Hospitals are often characterized as bureaucracies due to their complex organizational structures, standardized procedures, and hierarchical decision-making processes. Rooted in Max Weber's theory of bureaucratic management, these institutions prioritize efficiency, predictability, and accountability through formalized rules and divisions of labor. While this framework ensures consistency in patient care, adherence to regulations, and clear lines of authority, it can also lead to rigidity, slow decision-making, and depersonalized interactions. Critics argue that excessive bureaucracy may hinder adaptability, stifle innovation, and prioritize administrative tasks over patient-centered care. Thus, the question of whether a hospital is inherently a bureaucracy invites examination of its benefits in maintaining order and its potential drawbacks in delivering compassionate, flexible healthcare.
| Characteristics | Values |
|---|---|
| Hierarchical Structure | Hospitals typically have a clear chain of command, with roles ranging from administrative staff to medical directors and department heads. |
| Division of Labor | Tasks are specialized, with different departments (e.g., nursing, radiology, administration) focusing on specific functions. |
| Formal Rules and Procedures | Hospitals operate under strict protocols, guidelines, and regulatory standards to ensure patient safety and quality care. |
| Impersonality | Interactions are often rule-based rather than personal, emphasizing efficiency and consistency in service delivery. |
| Written Communication | Extensive documentation is used for patient records, policies, and administrative processes. |
| Professionalism | Employees are required to meet specific qualifications and certifications, ensuring expertise in their roles. |
| Goal-Oriented | The primary focus is on patient care, recovery, and operational efficiency, aligning with organizational objectives. |
| Predictability | Standardized procedures and schedules aim to create a predictable environment for patient treatment and staff workflows. |
| Centralized Decision-Making | Key decisions are often made by top-level management or committees, though some autonomy exists at lower levels. |
| Accountability | Clear lines of responsibility ensure that staff and departments are held accountable for their actions and outcomes. |
Explore related products


$34.48 $105




What You'll Learn
- Hierarchical Structure: Hospitals have clear chains of command, from administrators to nurses
- Rules and Procedures: Strict protocols govern patient care, staff conduct, and operations
- Specialization Roles: Departments and staff have specific, defined responsibilities
- Impersonal Interactions: Bureaucratic systems prioritize efficiency over personalized patient experiences
- Accountability Mechanisms: Hospitals use audits, reviews, and reporting to ensure compliance
![]()
Hierarchical Structure: Hospitals have clear chains of command, from administrators to nurses
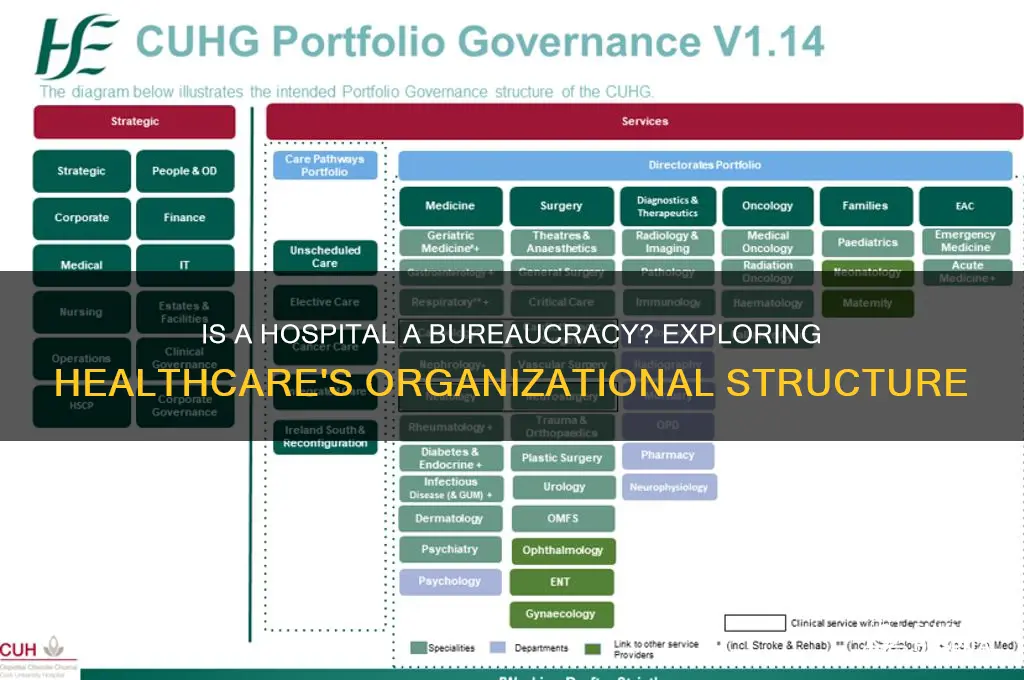
Hospitals operate within a hierarchical structure that mirrors bureaucratic systems, ensuring accountability and efficiency in patient care. At the apex are administrators—CEOs, CFOs, and medical directors—who oversee strategic decisions, resource allocation, and compliance with regulations. Below them, department heads manage specialized units like surgery, pediatrics, or emergency care, translating organizational goals into actionable plans. Nurses, often the most visible caregivers, form the operational backbone, executing treatment plans under the supervision of physicians. This tiered system creates a clear chain of command, minimizing ambiguity and ensuring that responsibilities are well-defined. For instance, a nurse administers medication (e.g., 5 mg of intravenous morphine for pain management in adults) only after a physician’s order, illustrating how hierarchy safeguards patient safety through structured protocols.
Consider the workflow during a medical emergency, such as a code blue. The hierarchical structure becomes a lifeline. The attending physician leads, making critical decisions like whether to administer 1 mg of epinephrine for cardiac arrest. Nurses follow directives, preparing medications and monitoring vital signs, while technicians handle equipment. This division of roles, rooted in the hospital’s hierarchy, prevents chaos and ensures timely interventions. Without such a structure, overlapping responsibilities could lead to errors—a risk no hospital can afford. Thus, the hierarchy isn’t merely administrative; it’s a functional necessity for high-stakes environments.
Critics argue that rigid hierarchies can stifle innovation and delay decision-making. For example, a nurse noticing a patient’s deteriorating condition might need to escalate concerns through multiple layers before action is taken. However, this system also acts as a safeguard. Before a 10-year-old receives a high-risk procedure, multiple levels of approval—from the pediatrician to the ethics committee—ensure it’s medically justified. This balance between efficiency and caution highlights the hierarchy’s dual role: it can be both a barrier and a protector, depending on the context. Hospitals must continually refine their structures to prioritize patient outcomes over procedural rigidity.
To navigate this hierarchy effectively, patients and families should understand key roles. Administrators handle billing and policy concerns, while nurses are the first point of contact for immediate needs. For instance, if a patient requires a dosage adjustment—say, reducing an antibiotic from 500 mg to 250 mg due to side effects—the nurse communicates this to the physician, who then updates the order. Knowing this flow empowers patients to direct queries appropriately, reducing frustration and improving care coordination. Ultimately, the hospital’s hierarchy isn’t just about control—it’s a framework designed to deliver safe, systematic care in complex environments.
Eastern State Hospital in Kentucky: Location and Closure Status Update
You may want to see also
Explore related products

$19.2 $28





![]()
Rules and Procedures: Strict protocols govern patient care, staff conduct, and operations
Hospitals are quintessential examples of bureaucratic structures, where rules and procedures are the backbone of daily operations. These protocols are not mere formalities but essential safeguards designed to ensure patient safety, maintain quality care, and mitigate risks. For instance, the administration of medication follows a strict process: a physician prescribes a dosage (e.g., 500 mg of amoxicillin for a 50 kg adult), which is then verified by a pharmacist and administered by a nurse who must cross-check the patient’s ID, medication name, and dosage against the chart. Deviating from this procedure, even slightly, can lead to critical errors, such as administering the wrong drug or dosage, underscoring why these rules are non-negotiable.
Consider the triage process in an emergency department, a prime example of how procedures streamline chaos. Patients are categorized based on the severity of their condition—Level 1 for life-threatening cases, Level 5 for non-urgent issues. This system ensures that a 30-year-old with chest pain is seen before a 25-year-old with a sprained ankle. Without such protocols, care would be haphazard, potentially delaying treatment for those in critical need. These rules are not arbitrary; they are evidence-based and continually refined to optimize outcomes, reflecting the hospital’s bureaucratic commitment to efficiency and fairness.
Staff conduct is equally governed by rigid protocols, from infection control measures to communication standards. For example, hand hygiene compliance is monitored through audits, with staff required to sanitize hands before and after every patient interaction. Failure to adhere can result in disciplinary action, as breaches can lead to hospital-acquired infections, which affect 1 in 25 patients daily in the U.S. alone. Similarly, the SBAR (Situation, Background, Assessment, Recommendation) communication tool is mandated for handoffs to ensure clarity and reduce errors. These rules may seem restrictive, but they foster accountability and consistency in a high-stakes environment.
Critics argue that such bureaucracy can stifle flexibility and human judgment, but the alternative—unstructured decision-making—poses greater risks. For instance, allowing nurses to deviate from medication protocols based on personal judgment could lead to overdoses or adverse reactions. Hospitals balance this tension by embedding discretion within boundaries, such as allowing physicians to override standard dosing for pediatric patients (e.g., adjusting amoxicillin dosage to 10 mg/kg for a child) but requiring documentation and peer review. This hybrid approach ensures that rules serve as guardrails, not straitjackets.
Ultimately, the bureaucratic nature of hospitals is not a flaw but a feature. Rules and procedures are the invisible scaffolding that supports the complex machinery of healthcare delivery. They transform individual efforts into coordinated action, ensuring that a 70-year-old undergoing surgery receives the same standard of care as a newborn in the NICU. While these protocols may seem onerous, they are the price of reliability in an industry where mistakes can be fatal. In hospitals, bureaucracy is not red tape—it’s a lifeline.
Volunteering at Hospitals: A Step-by-Step Guide to Making a Difference
You may want to see also
Explore related products






![]()
Specialization Roles: Departments and staff have specific, defined responsibilities
Hospitals embody bureaucratic structures through their reliance on specialization, a principle that divides complex tasks into manageable, defined roles. This division is evident in the myriad departments—emergency, radiology, pediatrics, and more—each with distinct responsibilities. For instance, the emergency department focuses on immediate, life-saving interventions, while radiology specializes in diagnostic imaging. This segmentation ensures that staff, from nurses to technicians, are trained to handle specific tasks efficiently, minimizing errors and maximizing productivity. Without such specialization, hospitals would struggle to deliver timely, high-quality care in the face of diverse patient needs.
Consider the role of a pharmacist in a hospital setting. Their specialization lies in medication management, including dosage calculations, drug interactions, and patient education. For example, a pharmacist must ensure that a 70-year-old patient with renal impairment receives a reduced dose of a particular antibiotic to avoid toxicity. This precision is only possible because the pharmacist’s role is narrowly defined, allowing them to focus on pharmacological expertise rather than general patient care. Such specialization not only enhances safety but also streamlines workflows, as other staff members can rely on the pharmacist’s expertise without duplicating efforts.
However, specialization is not without its challenges. While it fosters efficiency, it can also create silos, where departments operate in isolation, hindering collaboration. For instance, a surgeon may focus solely on the operative procedure, leaving post-operative care coordination to others. This division can lead to gaps in patient care if communication breaks down. Hospitals mitigate this risk through protocols like multidisciplinary rounds, where specialists from various departments collaborate to develop comprehensive care plans. These practices ensure that specialization enhances, rather than fragments, the overall care delivery system.
To implement effective specialization, hospitals must invest in training and clear role definitions. For example, a nurse in the intensive care unit (ICU) undergoes specialized training in critical care, enabling them to manage ventilators and administer high-risk medications like heparin drips. Similarly, a physical therapist focuses on mobility and rehabilitation, using evidence-based techniques to aid recovery. By delineating these roles, hospitals ensure that each staff member operates within their expertise, reducing the likelihood of errors and improving outcomes. This structured approach is a hallmark of bureaucratic efficiency in healthcare.
Ultimately, specialization in hospitals is a double-edged sword—it drives precision and efficiency but requires careful management to avoid fragmentation. Practical tips for optimizing this structure include fostering interdepartmental communication, providing ongoing training, and using technology to integrate workflows. For instance, electronic health records (EHRs) can bridge gaps by ensuring all specialists access the same patient data. By balancing specialization with collaboration, hospitals can harness the strengths of bureaucracy to deliver cohesive, patient-centered care. This delicate equilibrium is what makes specialization a cornerstone of modern healthcare systems.
Philippine Private Hospitals: How Many Exist Today?
You may want to see also
Explore related products






![]()
Impersonal Interactions: Bureaucratic systems prioritize efficiency over personalized patient experiences
Hospitals, by their very nature, are complex organisms designed to treat a vast array of medical conditions efficiently. This efficiency, however, often comes at the cost of personalized patient experiences. Bureaucratic systems, with their rigid protocols and standardized procedures, prioritize streamlining processes over individual needs.
A patient's journey through a hospital is a choreographed dance dictated by these systems. From intake forms and triage protocols to discharge instructions, every step is designed to maximize throughput and minimize errors. While this standardization is crucial for safety and consistency, it can lead to a sense of detachment for patients.
Imagine an elderly patient, recently diagnosed with a chronic illness, navigating this labyrinthine system. They are shuffled from department to department, interacting with a revolving door of healthcare professionals, each focused on their specific task. The warmth of a familiar face or the comfort of a personalized explanation often gets lost in the shuffle. This impersonal nature of bureaucratic healthcare can exacerbate anxiety and hinder the healing process, particularly for vulnerable populations.
Consider the following scenario: a young mother brings her child to the emergency room with a high fever. The triage nurse, following protocol, asks a series of standardized questions, checks vital signs, and assigns a priority level. While this system ensures the most critical cases are seen first, it may leave the mother feeling dismissed, her concerns about her child's well-being reduced to a set of data points. A more personalized approach, acknowledging her fears and providing clear, empathetic explanations, could significantly improve her experience without compromising efficiency.
Balancing efficiency and personalization is a delicate tightrope walk for hospitals. Implementing strategies like dedicated patient navigators, who guide individuals through the system and act as a consistent point of contact, can help bridge the gap. Additionally, incorporating patient feedback into protocol design and encouraging healthcare professionals to prioritize empathetic communication can foster a more human-centered approach within the bureaucratic framework.
Ultimately, recognizing the inherent tension between efficiency and personalization is crucial. Hospitals must strive to create systems that are both streamlined and compassionate, ensuring that patients feel seen, heard, and valued throughout their healthcare journey. This requires a conscious effort to humanize the bureaucratic process, acknowledging that behind every chart and diagnosis is a unique individual deserving of dignity and respect.
Crafting Effective Hospital Press Releases: Essential Tips and Best Practices
You may want to see also
Explore related products






![]()
Accountability Mechanisms: Hospitals use audits, reviews, and reporting to ensure compliance
Hospitals, often characterized as bureaucracies due to their hierarchical structures and standardized procedures, rely heavily on accountability mechanisms to ensure compliance with regulations, maintain quality care, and mitigate risks. Audits, reviews, and reporting are the backbone of these mechanisms, serving as systematic tools to evaluate performance, identify gaps, and drive improvement. For instance, a financial audit might uncover discrepancies in billing practices, while a clinical review could highlight deviations from evidence-based protocols. These processes are not merely administrative formalities but critical safeguards that protect patients, staff, and the institution itself.
Consider the role of audits in hospitals. These are structured evaluations, often conducted by internal or external teams, to assess adherence to policies, financial integrity, and operational efficiency. For example, a medication audit in a pediatric ward might focus on the accuracy of dosing for children under 12, ensuring that prescriptions align with weight-based guidelines (e.g., 5–10 mg/kg for certain antibiotics). Such audits not only prevent errors but also provide actionable data for training and policy updates. The key is to treat audits not as punitive measures but as opportunities for learning and refinement, fostering a culture of continuous improvement.
Reviews, on the other hand, are more focused and often peer-driven. Mortality and morbidity reviews, for instance, are regular meetings where clinicians discuss adverse outcomes to identify systemic issues. These sessions are not about assigning blame but about understanding root causes—whether it’s a communication breakdown, resource shortage, or procedural flaw. A well-structured review process includes clear documentation, multidisciplinary participation, and follow-up actions. For example, a review might reveal that delays in stroke treatment stem from unclear triage protocols, prompting the hospital to implement a color-coded system for rapid response.
Reporting complements audits and reviews by providing real-time data and transparency. Hospitals use dashboards, incident reports, and performance metrics to track key indicators such as infection rates, readmission rates, and patient satisfaction scores. For instance, a hospital might mandate that all medication errors be reported within 24 hours, regardless of severity, to analyze trends and implement preventive measures. Effective reporting systems are user-friendly, confidential, and integrated into daily workflows to encourage participation. However, they must also balance detail with practicality—overburdening staff with excessive documentation can undermine the very accountability they aim to achieve.
In conclusion, accountability mechanisms in hospitals are not just bureaucratic red tape but essential frameworks for ensuring safety, quality, and compliance. Audits, reviews, and reporting work in tandem to identify risks, address shortcomings, and promote best practices. By embedding these mechanisms into the organizational culture, hospitals can navigate the complexities of modern healthcare while upholding their core mission: delivering patient-centered care. The challenge lies in implementing these tools thoughtfully, ensuring they empower rather than overwhelm, and adapting them to the dynamic needs of healthcare delivery.
Navigating to Greenville Memorial Hospital from Due West
You may want to see also
Frequently asked questions
Yes, a hospital is often considered a bureaucracy due to its hierarchical structure, formalized rules, and standardized procedures designed to manage complex operations and ensure patient safety.
Hospitals adopt bureaucratic structures to maintain efficiency, consistency, and accountability in delivering healthcare services, especially in high-stakes environments where errors can have serious consequences.
While bureaucracy ensures standardization and safety, it can sometimes lead to delays, rigid decision-making, and reduced flexibility, potentially impacting the speed and personalization of patient care.