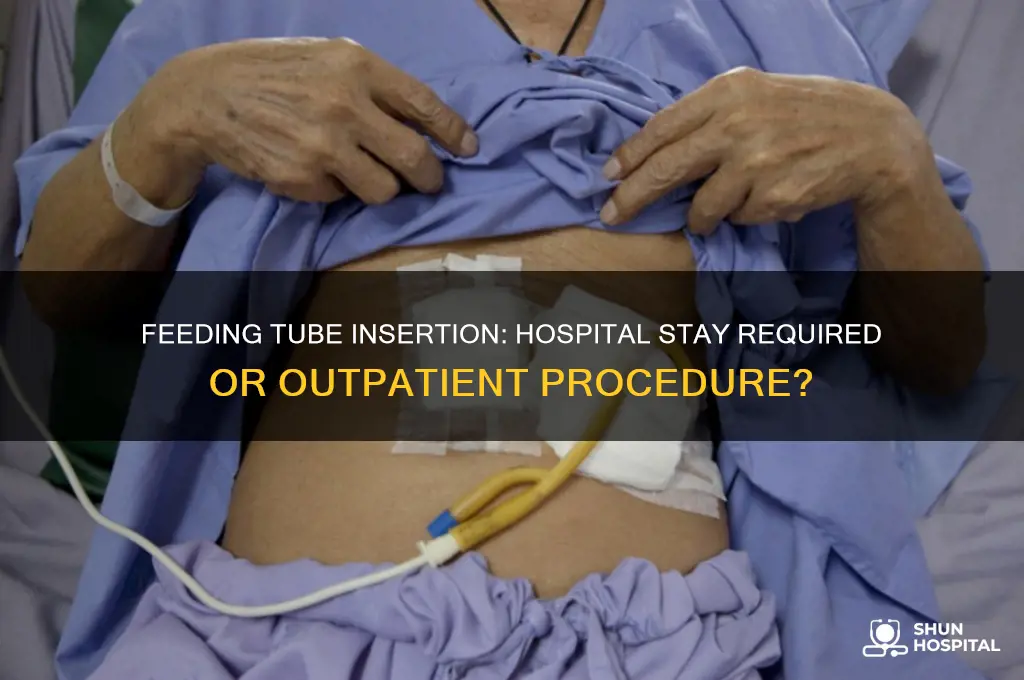
Feeding tube insertion is a common medical procedure used to provide nutrition to patients who cannot eat or drink adequately by mouth. While it is often performed as an outpatient procedure, the necessity of a hospital stay depends on various factors, including the patient's overall health, the type of feeding tube being inserted, and the presence of any underlying medical conditions. For many individuals, feeding tube insertion can be safely conducted in an ambulatory setting, allowing them to return home the same day. However, certain cases, such as those involving complex medical histories or the need for general anesthesia, may require a short hospital stay to ensure proper monitoring and management of potential complications. Ultimately, the decision is made on a case-by-case basis, balancing patient safety with convenience and healthcare resource utilization.
| Characteristics | Values |
|---|---|
| Necessity of Hospital Stay | Not always necessary; depends on patient condition and tube type. |
| Outpatient Procedures | Possible for some cases, especially with nasogastric or PEG tubes. |
| Inpatient Procedures | Common for complex cases, high-risk patients, or surgically placed tubes. |
| Procedure Duration | Typically 15–30 minutes for PEG; longer for surgical placements. |
| Anesthesia Required | Local anesthesia for PEG; general anesthesia for surgical tubes. |
| Recovery Time | Minimal for outpatient; 1–2 days for inpatient procedures. |
| Common Tube Types | Nasogastric (NG), PEG (percutaneous endoscopic gastrostomy), JEJ. |
| Patient Eligibility for Outpatient | Stable health, no severe comorbidities, cooperative patients. |
| Risks of Outpatient Procedure | Lower infection risk, reduced healthcare costs, quicker recovery. |
| Risks of Inpatient Procedure | Higher costs, potential hospital-acquired infections. |
| Post-Procedure Monitoring | Outpatient: follow-up within 24–48 hours; inpatient: immediate monitoring. |
| Insurance Coverage | Varies; outpatient often covered but depends on policy and necessity. |
| Latest Trends | Increasing preference for outpatient procedures due to safety and cost-effectiveness. |
Explore related products






What You'll Learn
![]()
Outpatient vs. inpatient procedures
Feeding tube insertion is a common procedure that can be performed either as an outpatient or inpatient procedure, depending on various factors such as the patient's medical condition, age, and the type of feeding tube being inserted. Outpatient procedures are typically performed in a clinic or ambulatory surgery center, allowing patients to return home the same day. In contrast, inpatient procedures require a hospital stay, which can range from one night to several days. When considering whether a hospital stay is necessary for feeding tube insertion, it's essential to weigh the benefits and drawbacks of both outpatient and inpatient procedures.
Outpatient feeding tube insertion procedures are generally preferred for patients who are otherwise healthy and do not have complex medical conditions. These procedures are often performed under local anesthesia or mild sedation, and patients can usually resume their normal activities within a short period. The advantages of outpatient procedures include reduced costs, less disruption to daily life, and a lower risk of hospital-acquired infections. However, outpatient procedures may not be suitable for patients with certain medical conditions, such as severe gastrointestinal disorders or bleeding disorders, which may require closer monitoring and management in a hospital setting.
Inpatient feeding tube insertion procedures, on the other hand, are typically reserved for patients with more complex medical needs or those who require closer monitoring during and after the procedure. This may include patients with severe malnutrition, gastrointestinal bleeding, or those who are at increased risk of complications. Inpatient procedures allow for more comprehensive monitoring, including vital signs, laboratory tests, and imaging studies, which can help identify and manage potential complications promptly. Additionally, inpatient stays provide an opportunity for healthcare professionals to educate patients and caregivers on proper feeding tube care and management, which is crucial for long-term success.
The decision to perform feeding tube insertion as an outpatient or inpatient procedure should be made on a case-by-case basis, taking into account the patient's individual needs and medical history. Factors to consider include the patient's age, overall health status, and the presence of comorbid conditions. For example, elderly patients or those with compromised immune systems may be at increased risk of complications and may benefit from the closer monitoring provided by an inpatient stay. Similarly, patients with complex medical conditions, such as severe gastroesophageal reflux disease or motility disorders, may require more intensive management and monitoring, making an inpatient procedure more appropriate.
In some cases, the type of feeding tube being inserted may also influence the decision to perform the procedure as an outpatient or inpatient. For instance, the insertion of a percutaneous endoscopic gastrostomy (PEG) tube, which is a common type of feeding tube, can often be performed as an outpatient procedure in healthy individuals. However, the insertion of more complex tubes, such as jejunostomy tubes or those requiring fluoroscopic guidance, may be more appropriately performed as an inpatient procedure to ensure proper placement and management of potential complications. Ultimately, the choice between outpatient and inpatient feeding tube insertion should be guided by the patient's best interests, taking into account their individual needs, preferences, and medical condition.
In conclusion, the decision to perform feeding tube insertion as an outpatient or inpatient procedure depends on a variety of factors, including the patient's medical condition, age, and the type of feeding tube being inserted. While outpatient procedures offer several advantages, including reduced costs and less disruption to daily life, inpatient procedures provide closer monitoring and management, which may be necessary for patients with complex medical needs. Healthcare professionals should carefully evaluate each patient's individual circumstances to determine the most appropriate setting for feeding tube insertion, ensuring the best possible outcomes and quality of care. By weighing the benefits and drawbacks of both outpatient and inpatient procedures, patients and their caregivers can make informed decisions about the most suitable approach for their specific situation.
Leaving the Hospital: Wheelchair Requirement or Personal Choice?
You may want to see also
Explore related products






![]()
Risks and complications of insertion
Feeding tube insertion, while generally safe, carries potential risks and complications that vary depending on the type of tube (nasogastric, gastrostomy, or jejunostomy) and the method of insertion (surgical or percutaneous endoscopic gastrostomy, PEG). Understanding these risks is crucial in determining whether a hospital stay is necessary to manage potential complications effectively. One of the most common risks is infection at the insertion site, particularly with gastrostomy tubes. Infections can range from mild skin irritation to more severe conditions like peritonitis, which requires immediate medical attention. Hospital monitoring allows for prompt administration of antibiotics and wound care, reducing the risk of complications.
Another significant risk is tube displacement or dislodgement, which can occur if the tube is not secured properly or if the patient moves excessively. This complication is more likely with nasogastric tubes but can also happen with gastrostomy tubes. If the tube is dislodged, it may need to be reinserted, and complications such as bleeding or perforation can arise. A hospital stay ensures that healthcare providers can quickly address displacement and minimize associated risks. Additionally, bleeding during or after insertion is a potential complication, particularly with surgical or PEG procedures. While minor bleeding is common, excessive bleeding may require intervention, including blood transfusions or surgical repair, which are best managed in a hospital setting.
Perforation of the stomach, intestines, or other organs is a rare but serious risk of feeding tube insertion. This complication can lead to life-threatening conditions such as peritonitis or sepsis if not treated immediately. Symptoms like severe abdominal pain, fever, or signs of shock require urgent medical attention, making a hospital stay essential for high-risk patients or those with complex medical histories. Aspiration pneumonia is another risk, particularly with nasogastric tubes, where food or fluids enter the lungs instead of the stomach. This complication is more likely in patients with swallowing difficulties or reduced consciousness, and hospital monitoring allows for early detection and treatment with suctioning or antibiotics.
Finally, long-term complications such as tube site granulomas, skin breakdown, or gastrointestinal issues like diarrhea, constipation, or reflux can arise. While these complications may not require immediate hospitalization, ongoing medical supervision is often necessary to manage symptoms and adjust tube care. For patients at higher risk of complications due to age, underlying health conditions, or the complexity of the procedure, a hospital stay provides the necessary support and resources to address these issues promptly. In conclusion, while feeding tube insertion is often performed on an outpatient basis, certain risks and complications underscore the need for a hospital stay, particularly for vulnerable populations or when complications arise.
Your Health, Your Choice: No Consent, No Debt
You may want to see also
Explore related products






![]()
Patient eligibility criteria
Feeding tube insertion is a procedure that can be performed in various settings, including hospitals, outpatient clinics, and even at home, depending on the patient's condition and the type of feeding tube required. However, determining whether a hospital stay is necessary for feeding tube insertion hinges on specific patient eligibility criteria. These criteria ensure the procedure is safe, effective, and appropriate for the patient's medical needs.
Medical Stability and Underlying Conditions are primary factors in assessing patient eligibility. Patients who are hemodynamically stable, with well-controlled chronic conditions, are often candidates for outpatient feeding tube insertion. For instance, individuals with dysphagia due to stroke or neurological disorders may not require hospitalization if their vital signs are stable and they have no acute complications. Conversely, patients with severe malnutrition, uncontrolled infections, or significant respiratory issues may need a hospital stay to optimize their condition before and after the procedure.
Type of Feeding Tube and Complexity of Insertion also play a critical role in eligibility. Nasogastric or nasojejunal tubes, which are less invasive, can often be placed in an outpatient setting if the patient tolerates the procedure well. However, more complex procedures, such as percutaneous endoscopic gastrostomy (PEG) or jejunostomy tubes, may require hospitalization, especially if the patient has anatomical abnormalities or a high risk of complications. Patients with a history of abdominal surgeries or severe gastrointestinal disorders may need closer monitoring in a hospital setting.
Patient and Caregiver Capabilities are another essential consideration. Outpatient feeding tube insertion is more feasible if the patient and their caregivers are capable of managing post-procedure care, including tube maintenance, feeding, and monitoring for complications. Patients with limited support systems or cognitive impairments may require hospitalization to ensure proper education and initial management. Additionally, patients at risk of aspiration or those needing immediate access to medical intervention in case of complications are better suited for a hospital stay.
Age and Comorbidities further influence eligibility. Pediatric patients or elderly individuals with multiple comorbidities may require hospitalization due to their increased vulnerability to procedural risks and complications. For example, elderly patients with frailty or dementia may need a controlled hospital environment to ensure safety and adequate recovery. Conversely, younger, healthier patients with straightforward cases may be eligible for outpatient insertion.
In summary, patient eligibility criteria for feeding tube insertion without a hospital stay include medical stability, the type and complexity of the procedure, patient and caregiver capabilities, and age-related factors. A thorough assessment by a healthcare provider is essential to determine the most appropriate setting for the procedure, balancing safety, efficacy, and patient convenience.
Top Heart Hospitals Accepting Humana Insurance: Your Comprehensive Guide
You may want to see also
Explore related products

![[2 Pack] Feeding Tube Belt, PEG Tube Holder G-Tube Abdominal Belt Breathable Black with Slit for G Tube J Tube PEG Tube Supplies, No More Taping The Tube](https://m.media-amazon.com/images/I/71CWOwLm1-L._AC_UL320_.jpg)



![]()
Recovery time and care needs
For gastrostomy or jejunostomy tubes, which are surgically placed through the abdomen, recovery time is longer. Patients may require a hospital stay of 1 to 2 days for monitoring, especially if the procedure is done surgically or endoscopically. After discharge, recovery at home typically takes 1 to 2 weeks. During this period, patients should avoid strenuous activities, heavy lifting, or anything that puts pressure on the abdomen to prevent dislodging the tube or causing complications. Pain management with over-the-counter medications may be necessary, and the insertion site must be kept clean and dry to prevent infection.
Care needs for gastrostomy or jejunostomy tubes are more involved. The insertion site must be monitored daily for redness, swelling, discharge, or signs of infection. Dressings may need to be changed regularly, and the tube should be flushed with water before and after feedings to prevent clogging. Patients or caregivers must also learn how to administer tube feedings correctly, including preparing formula, using feeding pumps (if applicable), and recognizing signs of intolerance such as nausea, vomiting, or abdominal pain.
Nutritional monitoring is another critical aspect of post-insertion care. Patients may need to work with a dietitian to ensure they are receiving adequate calories, fluids, and nutrients through the feeding tube. Adjustments to the feeding schedule or formula may be required based on tolerance and nutritional needs. Regular follow-up appointments with a healthcare provider are essential to assess tube placement, address any complications, and ensure the patient is adapting well to tube feeding.
Finally, emotional and psychological support is an often-overlooked aspect of recovery. Adjusting to life with a feeding tube can be challenging, and patients may experience anxiety, frustration, or grief. Caregivers and family members should provide encouragement and assistance, and patients may benefit from joining support groups or speaking with a counselor. With proper care and attention to recovery guidelines, most individuals can adapt to feeding tube use and maintain a good quality of life.
South Shore Hospital: A Teaching Facility?
You may want to see also
Explore related products






![]()
Cost and insurance coverage differences
The necessity of a hospital stay for feeding tube insertion can significantly impact the overall cost and insurance coverage. In many cases, feeding tube insertion can be performed as an outpatient procedure, meaning the patient does not need to be admitted to the hospital. This is often the case for simpler procedures, such as the placement of a nasogastric (NG) tube or a percutaneous endoscopic gastrostomy (PEG) tube, which can be done in a doctor's office, endoscopy center, or outpatient surgery center. Outpatient procedures generally cost less than inpatient procedures because they do not involve hospital room charges, extended monitoring, or additional hospital services.
When feeding tube insertion is performed as an outpatient procedure, the cost is typically lower, ranging from $500 to $2,000, depending on the type of tube, the complexity of the procedure, and the geographic location. Insurance plans often cover a significant portion of this cost, especially if the procedure is deemed medically necessary. Most private insurance plans, Medicare, and Medicaid cover feeding tube insertion when it is prescribed by a physician and supported by medical documentation. However, patients should verify their coverage with their insurance provider, as some plans may require pre-authorization or have specific criteria for coverage.
In contrast, if a hospital stay is necessary for feeding tube insertion, the cost can increase substantially. Hospital stays involve additional expenses, including room charges, nursing care, diagnostic tests, and other hospital services. The total cost for an inpatient feeding tube insertion can range from $5,000 to $15,000 or more, depending on the length of stay and any complications that arise. Insurance coverage for inpatient procedures is generally more comprehensive, but patients may still be responsible for deductibles, copayments, or coinsurance. Medicare and Medicaid typically cover inpatient feeding tube insertion if it is deemed medically necessary, but private insurance plans may have stricter criteria or require pre-authorization.
Insurance coverage differences also depend on whether the feeding tube insertion is considered a short-term or long-term solution. For example, temporary feeding tubes (e.g., NG tubes) may be covered differently than permanent or long-term tubes (e.g., PEG tubes or jejunostomy tubes). Some insurance plans may cover the initial insertion but require additional documentation or justification for ongoing supplies or replacements. Patients with long-term feeding tubes may also need coverage for related supplies, such as feeding formulas, tubing, and syringes, which can add to the overall cost.
Lastly, the choice of healthcare facility can influence both cost and insurance coverage. Outpatient procedures performed in a doctor's office or endoscopy center are often less expensive than those done in a hospital outpatient department. However, insurance plans may have different reimbursement rates for different types of facilities, which can affect the patient's out-of-pocket costs. Patients should compare costs and coverage at various facilities and choose one that is both cost-effective and within their insurance network to minimize unexpected expenses. Always consult with both the healthcare provider and insurance company to understand the full financial implications of feeding tube insertion.
Top Heart Doctors: Where to Find the Best Care
You may want to see also
Frequently asked questions
Not always. Depending on the type of feeding tube and the patient's health condition, some procedures can be done on an outpatient basis, while others may require a short hospital stay for monitoring.
Factors include the patient's overall health, the type of feeding tube (e.g., nasogastric, PEG), the complexity of the procedure, and the need for post-procedure monitoring or pain management.
Yes, some simpler procedures, like nasogastric tube insertion, can be done in a clinic or doctor’s office. However, more invasive procedures, such as PEG tube placement, often require a hospital setting.































