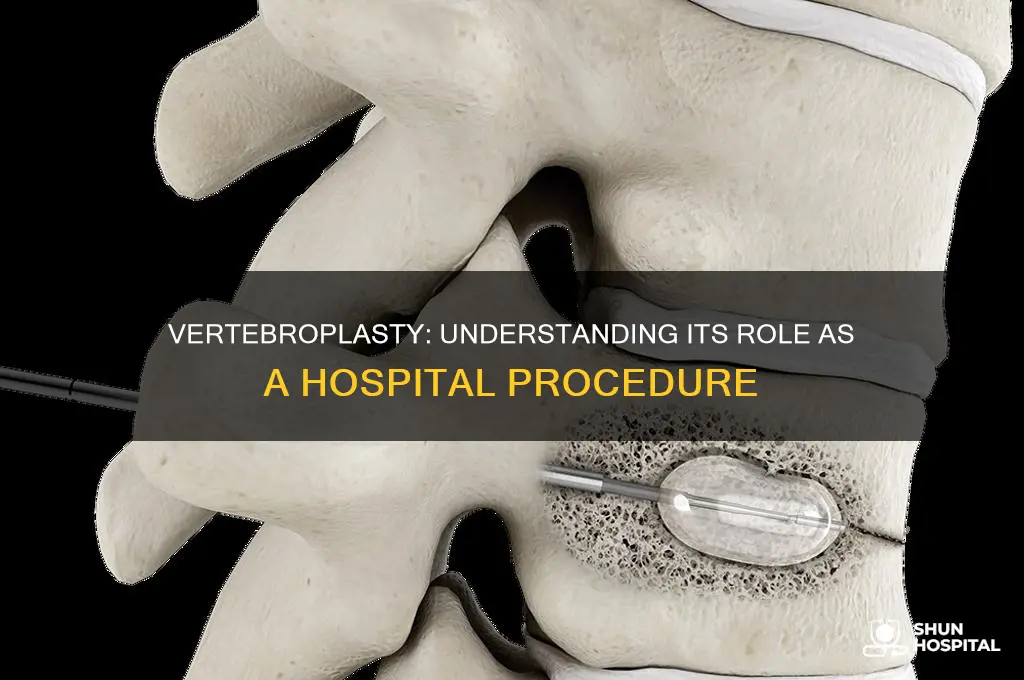
Vertebroplasty is a minimally invasive medical procedure primarily performed in a hospital setting, although it can also take place in an outpatient surgery center. It involves the injection of bone cement into a fractured vertebra to stabilize the bone and alleviate pain, particularly in cases of osteoporotic or traumatic vertebral fractures. The procedure is typically carried out by interventional radiologists or spine surgeons under local or general anesthesia, with the use of imaging guidance such as fluoroscopy to ensure precision. While vertebroplasty is generally safe and effective, it requires a controlled environment like a hospital to manage potential complications, such as cement leakage or infection, and to provide immediate access to emergency care if needed.
Explore related products






What You'll Learn
- Procedure Overview: Minimally invasive, stabilizes fractured vertebrae using bone cement injection under imaging guidance
- Patient Selection: Ideal for painful vertebral compression fractures, especially in osteoporosis or trauma cases
- Risks & Complications: Potential cement leakage, infection, nerve damage, or new fractures post-procedure
- Recovery Process: Typically outpatient, with immediate pain relief and minimal downtime for most patients
- Alternatives: Kyphoplasty, conservative management, or pain medications as non-surgical treatment options
![]()
Procedure Overview: Minimally invasive, stabilizes fractured vertebrae using bone cement injection under imaging guidance
Vertebroplasty is a minimally invasive procedure designed to stabilize fractured vertebrae by injecting bone cement under precise imaging guidance. Unlike open surgery, it requires only a small incision, typically less than 1 cm, through which a needle is inserted into the damaged vertebra. This outpatient procedure is often performed in a hospital setting, specifically in an interventional radiology suite or operating room, where advanced imaging technology like fluoroscopy ensures accurate cement placement. The entire process usually takes 30 to 60 minutes per vertebra, with patients often returning home the same day.
The procedure begins with the patient lying face down on the operating table. Local anesthesia is administered to numb the area, and in some cases, mild sedation is provided to ensure comfort. Using real-time imaging, the physician guides a biopsy needle into the fractured vertebra, avoiding critical structures like spinal nerves and blood vessels. Once proper placement is confirmed, a small amount of polymethylmethacrylate (PMMA) bone cement, typically 2 to 6 ml per vertebra, is slowly injected. The cement hardens within minutes, stabilizing the fracture and reducing pain.
While vertebroplasty is generally safe, it is not without risks. Potential complications include cement leakage, infection, or nerve injury, though these occur in less than 5% of cases. The procedure is most effective for acute vertebral fractures caused by osteoporosis or trauma, particularly in patients over 50. It is less suitable for fractures older than 6 months or those caused by cancer, as the cement may not adhere properly. Post-procedure, patients are advised to avoid strenuous activity for 24 hours and monitor for signs of infection or unusual pain.
Comparatively, vertebroplasty offers a quicker recovery and lower complication rate than traditional open surgery, making it a preferred option for eligible candidates. Its minimally invasive nature also reduces hospital stays, with most patients experiencing significant pain relief within 48 hours. However, it is not a cure for underlying conditions like osteoporosis, and patients may require additional treatments to prevent future fractures. Practical tips include wearing loose clothing for the procedure and arranging for a ride home, as sedation may impair driving ability.
In conclusion, vertebroplasty is a hospital-based procedure that combines precision, efficiency, and minimal invasiveness to address vertebral fractures. Its success hinges on skilled execution and patient selection, offering a viable solution for those seeking rapid pain relief and improved mobility. As with any medical intervention, understanding its benefits, limitations, and aftercare is crucial for optimal outcomes.
Lake Cumberland Hospital: MDs and Medical Care
You may want to see also
Explore related products






![]()
Patient Selection: Ideal for painful vertebral compression fractures, especially in osteoporosis or trauma cases
Vertebroplasty is a minimally invasive procedure that offers significant pain relief for patients suffering from vertebral compression fractures (VCFs), particularly those caused by osteoporosis or trauma. The key to its success lies in precise patient selection, ensuring that the procedure is both safe and effective. Ideal candidates are those experiencing acute, severe pain that has not responded to conservative treatments such as pain medication, bracing, or physical therapy. For instance, patients with osteoporosis-related fractures often report pain lasting more than 6 weeks despite optimal medical management, making them prime candidates for vertebroplasty. Similarly, individuals with traumatic VCFs who experience debilitating pain that hinders daily activities can benefit significantly from this intervention.
When evaluating patient suitability, clinicians must consider the fracture’s acuity and the patient’s overall health. Vertebroplasty is most effective for fractures less than 6 months old, as older fractures may have already undergone significant healing, reducing the procedure’s impact. Age is another critical factor; while vertebroplasty is commonly performed on older adults, particularly those over 65, younger patients with traumatic fractures may also be eligible if their pain is severe and persistent. For example, a 72-year-old woman with osteoporotic VCFs and a visual analog scale (VAS) pain score of 8/10 would be an ideal candidate, whereas a 45-year-old with a healed fracture and mild discomfort would not.
The procedure itself is typically performed in a hospital or outpatient setting under fluoroscopic guidance, with the patient under conscious sedation. A small amount of polymethylmethacrylate (PMMA) cement is injected into the fractured vertebra to stabilize it and alleviate pain. While generally safe, patient selection is crucial to minimize risks such as cement leakage or infection. For instance, patients with coagulopathies or those on anticoagulants may require additional precautions or temporary medication adjustments. Practical tips include ensuring patients fast for at least 6 hours before the procedure and arranging for transportation home, as sedation can impair driving ability.
Comparatively, vertebroplasty stands out as a targeted solution for VCF-related pain, especially when contrasted with kyphoplasty, which involves balloon inflation before cement injection. While kyphoplasty may restore vertebral height, vertebroplasty is often preferred for its simplicity and effectiveness in pain relief. For example, a study published in *The New England Journal of Medicine* found that vertebroplasty provided significant pain reduction within 48 hours for patients with osteoporotic fractures, highlighting its role as a first-line intervention for carefully selected patients.
In conclusion, patient selection is the cornerstone of successful vertebroplasty, particularly for those with painful VCFs due to osteoporosis or trauma. By focusing on acute, severe pain unresponsive to conservative measures, clinicians can identify ideal candidates who stand to gain the most from this procedure. Specific considerations, such as fracture acuity, patient age, and overall health, ensure both safety and efficacy. With proper selection and execution, vertebroplasty remains a valuable tool in managing VCF-related pain, offering rapid relief and improved quality of life for those who need it most.
Cash Donations: Improving Hospital Quality?
You may want to see also
Explore related products






![]()
Risks & Complications: Potential cement leakage, infection, nerve damage, or new fractures post-procedure
Vertebroplasty, a procedure often performed in hospital settings, involves injecting bone cement into fractured vertebrae to stabilize the spine and alleviate pain. While it offers significant relief for many patients, particularly those with osteoporotic compression fractures, it is not without risks. Among the most concerning complications are cement leakage, infection, nerve damage, and new fractures post-procedure. Understanding these risks is crucial for patients and healthcare providers alike to make informed decisions and manage expectations.
Cement leakage is one of the most common complications, occurring in up to 67% of cases, though often asymptomatic. When cement leaks into surrounding tissues, it can cause serious issues such as spinal cord or nerve root compression, pulmonary embolism, or even cardiac complications if it enters the bloodstream. To mitigate this risk, radiologists use real-time imaging, such as fluoroscopy, to monitor cement placement. Patients should be aware that while minor leaks may resolve without intervention, severe cases may require additional procedures or medication to manage symptoms.
Infection, though rare (occurring in less than 1% of cases), poses a significant threat due to the introduction of foreign material into the body. Post-procedure infections can manifest as discitis, osteomyelitis, or abscess formation, often requiring prolonged antibiotic therapy or surgical debridement. Patients with compromised immune systems, diabetes, or a history of prior infections are at higher risk. Strict sterile techniques during the procedure and careful post-operative monitoring are essential to minimize this complication.
Nerve damage is another critical concern, with symptoms ranging from mild numbness to severe paralysis. This complication typically arises from direct needle trauma or cement compression on neural structures. Studies indicate that nerve injury occurs in approximately 0.5–1% of cases. To reduce this risk, precise needle placement and limited cement volume (typically 3–6 ml per vertebra) are crucial. Patients experiencing persistent neurological symptoms post-procedure should seek immediate medical attention.
Lastly, new fractures post-vertebroplasty, while less common, highlight the procedure’s limitations. Treating one vertebra can alter spinal mechanics, potentially increasing stress on adjacent levels and leading to future fractures. This risk is particularly relevant in patients with osteoporosis, who may require concurrent pharmacological management to strengthen bone density. Regular follow-up imaging and bone health assessments are recommended to monitor spinal integrity and address emerging issues proactively.
In summary, while vertebroplasty is a valuable hospital procedure for managing vertebral fractures, its risks demand careful consideration. Patients and providers must weigh the benefits against potential complications, ensuring informed consent and tailored post-procedure care. Awareness of these risks empowers individuals to take proactive steps in their recovery and long-term spinal health.
Exploring Diverse Roles in Hospital Human Resource Management Careers
You may want to see also
Explore related products






![]()
Recovery Process: Typically outpatient, with immediate pain relief and minimal downtime for most patients
Vertebroplasty, a minimally invasive procedure designed to stabilize vertebral compression fractures, often raises questions about its recovery process. Typically performed as an outpatient procedure, it allows patients to return home the same day, a stark contrast to more invasive spinal surgeries. This immediate transition from hospital to home underscores the procedure’s efficiency and the minimal physical toll it takes on the body. For most patients, the recovery process is straightforward, marked by rapid pain relief and a return to daily activities within a short timeframe.
The outpatient nature of vertebroplasty is a key advantage, particularly for older adults or those with limited mobility. Patients are usually monitored for a few hours post-procedure to ensure stability and manage any immediate side effects, such as mild discomfort or nausea. Pain relief is often immediate, with many reporting significant improvement as soon as the cement hardens in the fractured vertebra. This quick turnaround is attributed to the procedure’s targeted approach, which directly addresses the source of pain without extensive tissue disruption.
While recovery is generally swift, patients are advised to follow specific guidelines to ensure optimal healing. For the first 24 hours, avoiding strenuous activities, heavy lifting, or twisting motions is crucial. Patients may resume light activities, such as walking, immediately, as movement aids in circulation and reduces stiffness. Over-the-counter pain relievers can be used as needed, though severe pain should be reported to the healthcare provider. A follow-up appointment is typically scheduled within a week to assess recovery and address any concerns.
Comparatively, vertebroplasty’s recovery process is far less demanding than that of traditional open spinal surgeries, which often require hospitalization and weeks of restricted activity. The minimal downtime associated with vertebroplasty makes it an attractive option for those seeking quick relief from debilitating back pain. However, individual recovery experiences may vary based on factors like age, overall health, and the severity of the fracture. Patients with multiple fractures or underlying conditions may require a slightly longer recovery period.
In conclusion, vertebroplasty’s recovery process is designed for convenience and efficiency, aligning with its outpatient framework. Immediate pain relief, minimal restrictions, and a focus on early mobility make it a practical solution for many. By adhering to post-procedure guidelines and staying in communication with healthcare providers, patients can maximize the benefits of this procedure and return to their normal routines with confidence.
Unveiling the Mystery: The Guy in Hospital in Metal Gear Solid V
You may want to see also
Explore related products





![]()
Alternatives: Kyphoplasty, conservative management, or pain medications as non-surgical treatment options
Vertebroplasty, while effective for certain spinal fractures, is not the only option for patients seeking relief. For those hesitant about surgery or ineligible due to fracture characteristics, alternatives like kyphoplasty, conservative management, and pain medications offer viable pathways to recovery. Each approach carries distinct advantages and considerations, tailored to individual needs and medical profiles.
Kyphoplasty, a close relative of vertebroplasty, addresses not only pain but also spinal deformity. Unlike vertebroplasty, which injects bone cement directly into the fractured vertebra, kyphoplasty first restores vertebral height using a balloon-like device before cement is introduced. This two-step process can improve spinal alignment and reduce the risk of cement leakage. Studies show kyphoplasty provides significant pain relief within days, with improvements in mobility and quality of life. However, it remains a hospital-based procedure, typically performed under local anesthesia with sedation, and may not be suitable for patients with osteoporosis or certain fracture types. Recovery involves limited activity for 24–48 hours, followed by gradual resumption of normal routines.
Conservative management, on the other hand, avoids invasive procedures altogether, relying on rest, bracing, and physical therapy. A lumbar brace, worn for 6–12 weeks, immobilizes the spine to facilitate healing. Physical therapy, initiated after 4–6 weeks, focuses on strengthening core muscles and improving flexibility. This approach is particularly effective for stable fractures without neurological symptoms. While pain relief may be slower compared to surgical interventions, conservative management carries no procedural risks and is cost-effective. Patients over 65 or those with comorbidities often find this route preferable, though adherence to bracing and therapy protocols is critical for success.
Pain medications serve as a cornerstone of non-surgical treatment, often used in conjunction with other modalities. Acetaminophen (up to 3,000 mg/day) is typically the first-line option, while NSAIDs like ibuprofen (600–800 mg every 6–8 hours) can address inflammation. For severe pain, short-term opioids (e.g., hydrocodone 5–10 mg every 4–6 hours) may be prescribed, though their use is limited to 7–14 days due to addiction risks. Adjuvant therapies, such as lidocaine patches or gabapentin (300–600 mg three times daily), can target neuropathic pain. Patients must monitor for side effects, such as gastrointestinal bleeding with NSAIDs or drowsiness with opioids, and consult their physician for dosage adjustments.
Choosing among these alternatives requires a nuanced understanding of patient-specific factors. Kyphoplasty offers rapid pain relief and structural correction but demands a hospital setting. Conservative management prioritizes safety and simplicity but demands patience and commitment. Pain medications provide immediate symptom control but must be carefully managed to avoid complications. By weighing these options against individual health status, fracture severity, and lifestyle, patients and providers can collaboratively devise the most effective treatment plan.
Community-Centered Innovation: How Hospitals Drive Health Equity Forward
You may want to see also
Frequently asked questions
Yes, vertebroplasty is typically performed in a hospital setting, often in an outpatient or ambulatory surgery center.
The procedure usually takes about 1 to 2 hours, depending on the complexity of the case.
Most patients are discharged the same day, but some may require a short observation period or overnight stay if complications arise.
It is usually done under local anesthesia with mild sedation, though general anesthesia may be used in certain cases.
While generally safe, risks include infection, bleeding, nerve damage, or cement leakage, which are monitored and managed in the hospital setting.