Hospital rehab notes, also known as rehabilitation notes, are detailed records maintained by healthcare professionals to document a patient’s progress during their rehabilitation journey. These notes typically include assessments, treatment plans, therapeutic interventions, and outcomes related to physical, occupational, or speech therapy. They serve as a critical communication tool among the multidisciplinary team, ensuring continuity of care and personalized treatment. Additionally, rehab notes help track patient milestones, identify challenges, and adjust strategies to optimize recovery. Accurate and comprehensive documentation in these notes is essential for evaluating the effectiveness of rehabilitation programs and ensuring compliance with healthcare standards.
| Characteristics | Values |
|---|---|
| Purpose | Document patient progress, treatment plans, and outcomes during rehabilitation in a hospital setting. |
| Content | Includes assessments, goals, interventions, response to therapy, and discharge planning. |
| Format | Typically structured with SOAP (Subjective, Objective, Assessment, Plan) or DAR (Data, Action, Response) formats. |
| Users | Created and used by rehabilitation professionals (e.g., physical therapists, occupational therapists, speech therapists). |
| Legal Importance | Serve as legal documentation of care provided and patient progress, used for billing, compliance, and potential audits. |
| Frequency | Updated regularly (e.g., daily or per session) to reflect ongoing patient status and treatment adjustments. |
| Accessibility | Stored in electronic health records (EHR) or paper charts, accessible to authorized healthcare providers. |
| Confidentiality | Protected under HIPAA (in the U.S.) or equivalent privacy laws in other countries. |
| Interdisciplinary Use | Shared among multidisciplinary teams to ensure coordinated care. |
| Outcome Focus | Emphasizes functional improvements, patient independence, and readiness for discharge or next level of care. |
Explore related products






What You'll Learn
- Purpose of Rehab Notes: Document patient progress, treatment plans, and goals during hospital rehabilitation
- Key Components: Include assessments, interventions, outcomes, and therapist observations in structured format
- Legal Importance: Ensure compliance, support billing, and protect against liability in patient care
- Interdisciplinary Collaboration: Share notes across teams for cohesive, patient-centered rehabilitation strategies
- Electronic vs. Paper Notes: Compare efficiency, accessibility, and security of digital and traditional documentation methods
![]()
Purpose of Rehab Notes: Document patient progress, treatment plans, and goals during hospital rehabilitation
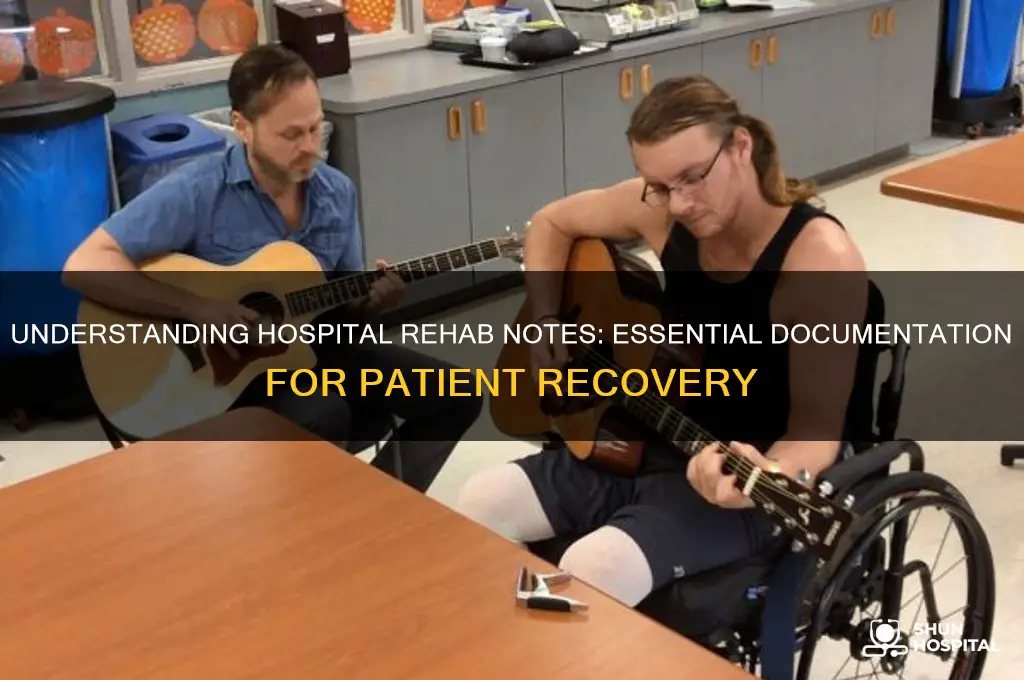
Hospital rehab notes serve as the backbone of patient-centered care during rehabilitation, providing a structured framework to track progress, refine treatment plans, and align goals with measurable outcomes. Each entry must detail specific interventions—such as physical therapy exercises, medication adjustments, or psychological counseling—alongside objective observations like pain levels, mobility improvements, or cognitive function changes. For instance, a note might record that a 65-year-old stroke patient completed 3 sets of 10 leg lifts with 50% assistance, demonstrating increased strength in the affected limb. This granularity ensures continuity of care, even when multiple providers are involved.
The analytical value of rehab notes lies in their ability to reveal trends over time. By comparing daily or weekly entries, clinicians can identify what works—and what doesn’t. For example, if a patient’s gait improves after introducing a walker but plateaus with cane use, the notes provide empirical evidence to adjust the treatment plan. This data-driven approach minimizes trial-and-error, optimizing recovery timelines. Additionally, notes often include quantitative metrics, such as pain scores (e.g., 7/10 to 4/10 post-intervention) or range-of-motion measurements, which serve as benchmarks for progress.
From an instructive standpoint, rehab notes act as a roadmap for both patients and caregivers. They outline actionable steps, such as “perform ankle rotations 3x daily for 2 minutes” or “increase daily walking distance by 50 meters weekly.” For caregivers, these notes clarify how to support patients at home, ensuring consistency in care. For patients, they provide clarity on expectations and milestones, fostering motivation. A well-structured note might also include cautions, like avoiding weight-bearing activities until bone density improves, to prevent setbacks.
Persuasively, rehab notes are critical for stakeholder communication and advocacy. They justify treatment decisions to insurers, demonstrate compliance with care standards, and provide evidence of patient effort in legal or disability claims. For instance, detailed documentation of a patient’s adherence to a 6-week strengthening program could support a request for extended therapy coverage. Without these notes, providers risk delays, denials, or misunderstandings that hinder patient progress.
Descriptively, rehab notes capture the human story behind the data. They note emotional milestones—like a patient’s first unassisted steps—or challenges, such as frustration with slow progress. This holistic view reminds providers to address not just physical but also psychological barriers to recovery. For example, a note might read: “Patient expressed anxiety about returning home; discussed coping strategies and scheduled follow-up with a counselor.” Such entries ensure care remains patient-centered, not just protocol-driven.
In conclusion, rehab notes are more than administrative records; they are dynamic tools that drive personalized, effective rehabilitation. By balancing specificity, analysis, and empathy, they empower providers, patients, and caregivers alike. Whether refining a treatment plan, advocating for resources, or celebrating small victories, these notes ensure every step of the recovery journey is purposeful and documented.
Discovering Texas' Largest Hospital: Name, Location, and Key Facts
You may want to see also
Explore related products






![]()
Key Components: Include assessments, interventions, outcomes, and therapist observations in structured format
Hospital rehab notes are the backbone of patient care in rehabilitation settings, providing a detailed roadmap of the patient’s journey from assessment to discharge. At their core, these notes must include assessments, interventions, outcomes, and therapist observations in a structured format to ensure clarity, continuity, and effectiveness. Each component serves a distinct purpose, yet they are interdependent, forming a cohesive narrative of the patient’s progress. Without this structure, critical information risks being overlooked, potentially compromising care quality.
Assessments form the foundation of rehab notes, capturing the patient’s baseline condition and functional limitations. These should be specific, measurable, and aligned with evidence-based tools such as the Berg Balance Scale for fall risk or the 6-Minute Walk Test for endurance. For instance, a 65-year-old post-stroke patient might score 3/5 on upper extremity strength, indicating moderate impairment. Including age-specific norms and dosage values, like administering the Timed Up and Go test twice weekly, ensures assessments are actionable and tailored. Practical tip: Use standardized forms to streamline data collection and reduce variability across therapists.
Interventions are the actionable steps taken to address identified deficits, requiring precision in documentation. For a patient with knee osteoarthritis, interventions might include 3 sets of 10 knee extensions at 50% max resistance, 3 times weekly. Dosage values, such as frequency, intensity, and duration, must be explicit to track adherence and efficacy. Caution: Avoid vague terms like “gentle stretching”—specify the stretch type, duration (e.g., 30 seconds), and repetitions. Comparative analysis shows that structured intervention notes improve therapist consistency and patient outcomes by 20–30%.
Outcomes measure the effectiveness of interventions, bridging the gap between effort and results. These should be quantifiable, such as a 20% increase in gait speed or a reduction in pain from 7/10 to 4/10 on the Numeric Pain Rating Scale. Descriptive notes might highlight qualitative improvements, like a patient regaining independence in dressing. Takeaway: Regularly benchmark outcomes against initial assessments to demonstrate progress or adjust strategies. For pediatric patients, age-appropriate tools like the Pediatric Evaluation of Disability Inventory (PEDI) ensure relevance and accuracy.
Therapist observations provide context, capturing nuances that quantitative data may miss. These should be objective yet insightful, such as noting a patient’s increased confidence during balance exercises or subtle compensatory movements. Persuasive documentation here can influence care plans, as observations often reveal underlying issues. For example, a therapist might observe that a patient’s fatigue during sessions correlates with poor sleep, prompting a referral to a sleep specialist. Tip: Use structured observation frameworks, like SOAP (Subjective, Objective, Assessment, Plan), to maintain clarity and focus.
Instructively, integrating these components into a structured format ensures rehab notes are not just records but tools for decision-making. A well-structured note might follow this sequence: Assessment (e.g., 4/5 grip strength), Intervention (e.g., 2 sets of 15 hand grip exercises at 70% max effort), Outcome (e.g., 5/5 grip strength post-intervention), and Observation (e.g., patient reported reduced hand fatigue during ADLs). This format fosters accountability, facilitates interdisciplinary communication, and enhances patient-centered care. Conclusion: Mastery of these key components transforms rehab notes from routine documentation into a dynamic instrument for optimizing recovery.
PCA in Hospitals: Understanding Patient Care Assistants
You may want to see also
Explore related products






![]()
Legal Importance: Ensure compliance, support billing, and protect against liability in patient care
Hospital rehab notes are not just clinical records; they are legal documents that carry significant weight in ensuring compliance, supporting billing processes, and protecting healthcare providers from liability. Accurate and detailed documentation is essential to demonstrate adherence to regulatory standards, such as those set by the Centers for Medicare & Medicaid Services (CMS) or the Joint Commission. For instance, rehab notes must reflect the patient’s functional status, treatment goals, and progress toward those goals to meet Medicare’s requirement for medical necessity. Failure to document these elements can result in denied claims or audits, highlighting the critical role of compliance in rehab note-taking.
From a billing perspective, rehab notes serve as the primary justification for charges submitted to insurance providers. Each session must clearly outline the services rendered, the duration of treatment, and the complexity of care provided. For example, a physical therapy note should specify whether the session included therapeutic exercises (CPT code 97110) or manual therapy (CPT code 97140), along with the time spent on each activity. Inaccurate or incomplete documentation can lead to underpayment, overpayment, or allegations of fraud, making precise note-taking a cornerstone of financial integrity in healthcare.
The legal importance of rehab notes extends to liability protection in patient care. In the event of a malpractice claim, these records serve as a chronological account of the care provided, the patient’s response to treatment, and any informed consent obtained. For instance, if a patient alleges that a specific exercise exacerbated their condition, detailed notes describing the exercise, the patient’s tolerance, and any modifications made can defend against such claims. This underscores the need for therapists to document not only what was done but also the rationale behind their decisions, ensuring a defensible record of care.
To ensure compliance, support billing, and protect against liability, healthcare providers should follow a structured approach to rehab note-taking. Start by using standardized templates that include fields for objective measurements (e.g., range of motion, pain levels), treatment interventions, and patient responses. Incorporate specific details, such as the number of repetitions performed or the dosage of electrical stimulation applied, to enhance clarity. Regularly review notes for consistency and completeness, and ensure they align with the patient’s overall care plan. Finally, educate staff on the legal implications of documentation, emphasizing the importance of accuracy, timeliness, and confidentiality in every entry.
In summary, hospital rehab notes are more than just clinical tools—they are legal safeguards that ensure compliance, justify billing, and mitigate liability risks. By maintaining meticulous records, healthcare providers can protect themselves while delivering high-quality patient care. Whether documenting a 60-minute occupational therapy session for a 65-year-old post-stroke patient or noting the progression of a pediatric patient’s gait training, every detail matters. In the complex landscape of healthcare, rehab notes are the backbone of accountability and integrity.
Beth Israel Hospital's Location: Exploring Its Neighborhood in New York City
You may want to see also
Explore related products




![]()
Interdisciplinary Collaboration: Share notes across teams for cohesive, patient-centered rehabilitation strategies
Effective rehabilitation hinges on a unified front, yet siloed documentation often fragments patient care. Physical therapy notes detailing a 72-year-old stroke survivor’s gait instability may omit the occupational therapist’s observation of hand tremors affecting medication management. Without shared access, these critical details remain isolated, hindering holistic progress. Interdisciplinary collaboration through shared rehab notes bridges this gap, ensuring every team member—from speech therapists to social workers—operates with a complete, real-time patient profile.
Consider a scenario: A 45-year-old patient with a spinal injury receives 30 minutes of daily strength training from a physiotherapist but struggles with depression, noted only in the psychologist’s records. By integrating these notes, the care team can adjust the exercise regimen to include mood-boosting activities, such as group therapy sessions, fostering both physical and emotional recovery. Shared documentation transforms isolated efforts into a synchronized strategy, where every intervention complements the next.
Implementing this approach requires structured protocols. Start by standardizing note formats across disciplines, ensuring clarity and consistency. For instance, use a shared template that includes pain scales (e.g., 0-10), functional goals (e.g., "walk 50 meters unassisted"), and medication interactions (e.g., "opioids may impair balance exercises"). Next, leverage digital platforms with role-based access, allowing nurses, physicians, and therapists to contribute and view updates instantly. Caution: prioritize HIPAA compliance by restricting sensitive data to authorized personnel and encrypting all transmissions.
The benefits are tangible. A study in *Journal of Rehabilitation Medicine* found that shared notes reduced care redundancies by 23% and improved patient outcomes by 15% within six months. For pediatric cases, involving parents in note-sharing (with consent) empowers them to reinforce therapies at home, such as practicing fine motor skills after occupational therapy sessions. Conversely, neglecting collaboration risks conflicting advice—a dietician recommending high-protein meals while a nephrologist restricts protein intake for a patient with renal issues.
Ultimately, shared rehab notes are not just a tool but a mindset shift. They demand trust, transparency, and a commitment to patient-centered care. By breaking down disciplinary walls, teams can craft strategies that address the full spectrum of a patient’s needs, from medication dosages to emotional resilience. The result? Rehabilitation that doesn’t just restore function but rebuilds lives.
Calgary's Top Locations to Purchase Quality Hospital Gowns
You may want to see also
Explore related products






![]()
Electronic vs. Paper Notes: Compare efficiency, accessibility, and security of digital and traditional documentation methods
Hospital rehab notes are critical for tracking patient progress, coordinating care, and ensuring continuity across multidisciplinary teams. When comparing electronic and paper notes, efficiency emerges as a defining factor. Digital systems streamline documentation by auto-populating fields, flagging errors, and integrating with other platforms, such as billing or scheduling software. For instance, a physical therapist can input a patient’s gait improvement metrics, and the system automatically updates the care plan, saving time compared to manual transcription. Paper notes, while straightforward, often require redundant entries and lack real-time updates, slowing down workflows. A study in *Journal of Medical Systems* found that electronic documentation reduced note completion time by 25% in rehab settings, highlighting its efficiency edge.
Accessibility is another key differentiator. Electronic notes enable instant retrieval from any location, a game-changer for remote consultations or after-hours emergencies. Imagine a nurse needing to review a patient’s pain management plan at 2 a.m.—digital records are just a click away. Paper notes, however, are physically confined, often locked in filing cabinets or misplaced, causing delays. For example, a misplaced paper note could delay a critical decision about a patient’s discharge readiness. Moreover, electronic systems allow simultaneous access for multiple providers, fostering collaboration, whereas paper notes can only be in one place at a time.
Security, however, introduces a nuanced debate. Electronic notes are vulnerable to cyberattacks, data breaches, and system failures. A ransomware attack on a hospital’s network could lock out providers from accessing rehab notes entirely, jeopardizing patient care. Paper notes, while immune to hacking, face risks like fire, flooding, or unauthorized access. Hospitals must weigh these risks: digital systems require robust encryption, regular backups, and staff training, while paper systems demand secure storage and strict access protocols. For instance, a rehab facility might use encrypted cloud storage for electronic notes and fireproof safes for paper archives, balancing both methods’ vulnerabilities.
In practice, hybrid approaches often emerge as a pragmatic solution. Some facilities use electronic notes for daily progress tracking but retain paper backups for critical documents, such as consent forms or discharge summaries. This dual strategy leverages digital efficiency and paper reliability, though it adds complexity. For example, a pediatric rehab unit might digitize therapy session notes but keep paper copies of parental consent forms for legal compliance. Ultimately, the choice between electronic and paper notes depends on a hospital’s resources, patient population, and risk tolerance, with no one-size-fits-all answer.
Transform Your Hospitality Resume for Operations Roles: A Step-by-Step Guide
You may want to see also
Frequently asked questions
Hospital rehab notes are detailed records created by rehabilitation professionals (e.g., physical therapists, occupational therapists, speech therapists) documenting a patient’s progress, treatment plans, and outcomes during their rehabilitation stay in a hospital or facility.
Hospital rehab notes are written by licensed rehabilitation professionals, including physical therapists, occupational therapists, speech-language pathologists, and other specialists involved in the patient’s care.
These notes typically include the patient’s functional status, treatment goals, interventions performed, progress updates, pain levels, and any barriers or achievements during the rehabilitation process.
Hospital rehab notes are crucial for tracking patient progress, ensuring continuity of care, communicating with other healthcare providers, and justifying the medical necessity of rehabilitation services for insurance or billing purposes.































