Acute kidney injury (AKI) is a common complication in hospitalized patients, affecting approximately 10% of patients. AKI is a sudden episode of kidney failure or damage that can happen within a few hours or days. It is often caused by reduced blood flow to the kidneys, usually in patients who are already unwell with other health conditions. AKI is associated with high inpatient mortality, with an overall incidence rate of 2% to 5% in hospitalized patients and up to 67% in intensive care units. Studies have shown that hospital-acquired AKI is associated with increased mortality but not increased readmission rates. Therefore, it is essential to differentiate between AKI and chronic kidney disease (CKD) to effectively treat AKI and improve patient outcomes.
| Characteristics | Values |
|---|---|
| Incidence | 2.2% of all hospital admissions in the UK |
| 1% of all hospital admissions in the US | |
| 2% to 5% during hospitalization in the US | |
| 67% of patients admitted to the intensive care unit in the US | |
| 34% die in the hospital | |
| 42% are dead at 90 days post-discharge | |
| 48% are dead 1 year post-discharge | |
| 40% to 50% in-hospital mortality rate | |
| 50%+ mortality rate for ICU patients | |
| Occurrence | Common complication in hospitalized patients |
| Occurs in non-critically ill patients | |
| Occurs in critically ill patients | |
| Occurs in non-critical medical patients | |
| Occurs in adult patients | |
| Occurs in male patients |
Explore related products






What You'll Learn
- AKI is a common complication in hospitalised patients
- AKI is associated with high inpatient mortality
- AKI is an important contributor to extended hospital stays
- AKI is a frequent complication of acute illnesses requiring hospitalisation
- AKI is a common complication following diagnostic and therapeutic procedures
![]()
AKI is a common complication in hospitalised patients
Acute Kidney Injury (AKI) is a common complication in hospitalised patients. It is a serious disease, previously termed "acute renal failure" (ARF). AKI is associated with a high risk of mortality and other short- and long-term adverse outcomes. The in-hospital mortality rate for AKI is 40% to 50%, and the mortality rate for ICU patients is more than 50%. In patients who sustain in-hospital AKI, 34% die in the hospital, 42% are dead at 90 days, and 48% at one year post-discharge, compared to 12% one-year mortality in patients without AKI. AKI is also associated with less favourable outcomes in non-critical patients.
The overall incidence of AKI is 2.2%. However, in the United States, the incidence rate of acute kidney injury during hospitalisation is 2% to 5%, and it occurs in up to 67% of patients admitted to the intensive care unit. AKI is thus a significant contributor to extended hospital stays and patient morbidity. It is also expensive to manage.
AKI is often a complication of another serious illness and is usually seen in older people who are unwell with other conditions. Most cases of AKI are caused by reduced blood flow to the kidneys. Certain medications, such as non-steroidal anti-inflammatory drugs (NSAIDs), blood pressure medicines, and antibiotics, can also increase the risk of AKI.
It is important to differentiate between AKI and chronic kidney disease (CKD), as CKD is a risk factor for AKI. A history of CKD can include symptoms such as chronic fatigue, anorexia, nocturia, and a disturbed sleep-wake cycle. Early detection and treatment of AKI are essential to prevent abnormal levels of salts and chemicals from building up in the body, which can affect the ability of other organs to function properly.
Lenox Hill Hospital: Private or Public?
You may want to see also
Explore related products






![]()
AKI is associated with high inpatient mortality
Acute Kidney Injury (AKI) is a common complication in hospitalised patients. It is a major global public health problem, affecting approximately 10% of patients. AKI is a frequent complication of acute illnesses requiring hospitalisation. It is also expensive to manage and is associated with a high rate of prolonged hospitalisation and inpatient mortality.
Several studies have confirmed the high prevalence of AKI and its associated high mortality rate. In one study, the overall incidence of AKI was 2.2%, with 34% of patients with in-hospital AKI dying in the hospital, 42% dying within 90 days, and 48% dying within a year of discharge. The in-hospital mortality rate is reported at 24% and increases with the severity of the disease. The risk of dying increases with the severity of AKI in the hospital, within the first 90 days, and after 90 days of discharge.
The high mortality rate associated with AKI may be due to the interaction between AKI and illness severity. Studies have consistently observed that AKI is associated with higher illness severity, as quantified by scores such as the Acute Physiology and Chronic Health Evaluation (APACHE) or the Simplified Acute Physiology Score (SAPS) II. However, after multivariate analysis to correct for this, the relationship between AKI and mortality persisted and was consistently greater than the association between illness severity and mortality.
Early identification and treatment of AKI are essential to improving patient outcomes. According to a report by the United Kingdom National Institute for Health and Care Excellence (UK-NICE), early identification and treatment of AKI, with a focus on hydration and medications, could prevent up to 42,000 deaths from AKI each year. Additionally, AKI care bundles have been shown to reduce the risk of death and progression of AKI.
While most people with AKI make a full recovery, some go on to develop chronic kidney disease or long-term kidney failure. In severe cases, dialysis may be necessary to filter harmful waste, extra salt, and water from the blood.
Hospitals' Emergency Care: Rights and Responsibilities
You may want to see also
Explore related products






![]()
AKI is an important contributor to extended hospital stays
Acute kidney injury (AKI) is a common complication in hospitalized patients. AKI is seen in 1% of all hospital admissions, and its incidence rate during hospitalization is 2% to 5%. It occurs in up to 67% of patients admitted to the intensive care unit (ICU). AKI is a significant contributor to extended hospital stays and increased healthcare costs. It is associated with a higher risk of mortality and morbidity, with an in-hospital mortality rate of 30-50% when dialysis is required.
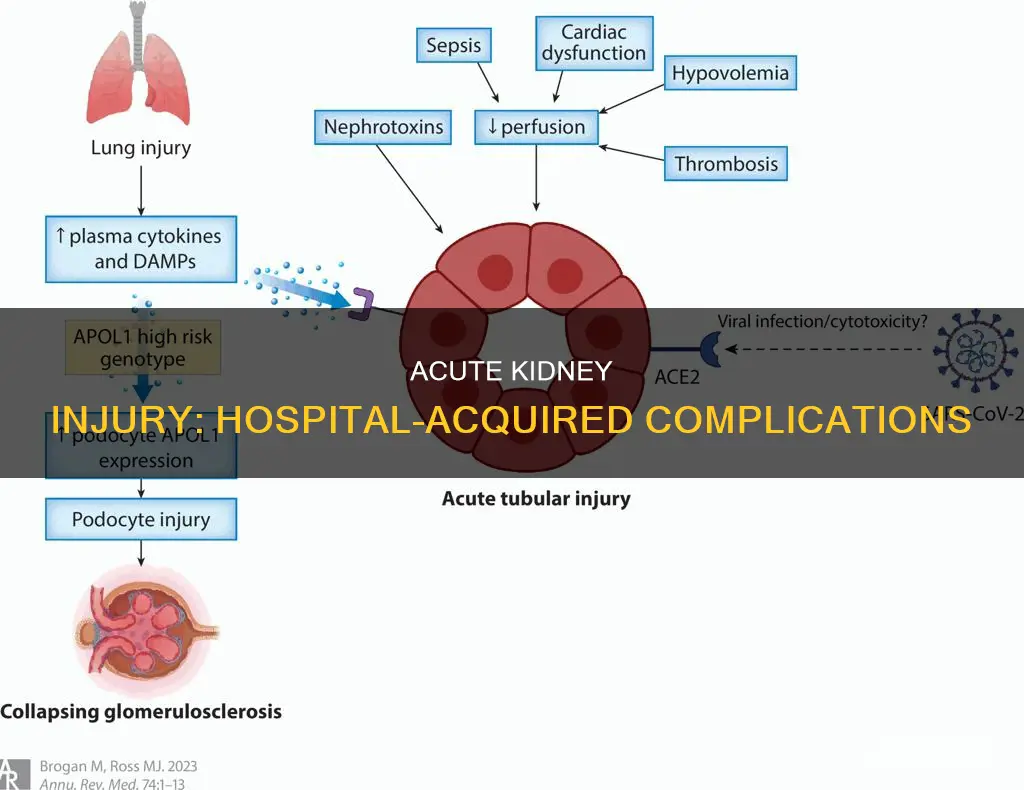
The pathogenesis of AKI is driven by its underlying etiology, which can be categorized as prerenal, intrarenal, or postrenal. Prerenal AKI is caused by reduced blood flow to the kidneys, which can be due to hypovolemia, hypotension, or certain medications. Intrarenal AKI involves direct kidney damage, such as acute tubular necrosis, which can be caused by ischemia or toxins. Postrenal AKI refers to obstructions that prevent the normal flow of urine, such as acute urinary tract obstruction or acute glomerulonephritis.
The evaluation of AKI should include a comprehensive metabolic panel and a detailed physical examination. Urine studies, including electrolytes, protein, osmolality, and albumin-to-creatinine ratios, can provide valuable information about the etiology of AKI. A history of urine output and orthostatic vital signs are also important considerations.
The management of AKI in hospitalized patients focuses on adjusting medication doses, avoiding nephrotoxic drugs, and addressing fluid balance through appropriate fluid challenges or diuretics. Mild AKI can often be managed as an outpatient, while more severe cases may require a higher level of care, such as the intensive care unit.
AKI has significant implications for patient outcomes and healthcare costs. Hospitalizations that include AKI are associated with longer lengths of stay and higher economic costs compared to hospitalizations without AKI. Early detection and intervention are crucial to achieving the best clinical outcomes for patients with AKI. Additionally, proper documentation and patient education during discharge can help prevent additional renal insults and improve long-term outcomes.
Moorfields Eye Hospital: Private or Public?
You may want to see also
Explore related products






![]()
AKI is a frequent complication of acute illnesses requiring hospitalisation
Acute kidney injury (AKI) is a frequent complication of acute illnesses requiring hospitalisation. It is a common complication in hospitalised patients, affecting approximately 10% of patients, depending on how it is measured. AKI is often associated with significant morbidity and mortality, with an in-hospital mortality rate of 40% to 50%. In the United States, 1% of all hospital admissions involve patients with AKI on admission, and the incidence rate during hospitalisation is 2% to 5%.
AKI is a serious condition where the kidneys suddenly stop working properly, ranging from minor loss of kidney function to complete kidney failure. It is usually a complication of another serious illness, often seen in older people who are already unwell with other conditions. It is important to detect AKI early and treat it promptly to prevent abnormal levels of salts and chemicals from building up in the body, which can affect the ability of other organs to function properly. If left untreated, kidney shutdown can occur, leading to death.
The pathogenesis of AKI is driven by its aetiology. The common endpoint in acute tubular necrosis is a cellular insult secondary to ischemia or direct toxins, resulting in effacement of the brush border, cell death, and decreased function of tubular cells. One intrarenal cause is intratubular obstruction by pigments, crystals, or immunoglobulin light chains. Most cases of AKI are caused by reduced blood flow to the kidneys, and certain medications, such as anti-inflammatory drugs (NSAIDs), blood pressure medicines, and antibiotics, can increase the risk of AKI.
AKI is associated with increased inpatient mortality, and patients with AKI have higher rates of preventable death compared to those without AKI. Studies have shown that 34% of patients with in-hospital AKI die during their hospital stay, with 42% dead at 90 days and 48% at one year post-discharge, compared to a 12% one-year mortality rate for patients without AKI. AKI is also associated with longer hospital stays and increased morbidity.
In summary, AKI is a frequent and serious complication of acute illnesses requiring hospitalisation. It is associated with high morbidity and mortality rates, and early detection and treatment are crucial to prevent adverse outcomes.
Bam Margera's Hospitalization: What We Know So Far
You may want to see also
Explore related products





![]()
AKI is a common complication following diagnostic and therapeutic procedures
Acute kidney injury (AKI) is a common complication following diagnostic and therapeutic procedures. It is a serious disease that affects approximately 10% of hospitalised patients, depending on how it is measured. AKI is often a complication of acute illnesses requiring hospitalisation, and it is associated with significant morbidity and mortality. The incidence rate of AKI in hospitals ranges from 2% to 5%, and it occurs in up to 67% of intensive care unit (ICU) patients.
HA-AKI, or hospital-acquired AKI, is a common complication resulting from a multitude of diagnostic and therapeutic procedures. It is associated with increased morbidity and mortality and has been proposed as a patient safety indicator. The overall incidence of AKI in hospitals is approximately 2.2%, with stage 1 accounting for 61%, stage 2 for 27%, and stage 3 for 12%. In patients who develop AKI during their hospital stay, the mortality rate is significantly higher than in those without AKI. Specifically, 34% of patients with in-hospital AKI die during their hospitalisation, 42% are dead within 90 days of discharge, and 48% are dead within one year.
AKI is a frequent complication in critical patients, leading to a worse prognosis. It is also associated with less favourable outcomes in non-critical patients. The risk of dying increases with the severity of AKI, and it is an independent factor for death when adjusted for co-morbidities. The in-hospital mortality rate for AKI is 40% to 50%, and for ICU patients, it exceeds 50%.
The common causes of AKI in hospitalised patients include oliguria, which may indicate AKI, and sudden anuria, which suggests acute urinary tract obstruction, acute glomerulonephritis, or vascular blockage. AKI is also associated with older patients who are unwell with other conditions, and it can range from minor loss of kidney function to complete kidney failure. It is essential to detect and treat AKI early to prevent the build-up of abnormal levels of salts and chemicals, which can affect the function of other organs.
Faulkner Hospital: How Far is it, Really?
You may want to see also
Frequently asked questions
AKI is where your kidneys suddenly stop working properly. It can range from minor loss of kidney function to complete kidney failure.
Acute kidney injury is a frequent complication in critical patients, affecting approximately 10% of patients. In the United States, the incidence rate of acute kidney injury in hospitals is 2% to 5%, and it occurs in up to 67% of patients admitted to the intensive care unit.
Hospital-acquired acute kidney injury is associated with increased morbidity and mortality. In-hospital mortality rates for AKI are 40% to 50%, and this risk increases with the severity of AKI. It is also linked to longer hospital stays and higher healthcare costs.































