The question of whether a suicidal person should be hospitalized is a critical and complex issue that requires careful consideration of both ethical and medical factors. On one hand, hospitalization can provide a safe, supervised environment where individuals at risk of self-harm can receive immediate and intensive treatment, including therapy, medication, and crisis intervention. It also ensures they are monitored to prevent suicide attempts. However, involuntary hospitalization raises concerns about autonomy, stigma, and the potential for trauma, as it may alienate the individual or erode trust in mental health systems. Ultimately, the decision should be guided by a thorough assessment of the person’s risk level, their willingness to engage in treatment, and the availability of alternative support systems, always prioritizing their safety and well-being.
| Characteristics | Values |
|---|---|
| Severity of Suicidal Ideation | Hospitalization is recommended for individuals with active suicidal plans, intent, or means. |
| Immediate Risk | Those at high risk of acting on suicidal thoughts (e.g., access to lethal methods) should be hospitalized. |
| Previous Suicide Attempts | Individuals with a history of suicide attempts are more likely to be hospitalized. |
| Mental Health Diagnosis | Hospitalization is often considered for those with severe depression, bipolar disorder, schizophrenia, or other serious mental health conditions. |
| Support System | Lack of a strong support system or unsafe home environment may necessitate hospitalization. |
| Ability to Keep Safe | If the person cannot ensure their own safety, hospitalization is typically required. |
| Medical or Psychiatric Instability | Hospitalization is necessary for those with co-occurring medical issues or severe psychiatric symptoms. |
| Professional Assessment | A mental health professional’s evaluation is crucial in determining the need for hospitalization. |
| Voluntary vs. Involuntary Admission | Voluntary admission is preferred, but involuntary hospitalization may occur if the person is deemed an immediate danger to themselves. |
| Duration of Hospitalization | Typically short-term (days to weeks) to stabilize the individual and create a safety plan. |
| Alternative Options | Outpatient treatment, crisis intervention, or partial hospitalization may be considered if the risk is lower. |
| Legal and Ethical Considerations | Hospitalization must balance the individual’s rights with the duty to prevent harm. |
Explore related products






What You'll Learn
- Immediate Risk Assessment: Evaluates danger level to determine necessity of hospitalization for suicidal individuals
- Benefits of Hospitalization: Provides safety, monitoring, and intensive treatment for acute suicidal crises
- Alternatives to Hospitalization: Outpatient therapy, crisis lines, and support networks as potential options
- Ethical Considerations: Balancing autonomy, safety, and involuntary commitment in suicidal cases
- Long-Term Impact: Hospitalization’s effects on recovery, stigma, and future mental health outcomes
![]()
Immediate Risk Assessment: Evaluates danger level to determine necessity of hospitalization for suicidal individuals
Suicidal ideation demands immediate attention, and the decision to hospitalize hinges on a critical evaluation: the immediate risk assessment. This structured process quantifies the urgency of the situation, moving beyond vague concern to actionable intervention.
Identifying Red Flags: The Triage of Desperation
The assessment begins with a meticulous scan for red flags. These include recent suicide attempts, a specific plan with means and intent, access to lethal methods (e.g., firearms, stockpiled medication), and escalating hopelessness or agitation. A history of mental illness, substance abuse, or recent loss amplifies risk. For instance, a teenager with a detailed plan to overdose on a parent's prescription medication after a breakup presents a far higher immediate risk than someone expressing passive suicidal thoughts without a history of attempts.
The Columbia-Suicide Severity Rating Scale: A Structured Approach
Tools like the Columbia-Suicide Severity Rating Scale (C-SSRS) provide a standardized framework. This scale probes the severity of ideation, the presence of suicidal behavior, and the lethality of methods considered. Scoring systems within the C-SSRS help clinicians objectively gauge risk, ensuring consistency and reducing reliance on subjective judgment. A score indicating high risk, particularly when coupled with red flags, strongly suggests the need for hospitalization.
Beyond the Checklist: The Human Element
While structured tools are invaluable, the human element remains crucial. A skilled assessor observes nonverbal cues: flat affect, tearfulness, or a sense of detachment can signal profound despair. Active listening uncovers nuances in language – a shift from "I wish I weren't here" to "I have a way to end it all" demands immediate action.
Hospitalization: A Temporary Haven, Not a Permanent Solution
Hospitalization serves as a temporary sanctuary, providing a safe environment, intensive monitoring, and access to crisis intervention. It allows for medication adjustments, therapy initiation, and the development of a comprehensive safety plan. However, it's not a cure. The goal is stabilization, followed by a seamless transition to outpatient care, ensuring ongoing support and preventing future crises.
Is Southlake Hospital Affiliated with Orlando Health System?
You may want to see also
Explore related products

$33.49 $70.95





![]()
Benefits of Hospitalization: Provides safety, monitoring, and intensive treatment for acute suicidal crises
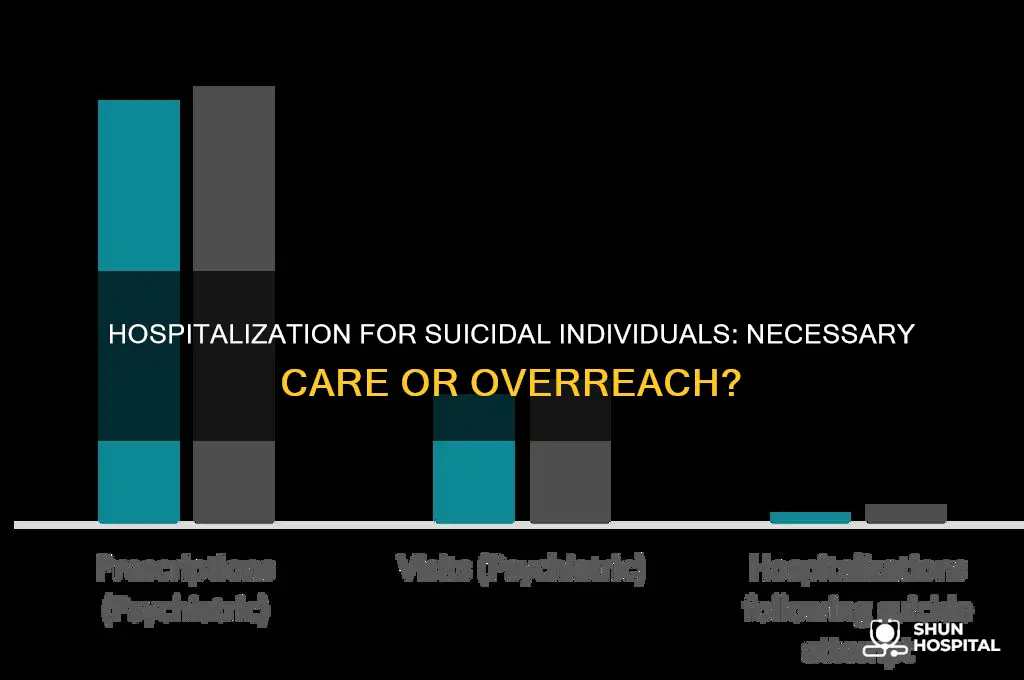
Hospitalization for suicidal individuals serves as a critical intervention, offering a structured environment where safety is prioritized. In acute crises, the risk of self-harm is highest, and home settings often lack the necessary safeguards. Hospitals, by contrast, are designed to minimize access to lethal means, from sharp objects to medications, reducing the immediate danger. For instance, a study published in the *Journal of Clinical Psychiatry* found that hospitalized patients experienced a 50% reduction in suicide attempts during their stay compared to those managed outpatient. This controlled setting acts as a physical barrier against impulsive actions, providing a crucial window for stabilization.
Monitoring in a hospital setting goes beyond occasional check-ins; it involves continuous observation by trained professionals. Suicidal individuals often struggle with volatile emotions and unpredictable behavior, making 24/7 supervision essential. For example, psychiatric units frequently employ "line-of-sight" monitoring for high-risk patients, ensuring staff can intervene at the first sign of distress. This level of vigilance is impossible to replicate at home, even with supportive family members. Additionally, vital signs, sleep patterns, and medication adherence are tracked, allowing for real-time adjustments to care plans. Such meticulous oversight can prevent escalation and provide data-driven insights into the patient’s condition.
Intensive treatment in a hospital setting offers a concentrated approach to addressing suicidal crises. Unlike outpatient care, which may involve weekly therapy sessions, hospitalization provides daily access to psychiatrists, psychologists, and specialized therapies. Evidence-based modalities like dialectical behavior therapy (DBT) or cognitive-behavioral therapy (CBT) are often delivered in group and individual formats, accelerating progress. Medication management is another key component; hospital stays allow for rapid titration of antidepressants or mood stabilizers, with some studies showing symptom improvement within 7–10 days of optimized pharmacotherapy. This immersive treatment model can disrupt suicidal ideation patterns and equip individuals with coping strategies before discharge.
A comparative analysis highlights the advantages of hospitalization over alternative interventions. While crisis hotlines and outpatient therapy play vital roles, they are limited in their ability to address acute, life-threatening situations. For example, a person in the throes of a suicidal crisis may be unable to engage meaningfully in a phone conversation or wait weeks for therapy appointments. Hospitalization bridges this gap by offering immediate, comprehensive care. It also serves as a transitional step, stabilizing patients before connecting them with long-term resources like partial hospitalization programs or community support groups. This continuum of care ensures that the benefits of hospitalization extend beyond the hospital walls.
Practical considerations underscore the value of hospitalization. For families and caregivers, knowing a loved one is in a safe, supervised environment can alleviate immense stress and fear. Hospitals also provide education on recognizing warning signs and preventing future crises, empowering caregivers to act proactively. For patients, hospitalization can be a turning point, offering a sense of hope and a structured path forward. While the decision to hospitalize is never taken lightly, its potential to save lives and foster recovery is undeniable. In acute suicidal crises, it remains one of the most effective tools available.
Hospital Volunteering: A Transformative Step Toward Medical School Success
You may want to see also
Explore related products






![]()
Alternatives to Hospitalization: Outpatient therapy, crisis lines, and support networks as potential options
Hospitalization isn’t the only path for someone experiencing suicidal thoughts. Outpatient therapy, crisis lines, and support networks offer viable alternatives, each addressing different needs and stages of crisis. For instance, outpatient therapy provides structured, long-term care, while crisis lines offer immediate, anonymous support. Understanding these options empowers individuals and their loved ones to make informed decisions tailored to the severity and context of the situation.
Outpatient therapy stands as a cornerstone for sustained mental health management. Cognitive Behavioral Therapy (CBT) and Dialectical Behavior Therapy (DBT) are evidence-based approaches proven to reduce suicidal ideation. CBT focuses on reframing negative thought patterns, while DBT emphasizes emotional regulation and distress tolerance. Sessions typically last 45–60 minutes, occurring weekly or biweekly. For adolescents, family therapy can be integrated to address systemic issues. Unlike hospitalization, outpatient therapy allows individuals to maintain daily routines, fostering a sense of normalcy and control. However, it’s less suited for acute crises where immediate intervention is critical.
Crisis lines serve as a lifeline during moments of intense distress. Services like the National Suicide Prevention Lifeline (988 in the U.S.) provide 24/7 access to trained counselors who can de-escalate crises and connect callers to local resources. Text-based options, such as Crisis Text Line (text 741741), cater to those uncomfortable with voice calls. These services are anonymous, free, and require no prior appointment, making them accessible even to those without a support system. While not a substitute for long-term care, crisis lines can stabilize individuals until they can access further help. A key limitation is their reliance on the individual’s willingness to reach out.
Support networks—friends, family, and community groups—play a crucial role in preventing isolation. Peer support groups, such as those offered by the American Foundation for Suicide Prevention, provide a sense of belonging and shared understanding. For families, education on recognizing warning signs and effective communication can transform them into active allies. Apps like *Sanvello* or *7 Cups* complement these networks by offering digital communities and tools for self-management. However, reliance on informal support alone can be risky if professional help is needed but not sought. Balancing personal connections with structured care is essential.
In practice, these alternatives often work best in combination. For example, someone might use a crisis line during an acute episode, begin outpatient therapy for ongoing treatment, and lean on a support network for daily encouragement. The key is assessing the individual’s needs—severity of ideation, presence of a safety plan, and access to resources—to determine the most effective approach. While hospitalization remains necessary in some cases, these alternatives offer flexibility, dignity, and continuity of care for many.
LeBron James' Birthplace: A Hospital's Claim to Fame
You may want to see also
Explore related products





![]()
Ethical Considerations: Balancing autonomy, safety, and involuntary commitment in suicidal cases
Suicidal ideation presents a complex ethical dilemma: how do we respect an individual’s autonomy while ensuring their safety? Involuntary hospitalization, often framed as a protective measure, raises questions about coercion, human rights, and the potential for harm. A 2021 study in *JAMA Psychiatry* found that while short-term hospitalization can reduce immediate risk, it may also lead to feelings of betrayal and decreased trust in mental health systems, particularly among marginalized groups. This tension underscores the need for a nuanced approach that balances immediate risk mitigation with long-term psychological well-being.
Consider the case of a 28-year-old with a history of depression who expresses suicidal thoughts but insists they do not want hospitalization. Clinicians must weigh the legal and ethical frameworks guiding involuntary commitment, such as the "duty to protect" and the "least restrictive alternative" principle. For instance, in the U.S., many states require evidence of an imminent threat before hospitalization can be mandated. However, "imminent" is subjective, leaving room for misinterpretation. A 2019 review in *Ethics & Behavior* highlights that such decisions often disproportionately affect individuals with limited access to outpatient resources, exacerbating existing inequalities.
To navigate this, a stepwise approach can be instructive. First, assess the individual’s capacity for decision-making using tools like the MacArthur Competence Assessment Tool for Treatment (MacCAT-T). If capacity is intact, explore alternatives to hospitalization, such as intensive outpatient programs or crisis stabilization units. Second, involve the individual in the decision-making process, fostering collaboration rather than coercion. For example, a safety plan co-created with the patient can include emergency contacts, coping strategies, and clear steps to take if risk escalates. Third, document the rationale for any involuntary measures transparently, ensuring accountability and minimizing legal risks.
Caution must be exercised to avoid over-reliance on hospitalization as a default solution. Research indicates that involuntary commitment can lead to trauma, particularly for those with prior adverse experiences in healthcare settings. A 2020 study in *The Lancet Psychiatry* found that 40% of patients reported feeling more suicidal after involuntary hospitalization due to feelings of powerlessness. Additionally, cultural and socioeconomic factors must be considered; for instance, Indigenous communities may view hospitalization as a disruption of familial and cultural support systems, which are critical to healing.
In conclusion, balancing autonomy, safety, and involuntary commitment requires a context-specific, patient-centered approach. While hospitalization can be lifesaving in acute cases, it should not overshadow the importance of preserving trust and dignity. By prioritizing collaboration, exploring less restrictive options, and addressing systemic inequities, clinicians can navigate this ethical minefield more effectively. The ultimate goal is not just to prevent immediate harm but to foster resilience and hope in a way that respects the individual’s humanity.
Hospitality Room Essentials: A Complete Guide
You may want to see also
Explore related products





![]()
Long-Term Impact: Hospitalization’s effects on recovery, stigma, and future mental health outcomes
Hospitalization for suicidal ideation can be a double-edged sword, offering immediate safety but potentially shaping long-term mental health trajectories in complex ways. While the acute benefits of stabilization are clear, the impact on recovery, stigma, and future outcomes demands careful consideration. Research suggests that involuntary hospitalization, in particular, can leave lasting psychological scars, with some individuals reporting feelings of betrayal, loss of autonomy, and heightened anxiety about future crises. This raises a critical question: how can we balance the need for protection with the potential for long-term harm?
Consider the case of a 28-year-old who, after a brief hospitalization, describes feeling "like a broken record" when seeking outpatient care. "Every therapist I see now treats me like I’m one step away from the edge," they explain. This example illustrates how hospitalization can inadvertently stigmatize individuals, framing them as perpetually high-risk rather than focusing on their resilience and recovery potential. Such stigma can deter future help-seeking, as individuals fear being labeled or treated solely through the lens of their past crisis. Clinicians must actively counter this by emphasizing strengths-based approaches and avoiding over-reliance on diagnostic histories.
From a recovery-oriented perspective, hospitalization should serve as a springboard, not a defining moment. A study in *Psychiatric Services* found that patients who received post-discharge follow-up within 7 days were 30% less likely to reattempt suicide within a year. This highlights the importance of structured aftercare, such as partial hospitalization programs or peer support groups, which can mitigate the isolating effects of hospitalization. Practical steps include ensuring a "warm handoff" between inpatient and outpatient providers, involving the individual in discharge planning, and providing concrete resources like crisis hotlines or app-based coping tools.
However, the long-term impact isn’t solely negative. For some, hospitalization marks a turning point, offering access to intensive treatment modalities like dialectical behavior therapy (DBT) or medication adjustments that stabilize symptoms. A 35-year-old participant in a qualitative study noted, "Being hospitalized forced me to confront my avoidance. It wasn’t pleasant, but it was necessary." This underscores the importance of individualizing care, recognizing that what feels punitive to one person may be transformative for another. Clinicians should assess not only the immediate risk but also the individual’s perceived needs, cultural background, and prior experiences with the mental health system.
Ultimately, the long-term effects of hospitalization hinge on how it’s framed and followed up. Viewing it as a temporary intervention rather than a failure of coping can shift the narrative from shame to resilience. Providers must also address systemic issues, such as the lack of step-down services or the financial burden of repeated hospitalizations, which disproportionately affect marginalized communities. By reframing hospitalization as one tool within a broader continuum of care, we can minimize stigma and maximize its potential to foster sustained recovery.
Outpatient Care Location at Memorial Hospital Hollywood: A Quick Guide
You may want to see also
Frequently asked questions
Not always. Hospitalization depends on the severity of the risk, the person's support system, and their willingness to engage in treatment. A mental health professional should assess the situation to determine the best course of action.
Hospitalization provides a safe, supervised environment, immediate access to mental health professionals, and intensive treatment, including therapy and medication, to stabilize the individual during a crisis.
Yes, if the risk is low and the person has a strong support system, outpatient treatment, such as therapy, medication, and crisis hotlines, may be sufficient. Regular monitoring by a mental health professional is essential.
The duration varies based on the individual's needs, but it often ranges from a few days to a couple of weeks. The goal is to stabilize the person and create a safety plan before discharge.
After discharge, a comprehensive aftercare plan is crucial. This may include ongoing therapy, medication management, support groups, and regular check-ins with mental health professionals to prevent relapse.































