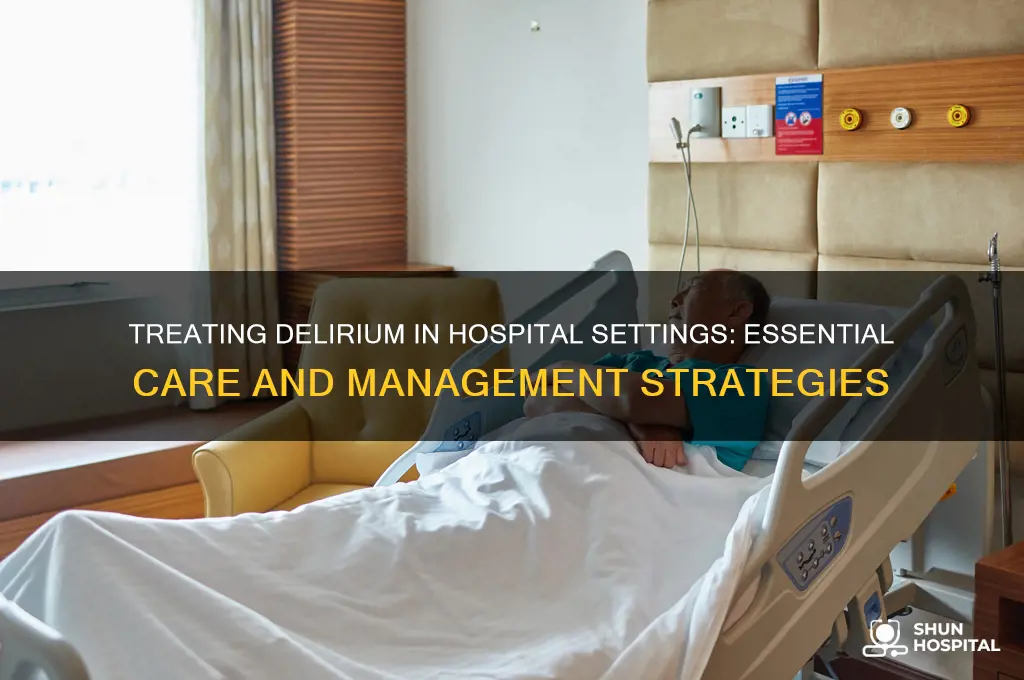
Delirium, a sudden and severe disturbance in mental abilities, is a serious condition that often requires prompt medical attention, and hospitals play a crucial role in its treatment. Given its acute nature and potential complications, delirium is frequently managed in a hospital setting where healthcare professionals can conduct comprehensive assessments, identify underlying causes, and provide immediate interventions. Treatment typically involves addressing the root cause, such as infections, medication side effects, or metabolic imbalances, while also implementing supportive care to stabilize the patient. Hospitals offer access to specialized resources, including diagnostic tools, multidisciplinary teams, and controlled environments, which are essential for effectively managing delirium and preventing long-term cognitive decline or other adverse outcomes.
| Characteristics | Values |
|---|---|
| Setting of Treatment | Hospital (inpatient) is the primary setting for delirium treatment, especially for severe cases, those with medical complications, or when safety is a concern. |
| Duration of Hospital Stay | Varies depending on severity and underlying causes; typically ranges from a few days to several weeks. |
| Multidisciplinary Approach | Involves physicians, nurses, pharmacists, physical therapists, and psychologists for comprehensive care. |
| Pharmacological Treatment | Medications like antipsychotics (e.g., haloperidol, quetiapine) may be used for severe agitation or distress, but are used cautiously due to potential side effects. |
| Non-Pharmacological Interventions | Reorientation strategies, cognitive stimulation, hydration, nutrition, pain management, and addressing underlying causes (e.g., infections, electrolyte imbalances). |
| Monitoring | Continuous monitoring for changes in mental status, vital signs, and response to treatment. |
| Family Involvement | Families are often involved in care planning, providing familiar objects, and assisting with reorientation. |
| Discharge Planning | Includes follow-up care, referrals to specialists, and strategies to prevent recurrence. |
| Prognosis | Better outcomes with early detection and treatment; hospital-based care improves recovery rates but depends on underlying health conditions. |
| Prevention Strategies | Hospitals implement protocols to prevent delirium, such as minimizing sedatives, maintaining sleep-wake cycles, and early mobility. |
Explore related products


$16.17 $29.95




What You'll Learn
![]()
Medications for Delirium Treatment
Delirium, a sudden confusion often seen in hospitalized patients, requires prompt treatment to prevent complications. While non-pharmacological approaches are first-line, medications play a crucial role in managing severe or persistent cases. The choice of medication depends on the delirium subtype (hyperactive, hypoactive, or mixed) and underlying causes.
Here’s a focused guide on medications used in hospital settings:
Antipsychotics: The Cornerstone of Treatment
Atypical antipsychotics like quetiapine (25–50 mg twice daily) and olanzapine (2.5–5 mg daily) are commonly used due to their efficacy in calming agitation and reducing psychotic features. Haloperidol (0.5–2 mg twice daily) remains an option but is less favored due to higher risks of extrapyramidal symptoms, especially in older adults. Dosages are typically lower in elderly patients to minimize side effects. These medications are often initiated in divided doses and titrated based on response, with close monitoring for adverse effects such as QT prolongation or sedation.
Benzodiazepines: For Alcohol Withdrawal or Seizure-Related Delirium
In cases where delirium is linked to alcohol withdrawal or seizures, benzodiazepines like lorazepam (0.5–2 mg every 6–8 hours) or diazepam (5–10 mg every 6–8 hours) are essential. These medications act by stabilizing GABA receptors, reducing withdrawal symptoms and preventing seizures. However, they should be avoided in patients with respiratory compromise or pre-existing cognitive impairment due to their sedative effects. Dosing is often tailored using protocols like the CIWA scale for alcohol withdrawal.
Alpha-2 Agonists: An Alternative for Agitation
Dexmedetomidine, an alpha-2 agonist, is increasingly used in intensive care units for its sedative and anti-agitative properties without respiratory depression. Administered intravenously (0.2–0.7 mcg/kg/hr), it is particularly useful in hyperactive delirium or when avoiding antipsychotics. However, it requires hemodynamic monitoring due to potential bradycardia and hypotension. This medication is not typically used long-term but rather for acute symptom control.
Practical Considerations and Cautions
Medications for delirium should be prescribed with caution, especially in older adults or those with comorbidities. Start with the lowest effective dose, reassess frequently, and discontinue as soon as symptoms resolve. Avoid polypharmacy, as it can exacerbate confusion. Always address reversible causes (e.g., infections, electrolyte imbalances) before or alongside medication use. For example, a patient with hypoactive delirium due to a urinary tract infection may require antibiotics rather than antipsychotics.
While medications are invaluable in managing delirium, they are not a standalone solution. Hospital treatment should integrate pharmacological interventions with environmental modifications, reorientation strategies, and family involvement. The goal is to use medications judiciously, prioritizing safety and minimizing duration to prevent long-term cognitive decline. In hospital settings, a multidisciplinary team approach ensures optimal care for this complex condition.
Jennifer Lopez Hospitalized: Separating Fact from Fiction in Recent Reports
You may want to see also
Explore related products






![]()
Role of Hydration and Nutrition
Dehydration and malnutrition are often overlooked yet critical contributors to delirium, particularly in hospitalized patients. Even mild dehydration, defined as a 1-2% loss of body weight, can impair cognitive function and exacerbate confusion. In older adults, who are already at higher risk for delirium due to age-related physiological changes, fluid deficits can precipitate or worsen symptoms. Hospitalized patients are especially vulnerable due to factors like reduced oral intake, diuretic use, and acute illnesses that increase fluid loss. Recognizing and addressing hydration status is therefore a cornerstone of delirium management in the hospital setting.
Nutrition plays an equally vital role, as deficiencies in key nutrients—such as vitamin B12, folate, and thiamine—can disrupt neurological function and contribute to delirium. For instance, thiamine deficiency, common in patients with alcoholism or poor dietary intake, is a well-documented cause of Wernicke-Korsakoff syndrome, which presents with confusion and memory impairment. Hospitalized patients, particularly those with acute illnesses or post-surgery, often experience decreased appetite or malabsorption, leading to rapid nutrient depletion. A proactive approach to nutritional assessment and supplementation is essential to prevent and treat delirium in this population.
Practical strategies for maintaining hydration and nutrition in hospitalized patients include regular monitoring of fluid intake and output, with a goal of 1.5 to 2 liters of fluid per day for most adults, adjusted for renal function and other comorbidities. Oral rehydration solutions can be beneficial for patients with mild to moderate dehydration, while intravenous fluids may be necessary for those unable to tolerate oral intake. Nutritional interventions should focus on high-protein, calorie-dense meals, supplemented with oral nutritional drinks if necessary. For patients at high risk, daily multivitamin supplementation, particularly with B-complex vitamins, can help prevent deficiencies.
It’s important to note that overhydration and excessive nutrient supplementation can also pose risks, particularly in patients with renal or hepatic impairment. For example, excessive fluid administration in heart failure patients can lead to volume overload, while high doses of certain vitamins, like vitamin A, can be toxic. A balanced approach, guided by regular laboratory monitoring and individualized care plans, is crucial. Collaboration between healthcare providers, including nurses, dietitians, and physicians, ensures that hydration and nutrition are optimized without causing harm.
In conclusion, addressing hydration and nutrition is a fundamental yet often underemphasized aspect of delirium treatment in the hospital. By systematically assessing and managing fluid and nutrient status, healthcare teams can significantly reduce the incidence and severity of delirium, improving patient outcomes and shortening hospital stays. This approach requires vigilance, individualized care, and interdisciplinary collaboration, but its impact on patient recovery is undeniable.
Locating the Generator in Maple Hospital: A Quick Guide
You may want to see also
Explore related products






![]()
Environmental Adjustments in Hospitals
Hospitals are increasingly recognizing the role of environmental factors in the development and management of delirium, a condition characterized by acute confusion and cognitive decline. One critical adjustment involves optimizing lighting to align with natural circadian rhythms. Patients, especially the elderly, benefit from exposure to bright, natural light during the day, which can be facilitated by large windows or full-spectrum lighting. Conversely, dim, warm lighting in the evening helps signal the body to prepare for sleep, reducing nighttime agitation. For example, a study in *JAMA Internal Medicine* found that patients in rooms with controlled lighting cycles experienced a 30% reduction in delirium incidence compared to standard lighting conditions.
Another key environmental adjustment is noise reduction. Hospital wards are notoriously noisy, with alarms, conversations, and equipment contributing to sensory overload. Implementing "quiet hours" during nighttime, using sound-absorbing materials in room design, and encouraging staff to minimize unnecessary noise can significantly improve patient outcomes. A practical tip for immediate implementation is the use of white noise machines or earplugs for patients, particularly in intensive care units where noise levels often exceed 80 decibels, far above the WHO-recommended 30 decibels for healing environments.
Spatial design also plays a pivotal role in delirium prevention. Cluttered, unfamiliar environments can exacerbate confusion. Hospitals can address this by creating clear, consistent layouts with visible landmarks, such as color-coded walls or themed corridors. Additionally, providing patients with personal items, like family photos or familiar objects, can help ground them in reality. For elderly patients, who are at higher risk of delirium, ensuring mobility aids are readily available and that rooms are free of trip hazards is essential. A comparative analysis in *The Lancet* highlighted that hospitals with patient-centered designs saw a 25% decrease in delirium cases among patients over 65.
Finally, temperature and air quality adjustments are often overlooked but crucial. Maintaining a consistent room temperature between 21°C and 24°C (70°F and 75°F) can prevent discomfort and agitation. Proper ventilation and air filtration systems reduce the risk of infections, which are known triggers of delirium. Hospitals can also introduce indoor plants or air purifiers to improve air quality, though care must be taken to avoid allergens. A persuasive argument for these adjustments lies in their cost-effectiveness: simple environmental modifications can reduce the need for pharmacological interventions, which often come with side effects and higher costs. By prioritizing these adjustments, hospitals can create a therapeutic environment that not only treats but also prevents delirium.
Michigan Hospitals at Capacity: Current Status and Patient Impact
You may want to see also
Explore related products

![Delirium: Photo of Gioia [4K Ultra HD + Blu-ray Set]](https://m.media-amazon.com/images/I/712-8+HrBCL._AC_UL320_.jpg)




![]()
Behavioral Management Strategies
Delirium, a sudden confusion often seen in hospitalized patients, particularly the elderly, demands immediate attention and tailored management. Among the array of interventions, behavioral management strategies stand out as a cornerstone in mitigating symptoms and improving outcomes. These strategies focus on creating a structured, calming environment while addressing the patient’s immediate needs without relying solely on pharmacological interventions.
Step 1: Establish a Predictable Routine
Patients with delirium thrive in environments with consistency. Implement a daily schedule that includes regular meal times, activity periods, and rest intervals. For example, orient the patient to time and place every morning using a large clock and calendar. During nighttime, reduce stimuli by dimming lights and minimizing noise. A study in *JAMA Internal Medicine* found that structured routines reduced delirium duration by 20% in post-surgical patients aged 65 and older.
Caution: Avoid Overstimulation
While engagement is crucial, overloading the patient with activities or questions can exacerbate confusion. Limit interactions to 10–15 minutes at a time, and ensure caregivers speak clearly and calmly. For instance, instead of asking open-ended questions, use simple, yes-or-no queries like, “Would you like some water?”
Step 2: Leverage Non-Pharmacological Tools
Incorporate sensory aids such as hearing aids or glasses to address deficits that worsen disorientation. For agitated patients, consider weighted blankets or soft music to promote relaxation. A randomized trial published in *The Lancet* demonstrated that patients exposed to familiar music experienced a 30% reduction in agitation episodes compared to controls.
Analysis: Balancing Safety and Autonomy
While physical restraints may seem necessary for safety, they often increase agitation and risk of injury. Instead, use low beds and bed alarms to monitor mobility without restricting movement. For example, a 72-year-old patient with delirium in a hospital setting benefited from a low-bed setup, reducing fall risks by 40% while allowing freedom to move within safe limits.
Takeaway: Personalization is Key
By prioritizing consistency, sensory support, and individualized care, behavioral management strategies not only alleviate delirium symptoms but also foster a healing environment. These approaches, when integrated into hospital protocols, can significantly reduce the duration and impact of delirium, improving both patient and caregiver experiences.
Heparin in Hospitals: When and Why?
You may want to see also
Explore related products





![]()
Importance of Multidisciplinary Care Teams
Delirium, a sudden confusion often seen in hospitalized patients, particularly the elderly, requires a nuanced approach that extends beyond the capabilities of any single healthcare discipline. The complexity of its causes—ranging from medication side effects to underlying infections—demands a coordinated effort. This is where multidisciplinary care teams become indispensable. By bringing together professionals from diverse fields, these teams can address the multifaceted nature of delirium, ensuring that patients receive comprehensive and effective treatment.
Consider the role of a pharmacist in this context. They can review a patient’s medication regimen to identify drugs known to precipitate delirium, such as opioids or benzodiazepines, and recommend safer alternatives or dosage adjustments. For instance, reducing the dose of an anticholinergic medication by 25–50% in elderly patients can significantly lower the risk of delirium. Simultaneously, a physical therapist might design mobility exercises to prevent muscle weakness and deconditioning, which are common in bedridden patients. These interventions, when combined, create a synergistic effect that addresses both the pharmacological and physical contributors to delirium.
The inclusion of a geriatrician or internist is equally critical. These specialists can conduct thorough assessments to identify underlying conditions like urinary tract infections or dehydration, which often trigger delirium in older adults. For example, prompt administration of intravenous fluids at a rate of 1–2 liters over 24 hours can correct dehydration, a reversible cause of delirium. A psychiatrist or psychologist, on the other hand, can evaluate cognitive function and provide strategies to manage agitation or hallucinations, such as reorientation techniques or the use of low-dose antipsychotics like quetiapine (25–50 mg daily) when necessary.
Nurses play a pivotal role in this team, serving as the eyes and ears at the bedside. They monitor subtle changes in a patient’s mental status, such as increased confusion or restlessness, and communicate these findings to the team. For instance, implementing a delirium screening tool like the Confusion Assessment Method (CAM) during every shift can ensure early detection and intervention. Additionally, nurses can educate family members on how to support their loved ones, such as maintaining a consistent sleep-wake cycle or providing familiar objects to reduce disorientation.
The strength of a multidisciplinary team lies in its ability to integrate these diverse perspectives into a cohesive care plan. For example, while a physician focuses on treating the underlying infection with antibiotics, a dietitian might address malnutrition by recommending high-protein supplements or ensuring adequate calorie intake. A social worker could assess the patient’s home environment to plan for a safe discharge, reducing the risk of readmission. This collaborative approach not only improves patient outcomes but also enhances efficiency, as each team member contributes their unique expertise to address specific aspects of delirium.
In practice, hospitals can foster multidisciplinary care by establishing delirium protocols that outline the roles and responsibilities of each team member. Regular team meetings, such as daily rounds or weekly case conferences, ensure ongoing communication and coordination. For instance, a 78-year-old patient with hip surgery might benefit from a protocol that includes pain management by an anesthesiologist, mobility exercises by a physical therapist, and cognitive monitoring by a nurse. By working together, these professionals can prevent delirium from prolonging hospital stays or leading to long-term cognitive decline.
Ultimately, the importance of multidisciplinary care teams in treating delirium cannot be overstated. Their ability to address the condition’s multifaceted nature ensures that patients receive holistic, evidence-based care. Hospitals that invest in such teams not only improve patient outcomes but also reduce healthcare costs associated with prolonged hospitalizations and complications. In the fight against delirium, collaboration is not just beneficial—it’s essential.
How Hospitals Manage and Offset Indigent Care Costs Effectively
You may want to see also
Frequently asked questions
No, delirium treatment depends on severity and underlying causes. Mild cases may be managed at home with close monitoring, while severe or complex cases often require hospitalization.
In-hospital treatment includes identifying and addressing underlying causes, medication adjustments, hydration, and supportive care. Antipsychotics or sedatives may be used in severe cases.
The duration varies based on the individual’s condition and response to treatment. Some patients improve within days, while others may require weeks of care.
Yes, hospitals use strategies like maintaining a consistent environment, minimizing sedatives, ensuring hydration, and promoting mobility to reduce the risk of delirium.








![Delirium [Blu-ray] [2021]](https://m.media-amazon.com/images/I/81yAcLCfmwL._AC_UL320_.jpg)






















