Deciding whether to discharge a patient from the hospital with a white blood cell (WBC) count of 16 requires careful consideration of the individual’s overall clinical condition, underlying health issues, and the context of the elevated WBC count. A WBC count of 16 is mildly elevated, typically indicating a response to infection, inflammation, or stress, but it is not an absolute criterion for hospitalization or discharge. Key factors to evaluate include the patient’s symptoms, vital signs, the presence of fever, the source of infection (if any), and any comorbidities that may complicate recovery. For instance, a stable patient with a localized infection and improving symptoms might be safely discharged with appropriate follow-up and outpatient management, while someone with systemic symptoms, severe illness, or immunocompromised status may require further monitoring in the hospital. Consultation with the healthcare team, including the primary physician and specialists, is essential to ensure a safe and informed decision.
Explore related products





What You'll Learn
- Understanding WBC Levels: Normal range, causes of elevation, and implications for health
- Infection Risk Assessment: Evaluating if elevated WBC indicates unresolved infection
- Post-Hospital Monitoring: Home care tips and when to seek medical attention
- Medications Impact: How drugs affect WBC counts and recovery process
- Doctor’s Discharge Criteria: Factors considered before releasing patients with elevated WBC
![]()
Understanding WBC Levels: Normal range, causes of elevation, and implications for health
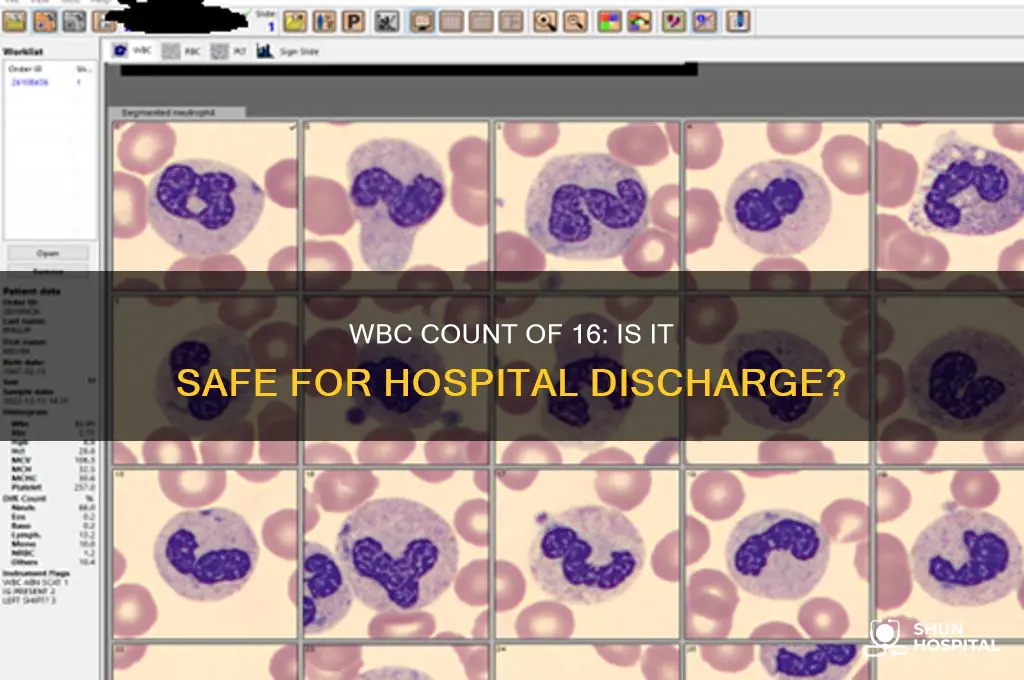
White blood cells (WBCs), also known as leukocytes, play a crucial role in the body's immune system by defending against infections and illnesses. Understanding WBC levels is essential for assessing overall health and identifying potential underlying issues. The normal range of WBCs in adults typically falls between 4,000 and 11,000 cells per microliter (µL) of blood. A WBC count of 16,000 cells/µL is considered elevated, a condition known as leukocytosis. While this may raise concerns, the decision to release a patient from the hospital with a WBC count of 16 depends on the clinical context, symptoms, and underlying causes of the elevation.
Elevated WBC levels can be caused by various factors, including infections (bacterial, viral, or fungal), inflammation, physical or emotional stress, certain medications, and underlying medical conditions such as autoimmune disorders or leukemia. In some cases, a WBC count of 16 may be a temporary response to a minor infection or stressor, while in others, it could indicate a more serious health issue. For instance, a mild elevation might be observed after surgery or during recovery from a common cold, whereas persistently high levels could signal a chronic condition requiring further investigation.
When considering whether a patient should be released from the hospital with a WBC count of 16, healthcare providers evaluate additional factors such as the patient's overall health, the presence of symptoms (e.g., fever, fatigue, or pain), and the results of other diagnostic tests. If the elevation is attributed to a manageable cause, such as a localized infection being treated with antibiotics, discharge may be appropriate with close follow-up care. However, if the cause remains unclear or if the patient is experiencing severe symptoms, further monitoring or treatment in the hospital may be necessary.
It is important for patients to communicate openly with their healthcare team about their concerns and symptoms. A WBC count of 16 alone is not a definitive indicator of whether hospitalization is required; rather, it is one piece of a larger clinical puzzle. Patients should follow their healthcare provider's recommendations, which may include additional testing, medication adjustments, or lifestyle changes to address the underlying cause of the elevated WBC levels.
In summary, a WBC count of 16 is above the normal range and warrants attention, but it does not automatically necessitate prolonged hospitalization. The decision to discharge a patient depends on the specific circumstances, including the cause of the elevation and the patient's overall condition. Understanding WBC levels and their implications empowers both patients and healthcare providers to make informed decisions about care and treatment, ensuring the best possible health outcomes.
Safety Net Hospitals: How Many Exist in the US?
You may want to see also
Explore related products





![]()
Infection Risk Assessment: Evaluating if elevated WBC indicates unresolved infection
When assessing whether an elevated white blood cell (WBC) count of 16 indicates an unresolved infection and impacts hospital discharge decisions, it is crucial to understand the context of this lab result. A WBC count of 16 × 10^9/L is considered mildly elevated, as the normal range typically falls between 4 and 11 × 10^9/L. While an elevated WBC count is often a marker of infection, it is not diagnostic on its own. Other factors, such as the patient’s clinical symptoms, medical history, and the presence of other lab abnormalities, must be considered in the infection risk assessment. For instance, if the patient is afebrile, asymptomatic, and has no signs of systemic infection, a WBC of 16 may not necessarily indicate an active, unresolved infection.
In evaluating infection risk, it is important to differentiate between the types of WBCs present, as this can provide additional insights. A differential WBC count can reveal whether the elevation is due to neutrophilia (often associated with bacterial infections), lymphocytosis (common in viral infections), or other abnormalities. For example, a left shift (presence of immature neutrophils) or toxic granulations in neutrophils may suggest a more severe or ongoing bacterial infection, even if the total WBC count is only mildly elevated. If the differential count shows a normal distribution and no signs of immature cells, the risk of unresolved infection may be lower, making hospital discharge more feasible.
The patient’s clinical course and response to treatment are critical in this assessment. If the patient has been treated for an infection (e.g., with antibiotics) and is improving clinically—with reduced fever, resolved symptoms, and stable vital signs—a mildly elevated WBC count may be a transient finding rather than a sign of persistent infection. However, if symptoms are worsening or new symptoms emerge, a WBC of 16 could indicate treatment failure or an unresolved infection, warranting further investigation before discharge. Serial WBC counts can also be helpful; a downward trend suggests resolution, while a stable or rising count may raise concerns.
Comorbidities and individual patient factors play a significant role in infection risk assessment. Patients with immunocompromised states (e.g., diabetes, HIV, or chemotherapy) may have a blunted WBC response to infection, making a count of 16 more concerning in this population. Similarly, elderly patients or those with chronic illnesses may have a higher baseline WBC count, requiring a more nuanced interpretation. In such cases, additional diagnostic tests, such as blood cultures, imaging, or inflammatory markers (e.g., CRP or procalcitonin), may be necessary to rule out unresolved infection before discharge.
Ultimately, the decision to discharge a patient with a WBC count of 16 should be individualized and based on a comprehensive risk assessment. If the elevated WBC is deemed unlikely to represent an unresolved infection—supported by clinical stability, normal differential count, and absence of red flags—discharge may be appropriate, with close outpatient follow-up. However, if uncertainty remains, further monitoring or additional diagnostics should be prioritized to avoid premature discharge, which could lead to complications or readmission. Collaboration between healthcare providers and clear communication with the patient about the risks and benefits of discharge are essential in these scenarios.
The Construction Timeline of the New Reid Hospital: A Detailed Overview
You may want to see also
Explore related products






![]()
Post-Hospital Monitoring: Home care tips and when to seek medical attention
After being discharged from the hospital with a white blood cell (WBC) count of 16, it's essential to continue monitoring your health and follow a structured home care routine. A WBC count of 16 is considered elevated, as the normal range is typically between 4,500 and 11,000 cells per microliter. This elevation may indicate an ongoing infection, inflammation, or stress on your body. Your healthcare provider likely deemed it safe for you to continue recovery at home, but vigilance is key to ensuring your condition improves. Here are detailed home care tips and guidelines on when to seek medical attention.
Home Care Tips for Post-Hospital Monitoring
First, prioritize rest and hydration. Your body needs energy to heal, so aim for 7-9 hours of sleep per night and take short naps if needed. Drink plenty of water to help flush toxins from your system and support your immune system. Maintain a balanced diet rich in fruits, vegetables, lean proteins, and whole grains to provide essential nutrients. Avoid processed foods, excessive sugar, and alcohol, as these can hinder recovery. If prescribed medications, take them exactly as directed, and do not skip doses. Keep a log of your symptoms, temperature, and how you feel daily to track progress and identify any concerning changes.
Monitoring Your WBC Levels and Symptoms
While at home, pay close attention to any persistent or worsening symptoms. These may include fever, chills, fatigue, body aches, or signs of infection such as redness, swelling, or pain at a wound site. If you had a specific condition that caused the elevated WBC count, monitor for symptoms related to that condition. For example, if you had a urinary tract infection, watch for burning during urination or frequent urges to urinate. Your healthcare provider may schedule a follow-up blood test to recheck your WBC count, so ensure you keep the appointment. If you notice any new or unusual symptoms, contact your doctor promptly.
When to Seek Medical Attention
Certain signs warrant immediate medical attention. Seek emergency care if you experience severe pain, difficulty breathing, chest pain, confusion, or a high fever (above 102°F or 39°C). Additionally, if your symptoms worsen despite following your treatment plan, or if you develop new symptoms like persistent cough, unexplained weight loss, or severe fatigue, contact your healthcare provider. An elevated WBC count can sometimes indicate a serious underlying issue, so it's better to err on the side of caution. Keep your hospital discharge papers and contact information for your healthcare team readily available.
Creating a Supportive Environment
Enlist the help of family members or friends to assist with daily tasks, especially if you're still feeling weak or fatigued. Avoid overexertion and gradually resume normal activities as your strength improves. Keep your living space clean to minimize the risk of infection, and wash your hands frequently. If you have pets, ensure they are healthy and up-to-date on vaccinations, as animals can sometimes carry infections. Stay informed about your condition and ask your healthcare provider any questions you have about your recovery process.
By following these home care tips and knowing when to seek medical attention, you can support your recovery and address any potential complications promptly. Remember, an elevated WBC count of 16 is a signal from your body that it’s working hard to heal, so give it the care and attention it needs. Always consult your healthcare provider if you’re unsure about your condition or symptoms.
Understanding Medicare Hospitalization Coverage and Deductibles
You may want to see also
Explore related products





![]()
Medications Impact: How drugs affect WBC counts and recovery process
Medications can significantly influence white blood cell (WBC) counts and the overall recovery process, making it crucial to understand their impact when considering hospital discharge with a WBC count of 16. Certain drugs, such as corticosteroids, are known to elevate WBC counts by stimulating the release of white blood cells from the bone marrow. While this might temporarily increase the count, it does not necessarily indicate a resolved infection or complete recovery. Patients on corticosteroids or similar medications should be monitored closely, as the elevated WBC count may mask underlying issues. Healthcare providers must assess whether the increase is medication-induced or a sign of ongoing inflammation or infection before deciding on discharge.
On the other hand, some medications can suppress WBC counts, complicating the interpretation of a count of 16. Chemotherapy drugs, immunosuppressants, and certain antibiotics are known to reduce white blood cell production or lifespan. In such cases, a WBC count of 16 might be higher than expected due to the medication’s suppressive effects, but it could still be insufficient for fighting infections effectively. Patients on these medications require careful evaluation of their overall health, including signs of infection, fever, or other symptoms, to determine if they are stable enough for discharge. The recovery process in these individuals may also be slower, necessitating a tailored post-discharge care plan.
Antibiotics, commonly used to treat infections, can also impact WBC counts and recovery. While they target bacteria, their effectiveness depends on the patient’s immune response, which is closely tied to WBC function. A WBC count of 16 in a patient on antibiotics might suggest improvement, but it is essential to ensure the infection is fully resolved. Premature discharge without confirming eradication of the infection could lead to relapse or complications. Healthcare providers should consider the duration of antibiotic therapy, the patient’s response, and any persistent symptoms before making a discharge decision.
Additionally, medications that affect the bone marrow, such as certain antipsychotics or anticonvulsants, can alter WBC counts indirectly. These drugs may disrupt the bone marrow’s ability to produce white blood cells, leading to fluctuations in counts. A WBC count of 16 in patients taking such medications may not accurately reflect their immune status. In these cases, a comprehensive assessment, including additional blood tests or clinical observations, is necessary to ensure the patient’s safety upon discharge. The recovery process may also be prolonged, requiring ongoing medical supervision and support.
Finally, it is important to consider the interplay between multiple medications and their cumulative effect on WBC counts and recovery. Polypharmacy, or the use of several medications simultaneously, can lead to complex interactions that influence white blood cell production, function, and recovery. Patients with a WBC count of 16 who are on multiple drugs should be evaluated holistically, taking into account their overall medication regimen and its potential impact on their immune system. Discharge decisions should prioritize the patient’s ability to recover safely, with appropriate follow-up care to monitor WBC counts and address any emerging issues. Understanding the role of medications in this context is essential for making informed decisions about hospital discharge and ensuring optimal patient outcomes.
Breastfeeding Newborns: How Often in the First Few Days?
You may want to see also
Explore related products




![]()
Doctor’s Discharge Criteria: Factors considered before releasing patients with elevated WBC
When considering whether to discharge a patient with an elevated white blood cell (WBC) count of 16, doctors follow a structured set of criteria to ensure patient safety and continuity of care. The decision is not based solely on the WBC count but rather on a comprehensive evaluation of the patient’s overall condition. A WBC count of 16 is mildly elevated, as the normal range is typically between 4,000 and 11,000 cells per microliter. However, the clinical context, such as the underlying cause of the elevation, the patient’s symptoms, and their response to treatment, plays a critical role in discharge decisions.
One of the primary factors doctors consider is the underlying cause of the elevated WBC count. For instance, a WBC of 16 could be due to a mild infection, inflammation, stress, or even a recent surgery. If the cause is identified and appropriately managed—such as a resolving infection with improving symptoms and stable vital signs—discharge may be considered. Conversely, if the elevation is due to a more serious condition, such as sepsis or leukemia, further hospitalization and treatment are likely necessary. Doctors will also assess whether the patient requires intravenous antibiotics or other in-hospital treatments that cannot be managed at home.
The patient’s clinical stability is another critical criterion. This includes evaluating vital signs (temperature, heart rate, blood pressure, and oxygen saturation), mental status, and overall well-being. If the patient is afebrile, hemodynamically stable, and showing signs of improvement, discharge may be appropriate. However, if the patient continues to exhibit symptoms like fever, chills, severe pain, or respiratory distress, further monitoring in the hospital is warranted. Additionally, doctors will consider the patient’s ability to manage their condition at home, including access to medications, follow-up care, and support systems.
Laboratory trends are also closely monitored. A single WBC count of 16 may not be as concerning if it is decreasing from a higher level, indicating resolution of the issue. Conversely, a rising WBC count, even if it starts at 16, could signal worsening infection or inflammation, necessitating continued hospitalization. Doctors may also review other lab results, such as inflammatory markers (e.g., CRP or procalcitonin), to assess the severity and progression of the condition.
Finally, follow-up care and patient education are essential components of the discharge decision. Before releasing a patient with an elevated WBC count, doctors ensure that the patient understands their diagnosis, treatment plan, and warning signs of deterioration. Arrangements for close follow-up with a primary care provider or specialist are made to monitor progress and adjust treatment as needed. If the patient lacks access to follow-up care or is unable to adhere to the treatment plan, discharge may be delayed until these issues are addressed.
In summary, discharging a patient with a WBC count of 16 involves a multifaceted assessment of the underlying cause, clinical stability, laboratory trends, and the availability of follow-up care. Doctors prioritize patient safety and ensure that all necessary conditions are met before releasing the patient from the hospital. If there is any uncertainty or concern, further observation and treatment in the hospital setting are preferred to mitigate risks and promote optimal recovery.
Hospitality Industry: My Career, My Calling
You may want to see also
Frequently asked questions
A WBC count of 16 is mildly elevated, but whether you should be released depends on your overall condition, symptoms, and the underlying cause of the elevation. Your doctor will assess if it’s safe for you to go home.
A WBC count of 16 is not inherently dangerous but indicates a possible infection, inflammation, or stress response. Your healthcare provider will determine if further treatment or monitoring is needed.
If you feel well and your doctor determines the elevation is not due to a serious condition, you may be discharged. However, follow-up care and monitoring are often recommended.
A WBC count of 16 can be caused by infections, inflammation, stress, certain medications, or underlying medical conditions. Your doctor will investigate the specific cause.
Antibiotics are only prescribed if the elevated WBC count is due to a bacterial infection. Your doctor will decide based on your symptoms, medical history, and additional tests.































