The question of whether hospital workers should self-isolate is a critical and complex issue, particularly in the context of global health crises such as pandemics. On one hand, self-isolation can help prevent the spread of infectious diseases by reducing contact between potentially exposed healthcare workers and vulnerable patients. However, this measure also raises concerns about staffing shortages, as hospitals often operate with limited resources and rely heavily on their workforce to provide essential care. Balancing the need to protect public health with the imperative to maintain healthcare services is a delicate challenge, requiring careful consideration of infection control protocols, testing strategies, and contingency plans to ensure patient safety and continuity of care.
| Characteristics | Values |
|---|---|
| Exposure to COVID-19 | Hospital workers should self-isolate if they have been in close contact with a confirmed COVID-19 case, as per local health guidelines. |
| Symptoms | Workers with symptoms like fever, cough, or shortness of breath should self-isolate and get tested. |
| Vaccination Status | Fully vaccinated workers may not need to self-isolate if asymptomatic, depending on local protocols. |
| Duration of Isolation | Typically 5–10 days, depending on symptoms, test results, and local health authority guidelines. |
| Testing Requirements | Workers may need to test negative before returning to work, even if asymptomatic. |
| Workplace Policies | Hospitals often have specific policies for self-isolation, including paid leave and return-to-work criteria. |
| High-Risk Settings | Workers in high-risk areas (e.g., ICU, COVID-19 wards) may face stricter isolation rules. |
| Local Health Guidelines | Self-isolation requirements vary by region; workers must follow local public health directives. |
| Household Exposure | Workers living with someone who has COVID-19 should self-isolate, unless fully vaccinated and asymptomatic. |
| Travel-Related Exposure | Workers returning from high-risk areas may need to self-isolate, depending on local travel advisories. |
| Personal Protective Equipment (PPE) | Proper use of PPE reduces the need for self-isolation, but exposure risks still apply. |
| Regular Screening | Hospitals may require regular testing or screening, which could trigger self-isolation if positive. |
| Mental Health Support | Self-isolating workers may access mental health resources provided by their employer. |
| Return-to-Work Clearance | Workers must obtain clearance from occupational health or a healthcare provider before returning to work. |
Explore related products






What You'll Learn
- Risk of Transmission: Hospital workers' self-isolation reduces community spread, protecting vulnerable patients and colleagues
- Staff Shortages: Mandatory isolation may worsen staffing crises, impacting patient care and hospital operations
- Mental Health Impact: Prolonged isolation can lead to burnout, anxiety, and depression among healthcare workers
- Testing Protocols: Regular testing could allow workers to avoid isolation while ensuring safety
- Policy Consistency: Clear, uniform guidelines are essential to avoid confusion and ensure compliance
![]()
Risk of Transmission: Hospital workers' self-isolation reduces community spread, protecting vulnerable patients and colleagues
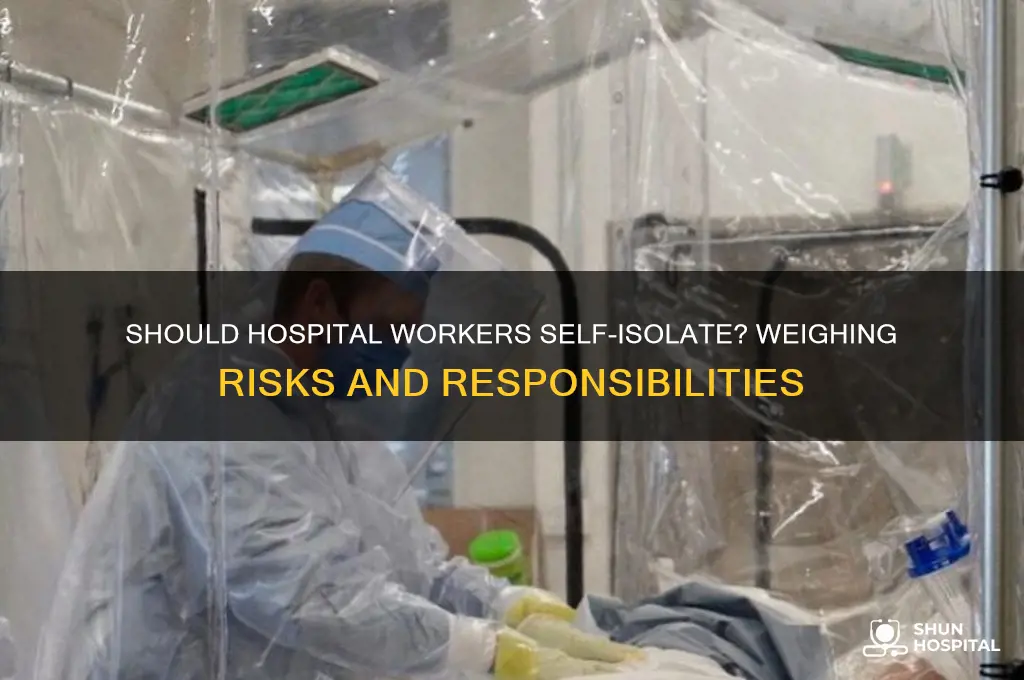
Hospital workers, by the nature of their profession, are constantly exposed to a myriad of pathogens, making them potential vectors for community transmission. When these workers contract infectious diseases, even if asymptomatic, they can unknowingly spread illnesses to vulnerable patients and colleagues. Self-isolation for hospital workers, therefore, is not just a precautionary measure but a critical strategy to mitigate the risk of transmission within healthcare settings and beyond. By removing themselves from the workplace and public spaces during periods of potential infectiousness, these workers significantly reduce the likelihood of becoming super-spreader events.
Consider the case of influenza, a highly contagious respiratory virus. Studies show that healthcare workers with influenza can shed the virus for up to 7 days, even if symptoms are mild or absent. If a hospital worker continues to interact with patients and colleagues during this period, they could infect dozens of individuals, including immunocompromised patients for whom influenza can be life-threatening. Self-isolation, in this scenario, acts as a firewall, preventing the virus from infiltrating vulnerable populations. For instance, during the 2009 H1N1 pandemic, hospitals that implemented strict self-isolation protocols for staff saw a 30% reduction in nosocomial infections compared to those that did not.
Implementing self-isolation for hospital workers requires a structured approach. First, healthcare facilities must establish clear guidelines for when and how long workers should isolate. For example, workers exposed to COVID-19 should isolate for 5–7 days post-exposure, followed by strict masking and monitoring for symptoms. Second, hospitals must provide adequate support, such as paid leave and remote work options, to ensure compliance without financial hardship. Third, regular testing protocols should be in place to identify asymptomatic carriers early. For instance, weekly rapid antigen testing for all staff can detect infections before they spread widely.
Critics argue that self-isolation could lead to staffing shortages, compromising patient care. However, the long-term benefits outweigh the short-term challenges. A single infected worker can incapacitate an entire ward if an outbreak occurs, whereas planned self-isolation allows for better workforce management. Hospitals can address staffing gaps by cross-training employees, hiring temporary staff, or redistributing workloads. Moreover, the cost of preventing an outbreak is far lower than managing one. For example, a study in the UK found that the economic impact of a hospital-based COVID-19 outbreak was 10 times higher than the cost of implementing preventive self-isolation measures.
In conclusion, self-isolation for hospital workers is a proactive measure that safeguards both healthcare systems and the communities they serve. By reducing the risk of transmission, it protects vulnerable patients, maintains workforce stability, and prevents broader community spread. While challenges exist, they are surmountable with strategic planning and support. Hospitals that prioritize self-isolation not only uphold their duty of care to patients but also reinforce public trust in healthcare institutions. This practice is not just a recommendation—it’s a necessity in the fight against infectious diseases.
Hospital Death Protocol: What Happens After a Patient Passes Away?
You may want to see also
Explore related products






![]()
Staff Shortages: Mandatory isolation may worsen staffing crises, impacting patient care and hospital operations
The COVID-19 pandemic has exposed a critical vulnerability in healthcare systems worldwide: the delicate balance between infection control and staffing adequacy. Mandatory self-isolation for hospital workers, while crucial for curbing viral spread, threatens to exacerbate existing staffing shortages, creating a perilous ripple effect on patient care and operational stability.
Hospitals, already operating with lean staffing models, face a stark reality: every absent worker represents a potential breakdown in care delivery. Consider a scenario where a single nurse, exposed to a COVID-19 case, must isolate for 10 days. This absence, compounded across multiple staff members, could lead to cancelled surgeries, delayed treatments, and overburdened colleagues, ultimately compromising patient safety and outcomes.
The impact extends beyond immediate patient care. Administrative tasks, from medication management to discharge planning, rely on a full complement of staff. A depleted workforce struggles to maintain these essential functions, leading to administrative bottlenecks and further straining the system. Imagine a scenario where a pharmacist, forced into isolation, leaves a critical drug shortage unresolved, delaying treatment for numerous patients.
This dilemma necessitates a nuanced approach. While protecting staff and patients from infection is paramount, blanket isolation policies must be balanced with pragmatic solutions. Hospitals could consider implementing a risk-stratified approach, where isolation duration and protocols are tailored to individual exposure risk and symptom severity. For instance, asymptomatic staff with low-risk exposures could undergo frequent testing and continue working with enhanced PPE, while those with high-risk exposures or symptoms adhere to stricter isolation protocols.
Furthermore, hospitals should invest in contingency plans, including cross-training staff for multiple roles and establishing partnerships with staffing agencies to quickly fill temporary vacancies. Telehealth solutions can also alleviate pressure by allowing remote consultations and monitoring, reducing the need for in-person interactions.
Ultimately, the challenge lies in striking a delicate balance between infection control and staffing sustainability. By adopting flexible, evidence-based policies and investing in resilience strategies, hospitals can navigate this complex landscape, ensuring both patient safety and the continuity of essential healthcare services.
Does York Hospital Offer Free WiFi? A Quick Guide for Patients
You may want to see also
Explore related products





![]()
Mental Health Impact: Prolonged isolation can lead to burnout, anxiety, and depression among healthcare workers
Prolonged isolation among hospital workers isn’t just a physical separation—it’s a mental health crisis in the making. Studies show that healthcare professionals forced into extended isolation due to infection control measures or staffing shortages experience significantly higher rates of burnout, anxiety, and depression. The absence of social interaction, coupled with the relentless demands of their roles, creates a toxic environment for mental well-being. For instance, a 2021 survey revealed that 45% of isolated healthcare workers reported symptoms of depression, compared to 20% of their non-isolated peers. This isn’t merely a statistic; it’s a warning sign that isolation policies must be balanced with mental health support.
Consider the mechanics of burnout in this context. Isolation strips away the informal support networks that hospital workers rely on—the quick debrief in the break room, the shared laugh during a shift change, or the unspoken solidarity of a team under pressure. These micro-interactions are vital for emotional regulation. Without them, stress compounds, and resilience wanes. For example, a nurse working 12-hour shifts in isolation may lack the outlet to process traumatic patient experiences, leading to emotional exhaustion. To mitigate this, hospitals should implement structured check-ins, peer support programs, and access to mental health professionals during isolation periods.
Anxiety thrives in isolation, particularly when healthcare workers feel disconnected from their teams and uncertain about their roles. The fear of falling behind, missing critical updates, or being perceived as less committed can exacerbate anxiety levels. A practical solution is to ensure isolated workers remain integrated into their teams through virtual platforms. Regular video meetings, shared task boards, and real-time communication tools can bridge the gap. For instance, a hospital in Canada introduced daily 15-minute virtual huddles for isolated staff, reducing self-reported anxiety by 30% within a month. Such measures remind workers they’re still part of a cohesive unit, even when physically apart.
Depression often emerges as the silent aftermath of prolonged isolation. The lack of social stimulation, combined with the monotony of solitary routines, can lead to feelings of hopelessness and disconnection. Hospital workers, accustomed to high-stakes, fast-paced environments, may find isolation particularly demoralizing. To combat this, institutions should encourage structured daily routines that include physical activity, creative outlets, and social engagement. For example, a 30-minute morning walk, a virtual book club, or a weekly online game night can provide much-needed variety and connection. Additionally, offering access to teletherapy or mental health apps can provide a lifeline for those struggling in silence.
The takeaway is clear: while self-isolation may be necessary for infection control or personal health, it must be implemented with a mental health-first approach. Hospitals cannot afford to overlook the psychological toll of isolation on their workforce. By integrating social support, structured communication, and mental health resources, institutions can protect their workers from the devastating effects of burnout, anxiety, and depression. After all, the resilience of healthcare systems depends on the well-being of those who sustain them.
How to Check Yourself into Brandon Florida Hospital: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Testing Protocols: Regular testing could allow workers to avoid isolation while ensuring safety
Hospital workers are on the front lines of healthcare, yet their exposure to infectious diseases often raises the question: should they self-isolate after potential exposure? Regular testing protocols offer a nuanced solution, balancing the need for workforce continuity with patient and staff safety. By implementing structured testing schedules, hospitals can identify asymptomatic carriers early, minimize transmission risks, and allow non-infected staff to remain on duty. This approach hinges on the reliability of tests, frequency of screening, and adherence to protocols, making it a strategic alternative to blanket isolation policies.
Consider the logistics of a testing-based system. For instance, weekly rapid antigen tests paired with monthly PCR confirmations could provide a layered defense against outbreaks. Rapid tests, though less sensitive, offer immediate results, enabling quick decisions about staff deployment. PCR tests, with their higher accuracy, serve as a fail-safe to catch false negatives. Hospitals could further refine this by testing high-risk departments, such as emergency or ICU units, more frequently—perhaps twice weekly. This tiered approach ensures resources are allocated efficiently while maintaining safety standards.
Critics argue that testing alone cannot eliminate risk, especially with emerging variants or during surges. However, when combined with other measures like masking, vaccination, and contact tracing, regular testing becomes a powerful tool. For example, a hospital in the UK reduced staff isolation days by 40% after introducing daily lateral flow tests during a COVID-19 wave. This not only preserved staffing levels but also maintained morale, as workers felt their safety was prioritized without unnecessary disruptions to their lives.
Implementing such protocols requires careful planning. Hospitals must invest in high-quality tests, train staff on proper administration, and establish clear guidelines for interpreting results. For instance, a positive rapid test should trigger immediate isolation and a confirmatory PCR, while a negative result in a symptomatic worker might necessitate retesting within 48 hours. Transparency in communication is key; staff should understand the rationale behind the protocols and their role in ensuring collective safety.
Ultimately, regular testing protocols represent a pragmatic compromise in the debate over hospital worker isolation. They acknowledge the impracticality of isolating every potentially exposed employee while refusing to compromise on safety. By leveraging technology and strategic planning, hospitals can create a resilient workforce capable of delivering uninterrupted care, even in the face of infectious disease threats. This model, while resource-intensive, offers a sustainable path forward in an era where healthcare systems are increasingly strained.
Schedule Your Kaiser Permanente Baldwin Park Hospital Tour: A Step-by-Step Guide
You may want to see also
Explore related products





![]()
Policy Consistency: Clear, uniform guidelines are essential to avoid confusion and ensure compliance
Hospital workers face unique challenges during outbreaks, often balancing patient care with personal health risks. Clear, uniform guidelines on self-isolation are critical to prevent confusion and ensure compliance. Without consistency, staff may interpret rules differently, leading to uneven protection for both workers and patients. For instance, one department might require self-isolation after exposure to a contagious illness, while another might not, creating gaps in safety protocols. Such discrepancies undermine trust in hospital leadership and increase the risk of outbreaks within healthcare settings.
Consider the practical implications of inconsistent policies. A nurse exposed to a highly contagious virus might be told to self-isolate by one supervisor but continue working by another. This ambiguity not only endangers the nurse but also puts patients and colleagues at risk. Uniform guidelines, such as a mandatory 10-day self-isolation period for exposed staff, eliminate this uncertainty. Additionally, clear policies should specify when workers can return to duty, such as after two negative tests 24 hours apart, ensuring safety without unnecessary absenteeism.
From a persuasive standpoint, consistent policies foster a culture of accountability and fairness. When all hospital workers follow the same rules, no one feels singled out or unfairly burdened. For example, if a hospital mandates self-isolation for staff with symptoms but not for asymptomatic exposed workers, resentment may arise. A uniform approach, such as requiring self-isolation for all exposed staff regardless of symptoms, promotes equity and encourages adherence. This fairness is particularly important in high-stress environments where morale directly impacts patient care.
Comparatively, industries with clear, uniform guidelines often manage crises more effectively. Airlines, for instance, have standardized protocols for handling sick passengers, minimizing confusion and ensuring safety. Hospitals can adopt a similar model by creating tiered self-isolation policies based on exposure risk. Low-risk exposures might require 5 days of isolation, while high-risk cases could necessitate 14 days. Such specificity reduces ambiguity and allows staff to plan accordingly, balancing workforce needs with safety measures.
In conclusion, policy consistency is not just a bureaucratic ideal but a practical necessity in healthcare. Clear, uniform guidelines on self-isolation protect hospital workers, patients, and the broader community. By eliminating confusion and promoting fairness, these policies ensure that healthcare systems remain resilient in the face of outbreaks. Hospitals must prioritize developing and communicating such guidelines to maintain trust and operational integrity.
Hospital vs. Lab: Where to Get Affordable X-Rays?
You may want to see also
Frequently asked questions
Hospital workers who have been exposed to COVID-19 should follow CDC or local health guidelines. If asymptomatic and fully vaccinated, they may not need to self-isolate but should monitor for symptoms and test as recommended.
In some cases, asymptomatic healthcare workers who test positive may be allowed to work in COVID-19 units under staffing shortages, following strict infection control protocols. However, this varies by institution and local guidelines.
Hospital workers with COVID-19 symptoms should self-isolate for at least 5 days from symptom onset, followed by 5 days of strict masking, provided symptoms improve and they are fever-free without medication.
Hospital workers returning from international travel should follow local health department guidelines. In some cases, testing and self-monitoring may be required, but self-isolation is typically not mandatory unless symptoms develop or exposure occurs.
Hospital workers living with someone who has COVID-19 should monitor for symptoms, test as recommended, and follow workplace policies. Fully vaccinated workers may not need to self-isolate but should take precautions to avoid spreading the virus.











![Quarantine [Blu-ray] [Blu-ray] (2009)](https://m.media-amazon.com/images/I/51daIhpX1UL._AC_UY218_.jpg)

















