis.
The Y-axis, plotted vertically, represents pressure, specifically the systolic and diastolic blood pressure values. Systolic pressure (the higher number) measures the force on artery walls when the heart beats, while diastolic pressure (the lower number) measures the force when the heart is at rest. The Y-axis is typically labeled with numerical values in millimeters of mercury (mmHg), ranging from normal levels (e.g., 120/80 mmHg) to hypertensive or hypotensive ranges. Understanding this axis is crucial for assessing whether BP readings fall within safe limits or indicate a potential health concern.
To accurately interpret a BP graph, it’s essential to recognize how the X-axis (time) and Y-axis (pressure) interact. For instance, a steady horizontal line on the graph indicates consistent BP over time, while a jagged or wavy line suggests variability. By aligning specific time points on the X-axis with corresponding pressure values on the Y-axis, clinicians can pinpoint critical moments, such as when BP exceeded safe thresholds or responded to treatment. This dual-axis analysis provides a comprehensive view of a patient’s cardiovascular status.
Additionally, some BP graphs may include multiple lines or colors to differentiate between systolic and diastolic pressures. In such cases, the Y-axis remains the reference for pressure values, while the X-axis continues to track time. Familiarizing oneself with these visual distinctions ensures precise interpretation. For example, if the systolic line consistently rises above the normal range while the diastolic line remains stable, it may indicate specific cardiovascular issues that require attention.
Lastly, mastering the X-axis (time) and Y-axis (pressure) is key to using BP graphs as a diagnostic and monitoring tool. It enables healthcare professionals to detect trends, evaluate treatment efficacy, and make informed decisions. Regular practice in correlating time-based events with pressure changes enhances the ability to provide timely and effective patient care. By focusing on these axes, clinicians can transform raw data into actionable insights, ensuring better management of blood pressure-related conditions.
Jackson Memorial Hospital Marianna, Florida: Ascension Association Explained
You may want to see also
Explore related products





![]()
Identifying Systolic/Diastolic Trends: Spot patterns in high and low pressure values over time
When analyzing a blood pressure graph in a hospital setting, identifying systolic and diastolic trends is crucial for understanding a patient's cardiovascular health. The graph typically plots time on the x-axis and blood pressure values on the y-axis, with separate lines for systolic (the higher number) and diastolic (the lower number) pressures. Begin by examining the overall trajectory of these lines. A consistent upward trend in systolic pressure over several readings may indicate worsening hypertension, while a downward trend could suggest hypotension or the effectiveness of treatment. Similarly, observe the diastolic line for patterns; persistent high diastolic values above 90 mmHg are concerning, whereas consistently low values below 60 mmHg may signal poor organ perfusion.
Next, look for fluctuations or spikes in both systolic and diastolic pressures. Irregular patterns, such as sudden peaks or valleys, could point to conditions like arrhythmias, stress responses, or medication effects. For example, a systolic pressure that intermittently spikes above 180 mmHg, coupled with diastolic values remaining stable, might suggest episodic hypertension or white coat syndrome. Conversely, a diastolic pressure that fluctuates widely without a corresponding systolic change could indicate autonomic dysfunction or fluid imbalances. Documenting the timing of these fluctuations can help correlate them with patient activities, meals, or medication administration.
Comparing systolic and diastolic trends relative to each other provides additional insights. A widening gap between systolic and diastolic pressures (increased pulse pressure) often occurs with aging or arterial stiffness, while a narrowing gap might be seen in conditions like heart failure or shock. For instance, if systolic pressure remains elevated but diastolic pressure drops significantly, this could signal severe hypotension or inadequate cardiac output. Conversely, if both systolic and diastolic pressures rise together, it may reflect systemic hypertension or increased vascular resistance.
Finally, assess the consistency and variability of systolic and diastolic values over time. A stable pattern with minimal variation suggests well-controlled blood pressure, whereas high variability (e.g., systolic pressure swinging between 120 and 180 mmHg) is associated with increased cardiovascular risk. Long-term trends are particularly valuable; for example, a gradual increase in both systolic and diastolic pressures over days or weeks may indicate worsening hypertension, while a steady decline could reflect improving health or medication efficacy. Always correlate these trends with the patient's clinical status and other diagnostic findings for a comprehensive interpretation.
Minimizing Surgery Costs: Strategies for Patients and Hospitals
You may want to see also
Explore related products






![]()
Recognizing Alarms: Decode alerts for hypertension, hypotension, or irregular readings
In a hospital setting, blood pressure graphs are vital tools for monitoring patients' cardiovascular health, and understanding how to interpret these graphs is crucial for recognizing alarms related to hypertension, hypotension, or irregular readings. When examining a blood pressure graph, the first step is to identify the systolic and diastolic pressure lines, typically represented by different colors or line styles. Systolic pressure, the higher number, indicates the force at which your heart pumps blood around the body when it contracts. Diastolic pressure, the lower number, represents the pressure in the arteries when the heart is at rest between beats. Normal blood pressure readings typically fall below 120/80 mmHg, and recognizing deviations from this range is essential for identifying potential issues.
Alarms for hypertension, or high blood pressure, are triggered when readings consistently exceed 130/80 mmHg. On a blood pressure graph, this would be evident by the systolic line remaining above 130 mmHg and the diastolic line above 80 mmHg over multiple readings. Hypertension alarms may also be accompanied by additional indicators, such as a steady increase in pressure over time or a widening gap between systolic and diastolic readings. It is crucial to respond promptly to hypertension alerts, as prolonged high blood pressure can lead to serious complications, including heart disease, stroke, and kidney damage.
On the other hand, hypotension, or low blood pressure, alarms are generated when readings consistently fall below 90/60 mmHg. In this case, the blood pressure graph would show the systolic line dropping below 90 mmHg and the diastolic line below 60 mmHg. Hypotension alerts may be triggered by various factors, including dehydration, blood loss, or certain medications. While low blood pressure is not always a cause for concern, it can lead to inadequate blood flow to vital organs, resulting in dizziness, fainting, or shock. Recognizing hypotension alarms and addressing the underlying cause is essential for preventing complications.
Irregular blood pressure readings, characterized by sudden spikes or drops, can also trigger alarms on the graph. These irregularities may be caused by factors such as stress, anxiety, or underlying medical conditions. When decoding irregular reading alerts, look for patterns or trends on the graph, such as periodic fluctuations or a consistent deviation from the patient's baseline. It is essential to investigate the cause of irregular readings, as they may indicate an underlying issue requiring medical attention. In some cases, irregular blood pressure patterns may be a sign of conditions like arrhythmia, pheochromocytoma, or other cardiovascular disorders.
To effectively recognize alarms on a blood pressure graph, it is vital to establish a patient's baseline readings and monitor for deviations over time. This involves reviewing previous graph data, noting any trends or patterns, and comparing current readings to established norms. Additionally, consider the patient's medical history, current medications, and any relevant clinical information when interpreting blood pressure graph alarms. By developing a comprehensive understanding of blood pressure graph interpretation, healthcare professionals can promptly identify and respond to alarms, ensuring timely interventions and improved patient outcomes. Regular monitoring and accurate decoding of alerts are crucial components of effective blood pressure management in a hospital setting.
Broadmoor Hospital: A Look at Its Past and Present
You may want to see also
Explore related products






![]()
Analyzing Waveforms: Interpret shape and amplitude for cardiac function insights
Analyzing waveforms on a blood pressure graph, often displayed on hospital monitors, provides critical insights into cardiac function. The shape and amplitude of these waveforms, typically derived from arterial lines or non-invasive blood pressure (NIBP) measurements, reflect the dynamics of the cardiovascular system. The waveform consists of three main components: the upslope, peak, and downslope, each corresponding to different phases of the cardiac cycle. The upslope represents ventricular contraction (systole), the peak indicates peak systolic pressure, and the downslope reflects ventricular relaxation (diastole) and aortic valve closure. Understanding these components is essential for interpreting cardiac performance and identifying abnormalities.
The amplitude of the waveform directly correlates with stroke volume and systemic vascular resistance. A high-amplitude waveform suggests increased stroke volume or elevated vascular resistance, while a low-amplitude waveform may indicate decreased cardiac output or hypotension. For example, in hypovolemic shock, the waveform often appears dampened with reduced amplitude due to inadequate preload. Conversely, in hypertensive patients, the waveform typically shows increased amplitude due to heightened vascular resistance. Monitoring amplitude trends over time helps clinicians assess the effectiveness of interventions, such as fluid resuscitation or vasopressor therapy.
The shape of the waveform provides additional clues about cardiac and vascular health. A normal waveform is characterized by a sharp upslope, distinct peak, and gradual downslope. Deviations from this shape can signal specific pathologies. For instance, a slow upslope may indicate aortic stenosis or severe left ventricular dysfunction, as the heart struggles to eject blood efficiently. A notch in the downslope, known as a "dicrotic notch," reflects aortic valve closure and is typically prominent in healthy individuals. Its absence or diminution can suggest aortic regurgitation or stiffened arteries.
Another critical aspect is the damping of the waveform, which occurs when the pressure transduction system is not properly flushed or calibrated. Overdamped waveforms appear flattened, making it difficult to distinguish systolic and diastolic phases, while underdamped waveforms show excessive oscillations. Properly interpreting waveform shape requires ensuring the monitoring system is correctly set up to avoid misleading conclusions. Clinicians must also correlate waveform findings with other clinical data, such as heart sounds, electrocardiograms, and patient symptoms, for a comprehensive assessment.
In summary, analyzing waveforms on a blood pressure graph involves evaluating both amplitude and shape to derive insights into cardiac function. Amplitude reflects stroke volume and vascular resistance, while shape provides clues about specific cardiac and vascular conditions. Recognizing abnormalities in these parameters enables timely interventions and improves patient outcomes. Mastery of waveform interpretation is a vital skill for healthcare professionals, ensuring accurate monitoring and management of critically ill patients in hospital settings.
Mogadishu's Hospitality: Unveiling the Cultural Roots of Somali Generosity
You may want to see also
Explore related products






![]()
Comparing Baseline Data: Use historical graphs to track patient progress or deterioration
When comparing baseline data using historical blood pressure graphs to track a patient's progress or deterioration, it's essential to establish a clear reference point. Begin by identifying the patient's initial or baseline blood pressure readings, typically recorded during their first hospital visit or at the start of a treatment plan. These baseline values serve as the foundation for all subsequent comparisons. For example, if a patient's initial systolic blood pressure was 140 mmHg and diastolic was 90 mmHg, these numbers become the benchmark against which future readings are measured. Ensure that the baseline data is accurately documented, including the date and time, to maintain consistency in your analysis.
Once the baseline is established, plot subsequent blood pressure readings on the same graph to visualize trends over time. Use distinct colors or symbols to differentiate between systolic and diastolic measurements, making it easier to track changes. When comparing these readings to the baseline, look for patterns such as consistent increases or decreases in blood pressure. For instance, if a patient’s systolic pressure drops from 140 mmHg to 120 mmHg over several weeks, this may indicate improvement, especially if the patient is on antihypertensive medication. Conversely, a steady rise above the baseline could signal deterioration or treatment ineffectiveness. Always consider the context, such as changes in medication, lifestyle, or underlying health conditions, when interpreting these trends.
Another critical aspect of comparing baseline data is assessing the variability of blood pressure readings. A stable blood pressure graph with minimal fluctuations around the baseline suggests consistent health status or effective treatment. However, significant variability, such as sudden spikes or drops, may indicate instability or complications. For example, if a patient’s blood pressure alternates between 130/80 mmHg and 160/100 mmHg over a short period, this could point to issues like medication non-compliance, stress, or an underlying condition like white coat hypertension. Comparing these variations to the baseline helps in identifying anomalies early and adjusting the care plan accordingly.
In addition to tracking individual readings, calculate averages over specific periods to smooth out short-term fluctuations and gain a clearer picture of long-term trends. For instance, compare the average blood pressure over the past month to the baseline average. If the monthly average shows a consistent decrease toward the normal range (e.g., <120/80 mmHg), this confirms progress. Conversely, an upward trend in the average readings may warrant further investigation or intervention. This method of comparing averages to baseline data provides a more objective measure of the patient’s overall trajectory.
Finally, use historical graphs to correlate blood pressure trends with other clinical data, such as symptoms, lab results, or medication adjustments. For example, if a patient’s blood pressure begins to rise after a change in medication, the graph can help determine whether the new drug is ineffective or if the dosage needs adjustment. Similarly, if a patient reports symptoms like dizziness or headaches, compare these episodes to the blood pressure graph to identify potential correlations. By integrating baseline data with other clinical information, healthcare providers can make more informed decisions and tailor treatment plans to the patient’s specific needs.
Accessing Medical Records at NYC's Metropolitan Hospital: A Step-by-Step Guide
You may want to see also
Frequently asked questions
The top number, or systolic pressure, represents the force at which your heart pumps blood into the arteries when it contracts.
The bottom number, or diastolic pressure, measures the pressure in the arteries when the heart rests between beats.
Hypertension is indicated by readings consistently above 130/80 mmHg, while hypotension is shown by readings below 90/60 mmHg. Always consult a healthcare professional for interpretation.































