Heart failure remains a leading cause of hospital readmissions, posing significant challenges to patient health and healthcare systems. However, one hospital has successfully implemented innovative strategies to reduce readmission rates, offering valuable insights for others. By focusing on comprehensive discharge planning, patient education, and post-discharge follow-up, this hospital has achieved remarkable results. Their approach includes personalized care plans, interdisciplinary team collaboration, and leveraging technology for remote monitoring. This story highlights the potential for targeted interventions to improve patient outcomes and reduce the burden of heart failure readmissions.
| Characteristics | Values |
|---|---|
| Hospital Name | Not explicitly mentioned in the source, but the story is based on a real hospital's experience |
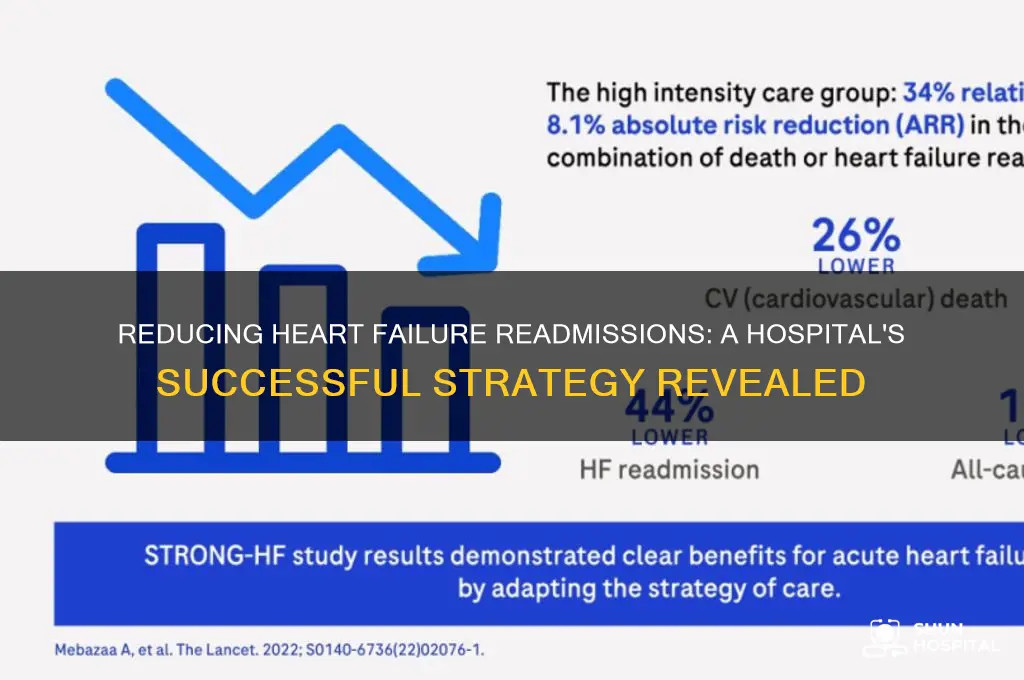
| Readmission Rate (Baseline) | 24.4% (within 30 days of discharge for heart failure patients) |
| Readmission Rate (After Intervention) | 12.2% (a 50% reduction) |
| Intervention Period | 18 months |
| Key Strategies | 1. Structured Discharge Planning: Included medication reconciliation, follow-up appointments, and clear discharge instructions. 2. Patient Education: Focused on symptom recognition, medication management, and lifestyle modifications. 3. Post-Discharge Phone Calls: Nurses called patients within 48 hours of discharge to assess their condition and address concerns. 4. Collaborative Care Teams: Involved pharmacists, dietitians, and social workers in patient care. 5. Telemonitoring: Implemented for high-risk patients to track vital signs remotely. |
| Patient Population | Heart failure patients (specific demographics not detailed in the source) |
| Outcome Measures | 30-day readmission rates, patient satisfaction, and healthcare costs |
| Cost Savings | Estimated $1.2 million in avoided readmission costs over 18 months |
| Staff Involvement | Multidisciplinary team including nurses, physicians, pharmacists, and social workers |
| Technology Used | Telemonitoring devices, electronic health records (EHR) for tracking patient data |
| Follow-Up Period | 30 days post-discharge |
| Sustainability | Strategies were integrated into standard care protocols to ensure long-term success |
| Challenges Addressed | Medication non-adherence, lack of patient understanding, and delayed follow-up care |
| Patient Engagement | Increased through personalized education and proactive communication |
| Data Source | Hospital's internal records and quality improvement reports |
Explore related products






What You'll Learn
- Early Follow-Up Appointments: Scheduling post-discharge visits within 7 days reduces readmissions significantly
- Patient Education Programs: Teaching self-care and medication management empowers patients to avoid complications
- Care Transition Coordination: Seamless handoffs between hospital and home care teams improve outcomes
- Remote Monitoring Systems: Using telehealth and wearable devices tracks health changes proactively
- Multidisciplinary Team Approach: Involving nurses, pharmacists, and social workers ensures comprehensive care planning
![]()
Early Follow-Up Appointments: Scheduling post-discharge visits within 7 days reduces readmissions significantly
Early follow-up appointments within 7 days of hospital discharge have emerged as a critical strategy for reducing heart failure readmission rates. This approach addresses a vulnerable period when patients transition from the structured hospital environment to self-care at home. During this time, medication adherence, symptom management, and lifestyle adjustments are often challenging, increasing the risk of complications. Scheduling a follow-up visit within this narrow window allows healthcare providers to identify and address issues before they escalate into emergencies requiring readmission. This proactive intervention ensures continuity of care and reinforces patient education, which is essential for long-term management of heart failure.
The effectiveness of early follow-up appointments lies in their ability to bridge the gap between hospital and home care. During these visits, providers can assess patients for signs of worsening heart failure, such as weight gain, shortness of breath, or fluid retention. They can also review medication regimens, ensuring patients understand dosages and potential side effects. Additionally, these appointments provide an opportunity to educate patients on dietary restrictions, fluid management, and the importance of daily weight monitoring. By addressing these factors early, hospitals can empower patients to take control of their health and prevent exacerbations that lead to readmissions.
Implementing a system for early follow-up appointments requires careful planning and coordination. Hospitals must establish protocols to ensure that discharge planners schedule these visits before patients leave the hospital. This may involve integrating electronic health records (EHRs) with scheduling systems to automate reminders for both patients and providers. Hospitals should also consider offering flexible appointment times, including weekends or evenings, to accommodate patients' schedules and reduce no-shows. Collaboration between cardiologists, primary care physicians, and nurse practitioners can further enhance the effectiveness of these visits by providing comprehensive care tailored to each patient's needs.
Another key aspect of early follow-up appointments is the use of multidisciplinary teams. Involving pharmacists, dietitians, and social workers in these visits can address additional barriers to care, such as medication affordability, dietary challenges, or lack of social support. For example, a pharmacist can review medications for potential interactions or side effects, while a dietitian can provide personalized nutrition advice. Social workers can assist with resources for transportation, financial assistance, or home health services, ensuring patients have the support they need to manage their condition effectively. This holistic approach maximizes the impact of early follow-up visits and fosters better health outcomes.
Finally, measuring the success of early follow-up appointments is essential for continuous improvement. Hospitals should track readmission rates, patient satisfaction, and adherence to treatment plans to evaluate the effectiveness of this strategy. Data analytics can identify trends or gaps in care, allowing hospitals to refine their protocols and address specific challenges. Sharing success stories and best practices within the healthcare community can also inspire other institutions to adopt similar initiatives. By prioritizing early follow-up appointments, hospitals can significantly reduce heart failure readmissions, improve patient outcomes, and enhance the overall quality of care.
Should I Stay with My Mom at the Hospital? A Guide
You may want to see also
Explore related products






![]()
Patient Education Programs: Teaching self-care and medication management empowers patients to avoid complications
Patient Education Programs play a pivotal role in reducing heart failure readmission rates by equipping patients with the knowledge and skills necessary to manage their condition effectively. One hospital’s success story highlights how structured self-care and medication management training can empower patients to avoid complications and maintain their health. These programs begin with comprehensive education sessions that explain heart failure in simple terms, emphasizing the importance of daily self-care practices such as monitoring weight, fluid intake, and symptoms like shortness of breath or swelling. Patients are taught to recognize early warning signs of worsening heart failure, enabling them to take proactive steps before their condition deteriorates.
Medication management is another critical component of these education programs. Many heart failure patients are prescribed multiple medications, including diuretics, beta-blockers, and ACE inhibitors, which can be confusing to manage. The hospital’s program includes hands-on training where patients learn how to organize their medications, understand dosages, and track when to take each pill. Nurses and pharmacists work directly with patients to address concerns, clarify side effects, and ensure adherence. By simplifying medication routines and providing tools like pill organizers or mobile apps, patients are less likely to miss doses or misuse medications, reducing the risk of complications that lead to readmission.
Self-care education extends beyond medication to lifestyle modifications that are essential for managing heart failure. Patients are taught the importance of a low-sodium diet, regular physical activity, and avoiding tobacco and alcohol. The hospital’s program includes cooking classes, exercise demonstrations, and support groups to make these changes more achievable. By involving family members or caregivers in the education process, patients gain a support system that reinforces healthy habits at home. This holistic approach ensures that patients understand how their daily choices impact their heart health and empowers them to make informed decisions.
Follow-up and reinforcement are key to the success of patient education programs. The hospital implemented a system of regular check-ins, either in-person or via telehealth, to monitor patients’ progress and address any challenges they face. These follow-ups allow healthcare providers to reinforce self-care principles, adjust medication plans as needed, and provide emotional support. Additionally, patients are given access to educational materials, such as brochures and online resources, to refresh their knowledge over time. This ongoing support helps patients stay engaged and motivated, reducing the likelihood of readmission due to mismanagement of their condition.
The impact of these patient education programs is evident in the hospital’s reduced readmission rates. By teaching self-care and medication management, patients become active participants in their own care, leading to better health outcomes and fewer hospital visits. This approach not only improves quality of life for patients but also reduces the financial and resource burden on the healthcare system. The hospital’s story serves as a model for other institutions seeking to implement effective strategies to combat heart failure readmissions, demonstrating that education and empowerment are powerful tools in chronic disease management.
Pneumonia Treatment: Hospital Care and Recovery
You may want to see also
Explore related products






![]()
Care Transition Coordination: Seamless handoffs between hospital and home care teams improve outcomes
Effective care transition coordination is a cornerstone of reducing heart failure readmission rates, as demonstrated by the success story of one hospital that implemented a structured handoff process between hospital and home care teams. The hospital recognized that fragmented care transitions often lead to gaps in patient understanding, medication errors, and inadequate follow-up, all of which contribute to readmissions. To address this, they developed a seamless handoff protocol that ensured continuity of care from the moment a patient was discharged. This included a standardized discharge checklist, clear communication of post-discharge care plans, and the involvement of home care teams in the transition process. By aligning hospital and home care providers, the hospital created a cohesive care pathway that significantly improved patient outcomes.
A critical component of this strategy was the designation of a care transition coordinator—a nurse or case manager responsible for overseeing the entire discharge process. This coordinator acted as a liaison between the hospital team, the patient, and the home care providers, ensuring that all parties were informed and aligned. The coordinator conducted thorough assessments to identify patients at high risk for readmission, such as those with complex medication regimens or limited social support. For these patients, the coordinator arranged follow-up appointments within 72 hours of discharge and provided detailed instructions on symptom management, diet, and activity levels. This proactive approach empowered patients to manage their condition effectively at home, reducing the likelihood of complications that could lead to readmission.
The hospital also implemented a structured communication system to facilitate seamless handoffs. Prior to discharge, the care transition coordinator held a multidisciplinary team meeting to review the patient’s care plan, ensuring that all providers—including home health nurses, pharmacists, and primary care physicians—were on the same page. A comprehensive discharge summary was then created, which included medication lists, diagnostic results, and specific care instructions. This document was shared electronically with the home care team and the patient’s primary care provider, eliminating delays and reducing the risk of miscommunication. Additionally, the coordinator followed up with the home care team within 48 hours of discharge to address any concerns and ensure the patient was stable.
Education played a pivotal role in the hospital’s care transition coordination efforts. Patients and their caregivers received personalized training on heart failure management, including how to monitor symptoms like weight gain or shortness of breath, which are early indicators of worsening condition. The hospital also provided written materials and access to telehealth resources for ongoing support. By equipping patients with the knowledge and tools to manage their health, the hospital fostered a sense of ownership and confidence, reducing the anxiety often associated with transitioning from hospital to home.
Finally, the hospital established a feedback loop to continuously improve its care transition processes. They tracked readmission rates and conducted regular audits of discharge practices to identify areas for enhancement. Patient and caregiver surveys provided valuable insights into their experiences during the transition, highlighting successes and challenges. This data-driven approach allowed the hospital to refine its protocols, ensuring that care transitions remained patient-centered and effective. As a result, the hospital achieved a significant reduction in heart failure readmission rates, demonstrating that seamless handoffs between hospital and home care teams are essential for improving outcomes and enhancing the quality of care.
Essential Hospital Nurse Gifts: Thoughtful Ideas to Show Appreciation
You may want to see also
Explore related products





![The Hospital [DVD]](https://m.media-amazon.com/images/I/61oQ2sBPcmL._AC_UY218_.jpg)
![]()
Remote Monitoring Systems: Using telehealth and wearable devices tracks health changes proactively
Remote monitoring systems have emerged as a transformative tool in reducing heart failure readmission rates by enabling proactive tracking of patients’ health changes outside traditional clinical settings. Leveraging telehealth platforms and wearable devices, these systems allow healthcare providers to continuously monitor vital signs such as heart rate, blood pressure, weight, and oxygen saturation in real time. For heart failure patients, sudden weight gain or fluctuations in blood pressure can be early indicators of fluid retention or worsening conditions, which are common triggers for readmissions. By detecting these changes early, providers can intervene before symptoms escalate, preventing hospital readmissions and improving patient outcomes.
Wearable devices, such as smartwatches and Bluetooth-enabled scales, play a pivotal role in remote monitoring by seamlessly integrating into patients’ daily lives. These devices collect data effortlessly, reducing the burden on patients to manually track their health metrics. For instance, a smart scale can automatically transmit daily weight measurements to a telehealth platform, where algorithms flag abnormal trends. If a patient gains more than 2-3 pounds in 24 hours—a critical red flag for heart failure—the system alerts the care team, who can then contact the patient to adjust medications or schedule a follow-up visit. This immediate response capability is key to preventing decompensation and subsequent readmissions.
Telehealth platforms serve as the backbone of remote monitoring systems, aggregating data from wearable devices and providing actionable insights to healthcare providers. These platforms often include dashboards that highlight at-risk patients, enabling care teams to prioritize interventions. Additionally, telehealth facilitates virtual consultations, allowing providers to educate patients on symptom management, medication adherence, and lifestyle modifications. For heart failure patients, this ongoing support fosters a sense of accountability and empowers them to take an active role in their care, further reducing the likelihood of readmissions.
Implementing remote monitoring systems requires a structured approach to ensure effectiveness. Hospitals must first identify high-risk heart failure patients who would benefit most from these programs. Next, patients need comprehensive training on using wearable devices and understanding the importance of consistent data transmission. Care teams should also establish clear protocols for responding to alerts, ensuring timely and appropriate interventions. Finally, integrating remote monitoring data into electronic health records (EHRs) streamlines communication and enables longitudinal tracking of patient progress.
The success of remote monitoring systems is evident in hospitals that have implemented such programs. For example, one hospital reported a 30% reduction in heart failure readmissions within six months of adopting a telehealth and wearable device program. Patients expressed higher satisfaction with their care, citing increased peace of mind and better communication with their providers. By proactively tracking health changes and enabling early interventions, remote monitoring systems not only reduce readmission rates but also enhance the overall quality of care for heart failure patients. As technology advances, these systems are poised to become a cornerstone of chronic disease management, revolutionizing how hospitals approach patient care.
Viera's Teaching Hospitals: What You Need to Know
You may want to see also
Explore related products

![]()
Multidisciplinary Team Approach: Involving nurses, pharmacists, and social workers ensures comprehensive care planning
A multidisciplinary team approach is a cornerstone strategy for reducing heart failure readmission rates, as demonstrated by successful hospital initiatives. By involving nurses, pharmacists, and social workers in the care planning process, hospitals can address the complex needs of heart failure patients more effectively. Nurses play a pivotal role in this model, serving as the primary point of contact for patients. They conduct thorough assessments, monitor symptoms, and educate patients on medication adherence, lifestyle modifications, and symptom recognition. Their continuous presence ensures that patients receive consistent, personalized care, which is critical for managing chronic conditions like heart failure. Nurses also act as care coordinators, facilitating communication among team members to ensure that all aspects of the patient’s health are addressed.
Pharmacists are another essential component of the multidisciplinary team, contributing their expertise in medication management. Heart failure patients often require complex medication regimens, and pharmacists can optimize these by reviewing prescriptions for efficacy, potential drug interactions, and adherence barriers. They also provide counseling to patients, explaining the purpose of each medication, potential side effects, and the importance of taking them as directed. By integrating pharmacists into the care team, hospitals can reduce medication-related complications, a common cause of readmissions. Additionally, pharmacists can assist in transitioning patients from hospital to home by ensuring they have access to affordable medications and understand their treatment plans.
Social workers bring a unique perspective to the team by addressing the psychosocial and environmental factors that impact heart failure management. They assess patients’ living situations, financial constraints, and support systems, identifying barriers to care such as lack of transportation, food insecurity, or inadequate housing. Social workers connect patients with community resources, such as meal delivery services, transportation assistance, or financial aid programs, to mitigate these challenges. By addressing these social determinants of health, social workers help patients maintain stability and adhere to their care plans, reducing the likelihood of readmission. Their involvement ensures that care planning extends beyond medical treatment to encompass the holistic needs of the patient.
The synergy of these professionals in a multidisciplinary team creates a comprehensive care plan tailored to each patient’s unique needs. Regular team meetings and shared documentation platforms foster collaboration, ensuring that all team members are aligned on the patient’s goals and progress. This coordinated approach not only improves patient outcomes but also enhances efficiency by preventing overlapping efforts and gaps in care. Hospitals implementing this model have reported significant reductions in readmission rates, as patients receive consistent, holistic support throughout their care journey.
To maximize the effectiveness of a multidisciplinary team approach, hospitals should invest in training and resources that promote interdisciplinary collaboration. This includes establishing clear roles and responsibilities, providing ongoing education on heart failure management, and leveraging technology to streamline communication. By empowering nurses, pharmacists, and social workers to work together seamlessly, hospitals can deliver high-quality, patient-centered care that addresses the multifaceted challenges of heart failure. This proactive, team-based strategy is a proven method for reducing readmissions and improving long-term outcomes for heart failure patients.
Silent Night or Chaos? Christmas Carols in Psychiatric Hospitals
You may want to see also
Frequently asked questions
The hospital focused on patient education, care coordination, follow-up appointments within 7 days of discharge, medication reconciliation, and a structured discharge process.
They developed easy-to-understand educational materials, provided one-on-one sessions with nurses, and emphasized the importance of diet, exercise, and medication adherence.
A dedicated care coordinator was assigned to each patient to ensure seamless communication between healthcare providers, schedule follow-ups, and address post-discharge concerns.
They conducted medication reconciliation at discharge, provided clear instructions, and offered affordable medication options or assistance programs for low-income patients.
The hospital reported a 25% reduction in 30-day readmission rates for heart failure patients and improved patient satisfaction scores related to post-discharge care.



















