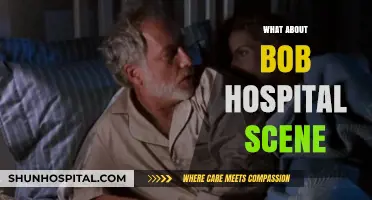
The question of whether New York hospitals were overrun during the peak of the COVID-19 pandemic remains a critical point of discussion, reflecting the unprecedented strain placed on the city's healthcare system. As the epicenter of the outbreak in the United States, New York faced an overwhelming surge in cases, leading to a dire shortage of medical resources, including hospital beds, ventilators, and personal protective equipment (PPE). Hospitals were forced to rapidly expand capacity, convert non-medical spaces into makeshift wards, and rely on emergency staffing measures to manage the influx of patients. The crisis highlighted both the resilience of healthcare workers and the vulnerabilities within the system, sparking debates about preparedness, resource allocation, and the long-term implications for public health infrastructure.
| Characteristics | Values |
|---|---|
| Timeframe | March-April 2020 (peak of COVID-19 first wave in New York) |
| Hospital Capacity | Hospitals were severely strained, with ICU beds nearing full capacity. |
| Patient Surge | Over 12,000 COVID-19 hospitalizations at the peak (early April 2020). |
| Staffing Challenges | Shortages of healthcare workers due to illness and overwhelming caseloads. |
| PPE Shortages | Critical shortages of personal protective equipment (PPE) reported. |
| Field Hospitals | Temporary field hospitals and facilities (e.g., Javits Center) were set up. |
| Mortality Rate | High mortality rates among hospitalized patients, especially in ICUs. |
| Government Response | Statewide mandates for hospitals to increase capacity by 50%. |
| Public Perception | Widespread concern about hospital capacity and healthcare system collapse. |
| Long-term Impact | Hospitals faced financial strain and long-term recovery challenges. |
| Latest Status (as of 2023) | Hospitals have recovered, with improved capacity and preparedness. |
Explore related products





What You'll Learn
![]()
Staff Shortages and Burnout
During the peak of the COVID-19 pandemic, New York City’s hospitals faced unprecedented strain, with staff shortages and burnout emerging as critical challenges. As patient volumes surged, healthcare workers were forced to operate under conditions that stretched their physical and mental limits. The sudden influx of critically ill patients, combined with inadequate staffing levels, created a perfect storm for exhaustion and disillusionment among medical professionals. This crisis highlighted not only the immediate need for more hands on deck but also the long-term consequences of neglecting workforce sustainability in healthcare.
Consider the numbers: at the height of the pandemic, some New York hospitals reported operating with up to 30% of their staff out sick or in quarantine. This left remaining workers to cover longer shifts, often without sufficient breaks, while managing life-and-death decisions daily. Burnout became inevitable, with symptoms like emotional exhaustion, depersonalization, and reduced personal accomplishment reported by over 50% of surveyed healthcare workers in NYC during this period. The psychological toll was compounded by the lack of adequate personal protective equipment (PPE) and the constant fear of infection, both for themselves and their families.
To address staff shortages, hospitals implemented stopgap measures, such as redeploying administrative staff to clinical roles and recruiting retired nurses and medical students. While these steps provided temporary relief, they were not sustainable solutions. For instance, medical students, though eager to help, lacked the experience to handle complex COVID-19 cases independently, placing additional strain on senior staff. Similarly, retired nurses, while valuable, faced increased health risks due to their age, limiting their ability to work in high-exposure environments.
Preventing burnout requires a multi-faceted approach. Hospitals must prioritize mental health support by offering access to counseling services, peer support groups, and stress management programs. Practical measures, such as ensuring adequate staffing ratios and enforcing mandatory rest periods, are equally essential. For example, capping shifts at 12 hours and mandating a minimum of 8 hours off between shifts can help mitigate fatigue. Additionally, providing clear communication about hospital policies and resources can reduce anxiety and foster a sense of security among staff.
The lessons from New York’s experience are clear: healthcare systems must invest in their workforce proactively, not just reactively. This includes addressing systemic issues like competitive wages, career advancement opportunities, and safe working conditions. By doing so, hospitals can build resilience against future crises and ensure that their staff remain capable of delivering high-quality care, even under the most challenging circumstances. Ignoring these issues risks not only the well-being of healthcare workers but also the overall stability of the healthcare system.
University of Utah Hospital: Accepted Insurance Plans Explained
You may want to see also
Explore related products






![]()
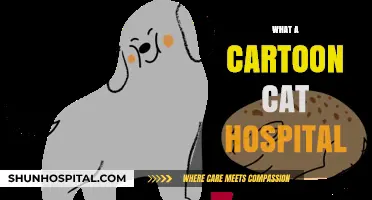
Patient Surge and Capacity Limits
During the peak of the COVID-19 pandemic, New York City’s hospitals faced an unprecedented patient surge that pushed their capacity limits to the brink. Emergency departments saw a 300% increase in admissions, with some facilities reporting up to 500 intubations per week—far exceeding their pre-pandemic averages of 50–70. This influx forced hospitals to convert cafeterias, lobbies, and even parking garages into makeshift ICUs, while staff worked 12–16 hour shifts to meet demand. The crisis highlighted a critical gap: most hospitals operate at 85–90% capacity under normal conditions, leaving little buffer for sudden spikes.
To manage such surges, hospitals must adopt scalable triage protocols. For instance, implementing a tiered system where patients are categorized by acuity (e.g., critical, urgent, stable) ensures resources are allocated efficiently. Staff should be cross-trained to handle multiple roles, and non-essential procedures should be deferred to free up beds and personnel. A practical tip: establish partnerships with local clinics or telemedicine providers to offload non-critical cases, reducing ER congestion.
A comparative analysis of New York’s response versus Italy’s Lombardy region reveals the importance of early resource reallocation. Lombardy, which faced a similar surge, saw mortality rates double due to delayed decisions on bed expansion and ventilator distribution. New York’s rapid deployment of field hospitals (e.g., the Javits Center) and national guard support mitigated some strain, though staffing shortages remained a bottleneck. This underscores the need for regional healthcare networks to share resources dynamically during crises.
Finally, long-term solutions require investment in surge capacity infrastructure. Hospitals should maintain stockpiles of critical supplies (e.g., ventilators, PPE) and develop modular spaces that can be quickly converted during emergencies. Policymakers must also address staffing shortages by incentivizing healthcare careers and creating reserve pools of retired or part-time workers. Without these measures, even the most advanced healthcare systems risk being overrun when faced with sudden, large-scale crises.
Mercer's Contagion Risk: Hospitals on High Alert
You may want to see also
Explore related products






![]()
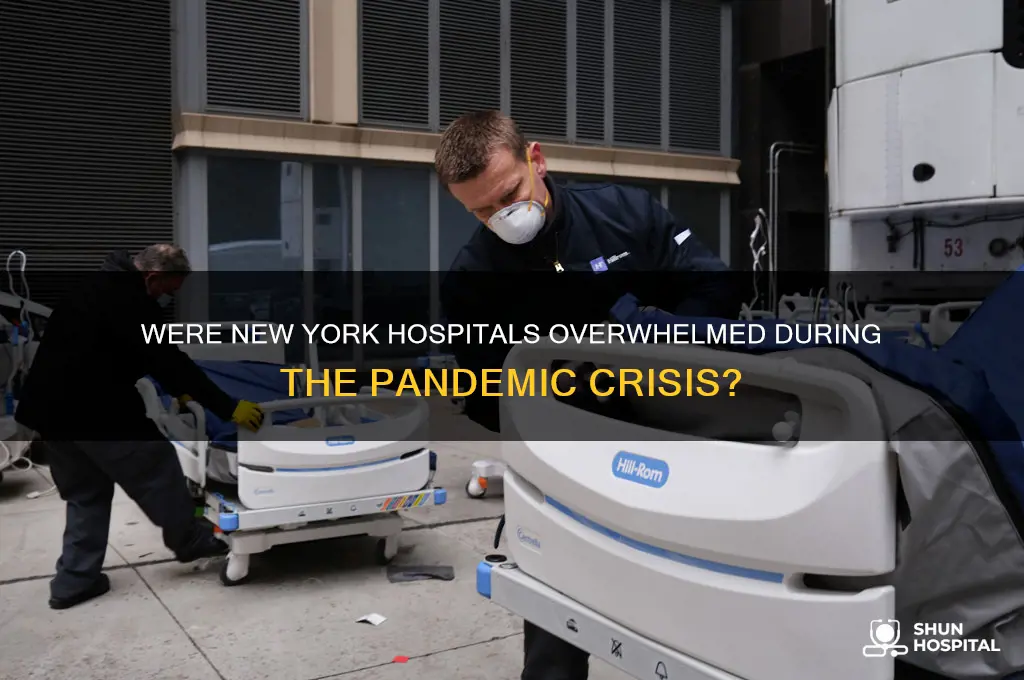
Supply Chain Challenges
During the peak of the COVID-19 pandemic, New York hospitals faced unprecedented demand for critical supplies, from personal protective equipment (PPE) to ventilators. The supply chain, already strained by global disruptions, became a bottleneck that exacerbated the crisis. For instance, N95 masks, essential for healthcare worker safety, were in such short supply that hospitals resorted to reusing them beyond their intended single-use lifespan. This scarcity wasn’t just a local issue; it was a global scramble, with countries outbidding each other for limited resources. The result? Hospitals in New York, the epicenter of the U.S. outbreak, were forced to ration supplies, putting both patients and staff at risk.
One of the most glaring supply chain challenges was the over-reliance on single-source suppliers, particularly those based overseas. China, a major manufacturer of medical supplies, saw its production halt due to lockdowns, creating a ripple effect worldwide. New York hospitals, which had stocked up on supplies just-in-time rather than just-in-case, were caught off guard. For example, the production of ventilators, critical for COVID-19 patients in respiratory distress, was delayed due to shortages of components like sensors and microchips. This highlighted the fragility of a system where 80% of active pharmaceutical ingredients used in U.S. medications are sourced from abroad. Diversifying supply chains and building domestic manufacturing capacity became urgent priorities, but these solutions require time and investment—luxuries the pandemic didn’t afford.
Another critical issue was the lack of real-time visibility into supply chain operations. Hospitals struggled to track orders, predict delivery times, or anticipate shortages. This opacity was compounded by hoarding and price gouging, as desperate facilities competed for the same limited resources. For instance, a box of surgical masks that typically cost $50 pre-pandemic surged to $700 or more. To mitigate this, some hospitals turned to unconventional sources, like construction companies for N95 masks or distilleries for hand sanitizer. While creative, these stopgap measures underscored the need for a more resilient, transparent supply chain system. Implementing technologies like blockchain or AI-driven inventory management could provide the visibility needed to prevent future shortages.
The pandemic also exposed the fragility of logistics networks, particularly in the "last mile" of delivery. With commercial flights grounded, the usual channels for transporting medical supplies were severely limited. Hospitals in New York had to rely on alternative methods, such as charter flights or ground transportation, which were slower and more expensive. For example, a shipment of ventilators from the federal stockpile took days longer than expected to reach New York City, delaying their deployment to patients in critical condition. Strengthening logistics infrastructure, including investing in dedicated medical supply transport networks, could ensure faster, more reliable delivery during crises.
Finally, the human factor cannot be overlooked. Supply chain disruptions weren’t just about physical goods—they were about the people managing them. Procurement officers, logistics coordinators, and warehouse workers faced immense pressure, often working overtime in high-stress environments. Burnout and staff shortages further strained the system, leading to errors and inefficiencies. Training and supporting these essential workers, while integrating automation where possible, could alleviate some of this burden. After all, a supply chain is only as strong as the people who manage it.
In addressing these supply chain challenges, New York hospitals—and healthcare systems globally—must adopt a multi-faceted approach. Diversifying suppliers, investing in technology, strengthening logistics, and supporting the workforce are not just reactive measures but proactive steps toward building resilience. The pandemic served as a stark reminder that preparedness isn’t a luxury; it’s a necessity. By learning from these lessons, we can ensure that hospitals are better equipped to face the next crisis, whatever it may be.
Creative Display Cabinet Ideas for Hospitals
You may want to see also
Explore related products






![]()
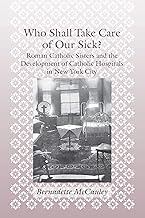
Triage and Care Prioritization
During the peak of the COVID-19 pandemic, New York City hospitals faced unprecedented surges in patient volume, forcing them to implement strict triage and care prioritization protocols. Triage, traditionally a battlefield concept, became a daily reality in emergency departments and ICUs. Nurses and physicians had to make split-second decisions about who would receive ventilators, ICU beds, or even basic monitoring, often based on age, comorbidities, and likelihood of survival. For instance, patients with severe respiratory distress but no significant underlying conditions were prioritized over those with advanced age and multiple chronic illnesses, a practice that sparked ethical debates but was deemed necessary to maximize survival rates.
One critical tool in this process was the use of scoring systems like the Sequential Organ Failure Assessment (SOFA) or the Clinical Frailty Scale (CFS). These standardized assessments helped clinicians objectively evaluate patients’ conditions and prognoses, reducing bias in decision-making. For example, a 45-year-old with a SOFA score of 5 (indicating moderate organ dysfunction) would likely be prioritized over a 75-year-old with a SOFA score of 8 and a CFS score of 7 (indicating severe frailty). While these tools provided structure, they also highlighted the harsh realities of resource allocation during a crisis.
Practical tips for healthcare providers in such scenarios include clear communication with patients and families about the rationale behind prioritization decisions. Transparency can mitigate mistrust, even in the face of difficult outcomes. Additionally, hospitals should establish multidisciplinary ethics committees to review and guide triage protocols, ensuring they align with both medical necessity and moral principles. For instance, some institutions adopted a "first-come, first-served" approach for patients with equal prognoses, while others prioritized healthcare workers or those with caregiving responsibilities, reflecting broader societal values.
Comparatively, New York’s experience contrasts with regions that avoided such extreme measures due to earlier lockdowns or lower infection rates. In Italy, for example, age-based triage was openly discussed but less systematically implemented, leading to higher mortality among older patients. New York’s approach, while more structured, still faced criticism for potentially exacerbating health disparities, as marginalized communities were disproportionately affected by COVID-19. This underscores the need for equitable triage protocols that consider social determinants of health, not just clinical factors.
In conclusion, triage and care prioritization during New York’s hospital overload were not just clinical decisions but moral and logistical challenges. By leveraging standardized tools, fostering transparency, and addressing ethical concerns, healthcare systems can better prepare for future crises. The lessons from New York serve as a stark reminder that effective triage is not just about saving lives but also about preserving trust and equity in the face of overwhelming demand.
Chief Nursing Officers: Essential for Critical Access Hospital Success?
You may want to see also
Explore related products




![Pandemic [DVD]](https://m.media-amazon.com/images/I/91ynbSGeZVS._AC_UL320_.jpg)

![]()
Government and Policy Responses
During the peak of the COVID-19 pandemic, New York City’s hospitals faced unprecedented strain, with patient surges threatening to overwhelm capacity. In response, the government and policymakers implemented a series of measures to mitigate the crisis. One of the most immediate actions was the issuance of an executive order to increase hospital capacity by 50%, achieved through the conversion of non-medical spaces into temporary care facilities and the construction of emergency field hospitals, such as the Javits Center and the USS Comfort. These steps were critical in preventing a complete collapse of the healthcare system.
Another key policy response was the invocation of the Defense Production Act to accelerate the production and distribution of personal protective equipment (PPE) and ventilators. This federal intervention ensured that New York hospitals received essential supplies at a time when global shortages were rampant. Additionally, the government mandated a statewide pause, closing non-essential businesses and issuing stay-at-home orders to flatten the curve. While these measures were economically painful, they significantly reduced the rate of infection, giving hospitals breathing room to manage patient loads.
Workforce shortages emerged as a critical challenge, prompting the government to waive licensing requirements for out-of-state healthcare professionals and retired medical personnel to join the frontlines. This policy not only bolstered staffing numbers but also ensured that experienced hands were available to handle the influx of patients. Simultaneously, the state launched a public campaign to recruit volunteers, resulting in thousands of additional workers, including medical students and professionals from other fields, stepping up to assist.
A comparative analysis of these responses reveals both strengths and limitations. While the rapid expansion of hospital capacity and the mobilization of resources were effective in the short term, the lack of a coordinated national strategy left states like New York scrambling for supplies and competing against each other. This highlighted the need for a more unified federal approach in future crises. Moreover, the economic and social costs of lockdowns underscored the importance of balancing public health measures with sustainable long-term strategies.
In conclusion, the government and policy responses to the strain on New York hospitals during the pandemic were multifaceted and adaptive. From increasing capacity and securing supplies to addressing workforce shortages, these measures played a pivotal role in averting a complete healthcare collapse. However, the experience also exposed vulnerabilities in the system, offering valuable lessons for improving preparedness and coordination in future emergencies. Practical takeaways include the importance of maintaining strategic stockpiles of medical supplies, fostering interstate collaboration, and investing in flexible healthcare infrastructure to withstand sudden surges in demand.
Exploring Beijing's Healthcare: Hospitals in the Capital
You may want to see also
Frequently asked questions
Yes, during the spring of 2020, New York City hospitals were severely overwhelmed by the influx of COVID-19 patients, leading to shortages of beds, ventilators, and medical staff.
Hospitals responded by setting up temporary facilities, converting non-ICU spaces into critical care units, and receiving assistance from out-of-state medical teams and the federal government to manage the surge.
No, after the initial wave, hospitals were able to stabilize as infection rates decreased, resources were replenished, and vaccination efforts began, though they faced challenges during subsequent waves.


![Pandemic [DVD]](https://m.media-amazon.com/images/I/51vChb09XaL._AC_UL320_.jpg)


![Pandemic [DVD]](https://m.media-amazon.com/images/I/81G1z+AOoNL._AC_UL320_.jpg)
![PANDEMIC [Blu-ray]](https://m.media-amazon.com/images/I/71xlZkgPU4L._AC_UL320_.jpg)



![Pandemic Pandemic [DVD]](https://m.media-amazon.com/images/I/81dZDU9gUpL._AC_UL320_.jpg)

![Pandemic [Blu-ray]](https://m.media-amazon.com/images/I/61EbhmkB1tS._AC_UL320_.jpg)