The question of whether hospitals were overrun is a critical one, particularly in the context of global health crises such as pandemics or large-scale emergencies. During such events, healthcare systems often face unprecedented challenges, including a surge in patient numbers, shortages of medical supplies, and overwhelmed staff. The COVID-19 pandemic, for instance, highlighted the fragility of many healthcare infrastructures worldwide, as hospitals in numerous countries struggled to cope with the influx of critically ill patients. This situation not only strained resources but also raised concerns about the quality of care and the safety of both patients and healthcare workers. Understanding the factors that contribute to hospitals becoming overrun and identifying strategies to mitigate these issues are essential for improving resilience in healthcare systems and ensuring preparedness for future crises.
| Characteristics | Values |
|---|---|
| Were hospitals overrun during the COVID-19 pandemic? | In many regions, yes, especially during peak waves. |
| Factors contributing to hospital overload | High infection rates, limited ICU beds, staffing shortages, lack of medical supplies. |
| Regions most affected | Vary by wave and vaccination rates; early hotspots included Italy, New York City, and India. |
| Impact on non-COVID care | Delayed elective surgeries, reduced access to emergency services, and postponed treatments. |
| Mitigation measures | Increased hospital capacity, field hospitals, vaccination campaigns, public health restrictions. |
| Current status (as of latest data) | Improved in many areas due to vaccinations and better treatments, but still a risk during surges. |
| Long-term effects on healthcare systems | Strained resources, burnout among healthcare workers, and increased healthcare costs. |
| Data sources | WHO, CDC, national health departments, peer-reviewed studies. |
Explore related products






What You'll Learn
- Staff Shortages and Burnout: Overworked healthcare workers, insufficient staffing, and mental health crises among medical professionals
- Patient Overflow and Triage: Limited beds, delayed treatments, and difficult decisions on prioritizing patient care
- Supply Chain Disruptions: Shortages of critical medical supplies, equipment, and medications impacting patient care
- Infection Control Challenges: Overcrowding leading to increased risk of infections and disease spread within hospitals
- Financial Strain on Hospitals: Rising costs, reduced revenue, and budget cuts affecting hospital operations and resources
![]()
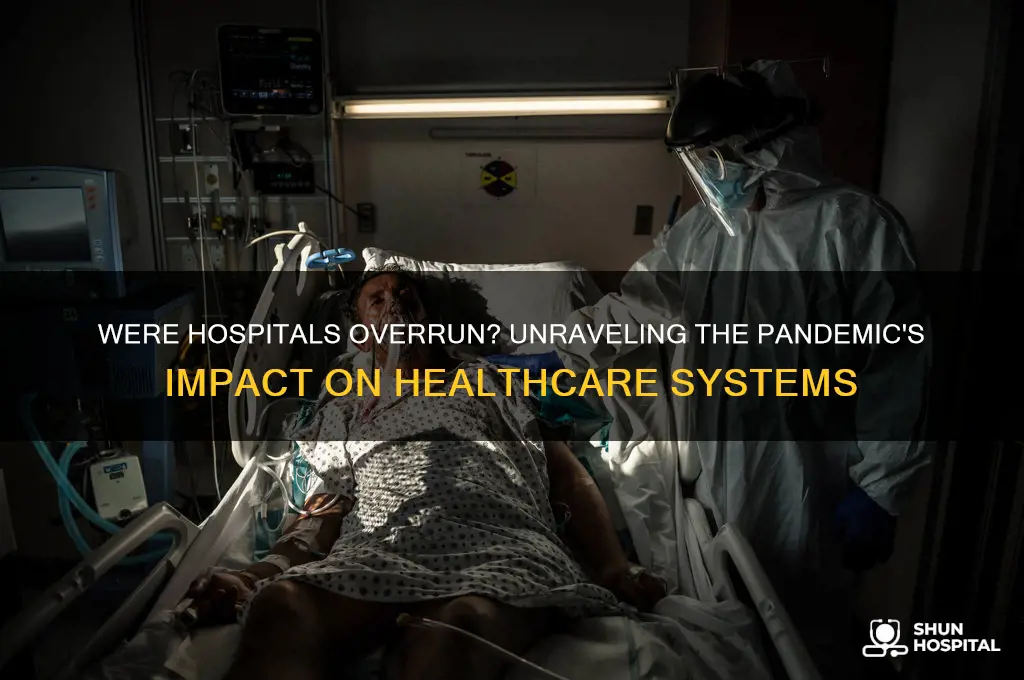
Staff Shortages and Burnout: Overworked healthcare workers, insufficient staffing, and mental health crises among medical professionals
The COVID-19 pandemic exposed a harsh reality: healthcare systems globally were ill-prepared for the surge in patients, and at the heart of this crisis were the overworked and understaffed medical professionals. Staff shortages in hospitals were not merely a logistical issue but a critical factor contributing to the overwhelming strain on healthcare services. As patient numbers skyrocketed, the existing staffing gaps widened, leaving an already exhausted workforce struggling to cope.
The Perfect Storm of Staff Shortages
Imagine a hospital ward where nurses are responsible for twice the number of patients they can safely manage. This scenario became a daily reality during the pandemic's peak. Staff shortages in healthcare are not a new phenomenon, but the crisis exacerbated an already fragile situation. According to a 2021 report by the World Health Organization (WHO), the global health workforce shortage was estimated to be around 18 million, with the most significant gaps in low- and lower-middle-income countries. When the pandemic hit, this shortage became a critical vulnerability. For instance, in the United States, hospitals in rural areas often operate with minimal staff, and when COVID-19 cases surged, these facilities were quickly overwhelmed, forcing them to transfer patients to already burdened urban hospitals.
Burnout: A Silent Epidemic Among Healthcare Heroes
The consequences of insufficient staffing extend far beyond delayed patient care. Overworked healthcare professionals faced unprecedented levels of stress and burnout. A study published in the *Journal of the American Medical Association* (JAMA) revealed that during the pandemic, the prevalence of burnout among healthcare workers increased significantly, with rates as high as 60% in some countries. This burnout crisis is not just about long hours; it's a complex issue involving emotional exhaustion, depersonalization, and a sense of diminished personal accomplishment. For instance, a nurse working 12-hour shifts, day after day, witnessing the suffering and death of patients without adequate support, is at high risk of developing severe mental health issues.
Addressing the Crisis: Practical Solutions
To combat staff shortages and burnout, a multi-faceted approach is necessary. Firstly, healthcare facilities should focus on workforce retention by offering competitive salaries, flexible schedules, and comprehensive mental health support programs. For instance, implementing a 'buddy system' where experienced staff mentor and support newer colleagues can foster a sense of community and provide an outlet for stress. Additionally, hospitals can explore innovative staffing models, such as hiring traveling nurses or utilizing telemedicine to alleviate the burden on physical resources.
Another crucial step is to invest in technology that streamlines administrative tasks, reducing the time nurses and doctors spend on paperwork. This could include implementing efficient electronic health record systems and automated appointment scheduling. By freeing up time, healthcare professionals can focus more on patient care and less on bureaucratic tasks, potentially reducing burnout.
A Call to Action
The issue of staff shortages and burnout in healthcare is not one that can be resolved overnight, but it demands immediate attention and long-term strategic planning. Governments and healthcare administrators must work together to address the root causes, ensuring that the workforce is adequately sized, well-supported, and equipped with the necessary resources. By prioritizing the well-being of healthcare workers, we not only improve the quality of patient care but also build a more resilient healthcare system capable of withstanding future crises. This involves a cultural shift, recognizing that the health of our healthcare providers is integral to the health of our communities.
Is Wage Garnishment Legal for Mississippi Hospital Debt? Know Your Rights
You may want to see also
Explore related products






![]()
Patient Overflow and Triage: Limited beds, delayed treatments, and difficult decisions on prioritizing patient care
During the peak of the COVID-19 pandemic, hospitals worldwide faced unprecedented patient surges, with some facilities reporting occupancy rates exceeding 150% of their normal capacity. This crisis highlighted the fragility of healthcare systems when demand outstrips resources. Limited beds became the bottleneck, forcing hospitals to convert cafeterias, parking lots, and even conference rooms into makeshift wards. In New York City, for instance, the Javits Center was repurposed as a 2,500-bed hospital to alleviate the strain on local facilities. Despite such efforts, the lack of physical space often meant patients waited in emergency departments for hours, sometimes days, before admission.
Triage, the process of prioritizing patients based on the severity of their condition, became a high-stakes endeavor. Clinicians were forced to make ethically fraught decisions, such as allocating ventilators to patients with higher survival odds. For example, in Italy, hospitals adopted age-based triage protocols, prioritizing younger patients due to their perceived higher chances of recovery. This approach, while controversial, underscored the grim reality of resource scarcity. Meanwhile, delayed treatments for non-COVID conditions, such as cancer surgeries and stroke interventions, led to worsened outcomes for millions. A 2021 study in *The Lancet* estimated that disruptions in healthcare services during the pandemic could result in over 1 million additional deaths globally from preventable diseases.
To manage patient overflow, hospitals implemented creative solutions, though not without challenges. Some facilities adopted "cohorting," grouping COVID-19 patients together to optimize staff and equipment use. Others leaned on telemedicine to triage patients remotely, reducing the burden on physical infrastructure. However, these measures were often reactive rather than preventive. For instance, while telemedicine effectively screened mild cases, it could not address the needs of critically ill patients requiring intensive care. The reliance on such stopgap solutions exposed systemic vulnerabilities, particularly in underfunded healthcare systems.
Moving forward, hospitals must adopt proactive strategies to mitigate future crises. Increasing surge capacity through modular construction and cross-training staff for multiple roles can enhance resilience. Policymakers should invest in data-driven models to predict patient influxes, allowing for better resource allocation. For example, the UK’s National Health Service (NHS) uses real-time data analytics to monitor bed occupancy and redirect patients to less congested facilities. Additionally, ethical frameworks for triage decisions must be developed collaboratively, involving clinicians, ethicists, and the public to ensure transparency and fairness.
Ultimately, the lessons from overwhelmed hospitals during the pandemic serve as a stark reminder of the need for robust healthcare infrastructure. While temporary fixes like makeshift wards and telemedicine played a role, they are no substitute for long-term investments in beds, equipment, and personnel. Addressing patient overflow and triage challenges requires a multifaceted approach—one that balances immediate crisis management with sustainable system-wide reforms. Without such measures, hospitals risk being ill-prepared for the next wave of patients, whether from pandemics, natural disasters, or other emergencies.
Medicare Hospital Stays: How Many Days Are Covered?
You may want to see also
Explore related products





![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)
![]()
Supply Chain Disruptions: Shortages of critical medical supplies, equipment, and medications impacting patient care
The COVID-19 pandemic exposed a fragile global supply chain, leaving hospitals worldwide scrambling for essential medical supplies. Personal protective equipment ( PPE) like N95 masks, gowns, and gloves became as precious as gold, with prices skyrocketing and shortages forcing healthcare workers to reuse equipment meant for single-use. This wasn't just about discomfort; it directly impacted patient care. Imagine a scenario where a nurse, lacking proper PPE, hesitates to enter a patient's room for fear of infection, delaying critical treatment.
A 2020 survey by the American Hospital Association revealed that 90% of hospitals faced shortages of critical supplies, including ventilators, crucial for treating severe COVID-19 cases. This meant difficult decisions about rationing care, prioritizing patients based on their chances of survival.
The ripple effects extended beyond PPE and ventilators. Shortages of medications like propofol, a common anesthetic used in intubation, and midazolam, a sedative, further complicated treatment. Imagine a surgeon unable to perform a life-saving procedure due to a lack of essential drugs. This wasn't a hypothetical scenario; it was a stark reality for many hospitals during the pandemic's peak.
The pandemic highlighted the interconnectedness of global supply chains. A disruption in one region, like a factory closure in China, could have devastating consequences for hospitals thousands of miles away. This vulnerability demands a rethinking of our approach to medical supply chains.
Building resilience requires a multi-pronged strategy. Firstly, diversifying supply sources is crucial. Relying on a single country or region for critical supplies leaves healthcare systems vulnerable. Secondly, investing in domestic manufacturing capabilities can reduce reliance on foreign suppliers and ensure a more stable supply chain. Finally, establishing strategic stockpiles of essential medications and equipment can provide a buffer during emergencies.
Exploring China's Extensive Hospital Network
You may want to see also
Explore related products
![Pandemic [DVD]](https://m.media-amazon.com/images/I/91ynbSGeZVS._AC_UL320_.jpg)

![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)

![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)

![]()
Infection Control Challenges: Overcrowding leading to increased risk of infections and disease spread within hospitals
Overcrowding in hospitals has emerged as a critical factor exacerbating infection control challenges, particularly during public health crises like pandemics. When patient volumes surpass a facility’s capacity, isolation protocols become nearly impossible to maintain. For instance, during the COVID-19 surge in 2020, hospitals in New York City reported occupancy rates exceeding 120%, forcing staff to place infectious patients in shared spaces. This proximity accelerates the spread of pathogens, not only among patients but also to healthcare workers, who then risk becoming vectors themselves. The World Health Organization (WHO) highlights that overcrowded wards can increase the risk of healthcare-associated infections (HAIs) by up to 30%, underscoring the urgency of addressing this issue.
To mitigate the risks of overcrowding, hospitals must implement strategic measures that balance patient care with infection control. One effective approach is cohorting, where patients with similar infections are grouped together to minimize cross-contamination. For example, during the H1N1 pandemic, hospitals in Mexico designated specific wards for influenza patients, reducing transmission rates by 25%. Additionally, increasing hand hygiene compliance among staff and visitors is non-negotiable. Studies show that adherence to hand hygiene protocols can decrease HAI rates by 40%. Practical tips include placing hand sanitizer dispensers at every patient bedside and conducting regular audits to ensure compliance.
However, overcrowding isn’t solely a logistical issue—it’s also a resource problem. Insufficient staffing levels compound the challenge, as overworked healthcare providers are more likely to make errors that facilitate infection spread. For instance, a study in the *Journal of Hospital Infection* found that nurses caring for more than four patients at a time were 70% more likely to skip infection control procedures. Hospitals must prioritize staffing ratios, ensuring that each patient receives adequate attention. Temporary solutions, such as hiring travel nurses or redeploying administrative staff to clinical roles, can provide immediate relief during surges.
Comparatively, hospitals in countries with robust healthcare infrastructure, like Germany and Japan, have fared better in managing overcrowding during crises. These nations invest in surge capacity planning, including modular hospitals and telemedicine, to divert non-critical cases. For example, Germany’s use of telemedicine reduced hospital visits by 40% during peak COVID-19 periods, alleviating pressure on physical facilities. Developing nations can adopt similar strategies by partnering with tech companies to implement remote consultation platforms, which not only reduce overcrowding but also improve access to care.
Ultimately, addressing overcrowding requires a multifaceted approach that combines immediate interventions with long-term systemic changes. Hospitals must invest in infrastructure expansions, such as increasing bed capacity and building isolation units, while also adopting digital tools to optimize patient flow. Policymakers play a crucial role by allocating funds for healthcare preparedness and enforcing regulations that ensure hospitals maintain safe occupancy levels. Without these measures, overcrowding will remain a persistent threat, undermining infection control efforts and endangering both patients and healthcare workers.
Exploring Minnesota's Small Town Hospitals: A Comprehensive Count and Overview
You may want to see also
Explore related products
![Pandemic Pandemic [DVD]](https://m.media-amazon.com/images/I/81dZDU9gUpL._AC_UL320_.jpg)


![Pandemic [ NON-USA FORMAT, PAL, Reg.2 Import - Netherlands ]](https://m.media-amazon.com/images/I/51diyJBw2mS._AC_UL320_.jpg)

![Pandemic [Blu-ray]](https://m.media-amazon.com/images/I/61EbhmkB1tS._AC_UL320_.jpg)
![]()
Financial Strain on Hospitals: Rising costs, reduced revenue, and budget cuts affecting hospital operations and resources
Hospitals, once seen as bastions of financial stability, are increasingly finding themselves in a precarious position. The rising costs of medical supplies, equipment, and labor have outpaced revenue growth, creating a widening gap that threatens their ability to operate effectively. For instance, the cost of personal protective equipment (PPE) skyrocketed during the COVID-19 pandemic, with some hospitals reporting a 1,000% increase in expenses for items like N95 masks and gloves. This surge in costs, coupled with the need to maintain outdated infrastructure, has left many institutions struggling to balance their budgets.
Consider the case of rural hospitals, which often operate on thinner margins than their urban counterparts. These facilities frequently serve older populations with higher rates of chronic conditions, requiring more resources per patient. When budget cuts force them to reduce staff or eliminate services, the consequences can be dire. For example, a rural hospital in the Midwest was forced to close its obstetrics unit due to financial constraints, leaving expectant mothers with limited options for prenatal and postnatal care. This not only affects patient outcomes but also exacerbates healthcare disparities in underserved communities.
To mitigate financial strain, hospitals must adopt strategic cost-saving measures without compromising care quality. One effective approach is implementing value-based care models, which prioritize patient outcomes over the volume of services provided. For instance, a hospital in California reduced readmission rates by 20% by introducing a transitional care program for high-risk patients, saving approximately $2 million annually. Additionally, leveraging technology, such as telemedicine and electronic health records, can streamline operations and reduce administrative costs. However, hospitals must proceed cautiously, as over-reliance on technology can lead to depersonalized care and increased burnout among healthcare workers.
A comparative analysis reveals that hospitals in countries with universal healthcare systems often face fewer financial challenges due to consistent funding streams. In contrast, U.S. hospitals, which rely heavily on private insurance and out-of-pocket payments, are more vulnerable to revenue fluctuations. For example, during the pandemic, elective procedure cancellations resulted in a 50% drop in revenue for some U.S. hospitals, while European hospitals experienced minimal financial impact due to government subsidies. This highlights the need for policy reforms that stabilize hospital funding and reduce dependency on unpredictable revenue sources.
Finally, addressing the financial strain on hospitals requires a multifaceted approach involving stakeholders at all levels. Hospital administrators must advocate for increased government funding and explore partnerships with private organizations to secure additional resources. Policymakers should prioritize legislation that caps the cost of essential medical supplies and incentivizes investment in rural healthcare. Patients can also play a role by staying informed about their healthcare options and supporting initiatives that strengthen hospital sustainability. By working together, we can ensure that hospitals remain equipped to meet the needs of their communities, even in the face of mounting financial pressures.
Hospital Management MBA: Your Career Guide
You may want to see also
Frequently asked questions
Yes, many hospitals worldwide were severely overwhelmed during the peak of the COVID-19 pandemic due to a surge in patients requiring critical care, shortages of medical staff, and limited resources like ventilators and ICU beds.
Hospitals often become overrun due to a combination of factors, including a sudden influx of patients, insufficient healthcare infrastructure, staffing shortages, and limited supplies of essential medical equipment.
Yes, during the 1918 Spanish Flu pandemic, hospitals were frequently overrun as the rapid spread of the virus led to a massive increase in patients, overwhelming medical facilities that were already strained by World War I.



![Pandemic [DVD] [UK Import]](https://m.media-amazon.com/images/I/61az7jpPZ+L._AC_UL320_.jpg)