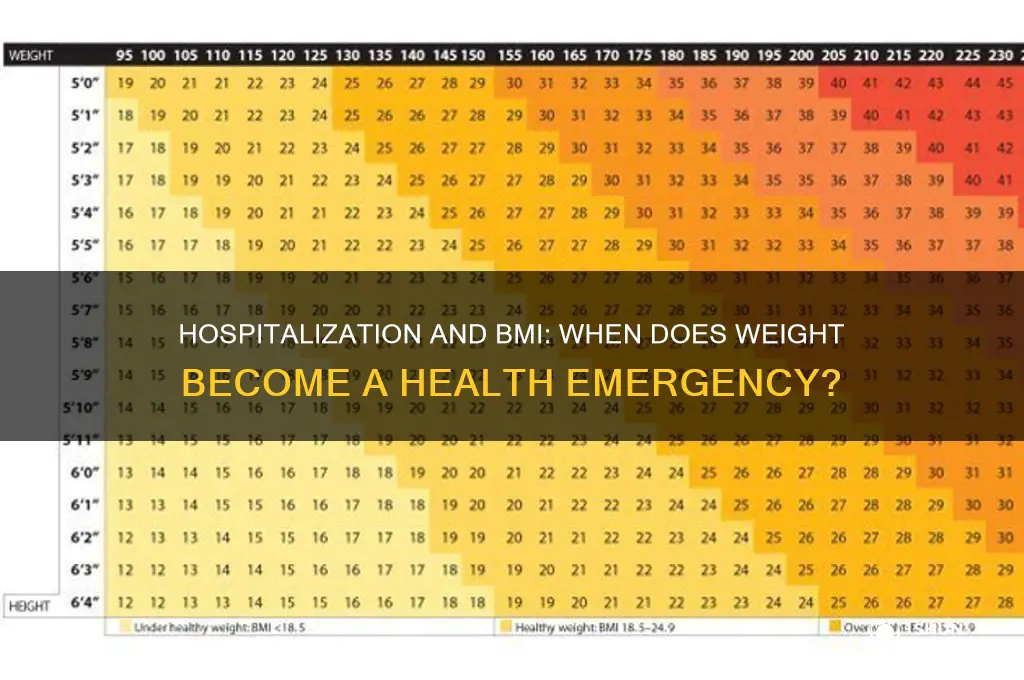
The Body Mass Index (BMI) is a widely used metric to assess whether an individual’s weight falls within a healthy range relative to their height. While BMI is not a perfect indicator of overall health, it can serve as a screening tool for potential weight-related issues. In some cases, individuals may be hospitalized due to complications arising from extreme BMI values, whether from severe obesity or underweight conditions. Understanding the BMI at which hospitalization becomes necessary can shed light on the critical health risks associated with significant deviations from a healthy weight range, emphasizing the importance of early intervention and preventive care.
| Characteristics | Values |
|---|---|
| Typical BMI Threshold for Hospitalization (Anorexia Nervosa) | 15-16 or below |
| Reason for Hospitalization at This BMI | Severe malnutrition, organ failure risk, electrolyte imbalances, bradycardia (slow heart rate), hypothermia |
| Other Factors Influencing Hospitalization | Rapid weight loss, medical complications, psychiatric instability, inability to maintain weight outpatient |
| BMI Alone is Not the Sole Criterion | Overall health, lab results, psychological state, and treatment response are also considered |
| Higher BMI Hospitalizations | Possible for individuals with severe medical complications or comorbidities, even at higher BMIs |
Explore related products






What You'll Learn
- BMI Thresholds for Hospitalization: Critical BMI levels requiring medical intervention and hospitalization
- Health Risks at Extreme BMIs: Severe complications linked to very high or low BMIs
- Hospitalization Criteria by BMI: Medical guidelines for admitting patients based on BMI
- BMI-Related Emergency Cases: Urgent health issues necessitating hospitalization due to BMI extremes
- Recovery Post-Hospitalization: Managing BMI after hospitalization to prevent re-admission
![]()
BMI Thresholds for Hospitalization: Critical BMI levels requiring medical intervention and hospitalization
Hospitalization due to extreme BMI levels is a critical intervention reserved for life-threatening conditions. For individuals with anorexia nervosa, medical professionals often consider hospitalization when BMI drops below 16, as this level is associated with severe malnutrition, organ failure, and heightened mortality risk. At this threshold, the body lacks sufficient fat and muscle mass to sustain vital functions, necessitating immediate nutritional rehabilitation and psychiatric support.
In contrast, morbid obesity (BMI ≥40) or class III obesity (BMI ≥50) may prompt hospitalization when complications arise, such as severe sleep apnea, uncontrolled diabetes, or cardiovascular instability. For example, a BMI of 60 or higher often correlates with mobility issues, chronic pain, and respiratory distress, requiring intensive medical management. Hospitalization in these cases focuses on stabilizing acute conditions before addressing long-term weight management strategies.
Pediatric cases present unique thresholds, as BMI-for-age percentile is used instead of absolute BMI. Hospitalization is typically considered when a child’s BMI falls below the 1st percentile or exceeds the 99th percentile, coupled with comorbidities like growth stunting or hypertension. Early intervention is crucial in children to prevent irreversible developmental damage or lifelong health complications.
Practical tips for caregivers and individuals include monitoring weight trends, not just absolute BMI, and recognizing red flags such as rapid weight loss, fainting, or persistent fatigue. For those at risk, regular consultations with dietitians, endocrinologists, and mental health professionals can preempt the need for hospitalization. Ultimately, BMI thresholds are not rigid rules but critical markers that signal the urgency for medical intervention to prevent irreversible harm.
Ketamine in Hospitals: When and Why is it Administered?
You may want to see also
Explore related products






![]()
Health Risks at Extreme BMIs: Severe complications linked to very high or low BMIs
Extreme Body Mass Index (BMI) values, whether very high or very low, signal critical health risks that often lead to hospitalization. A BMI below 15 or above 40 typically indicates severe malnutrition or obesity, respectively, both of which can trigger life-threatening complications. For instance, individuals with a BMI under 15 often face organ failure, hypothermia, and weakened immunity, while those with a BMI over 40 may experience respiratory distress, cardiovascular collapse, or diabetic ketoacidosis. These conditions frequently require immediate medical intervention, making hospitalization inevitable.
Consider the case of severe anorexia nervosa, where a BMI below 13 is common. At this level, the body begins to shut down non-essential functions to conserve energy, leading to bradycardia (slow heart rate), hypotension (low blood pressure), and electrolyte imbalances. Hospitalization often becomes necessary to stabilize vital signs, administer intravenous nutrition, and prevent irreversible damage to the heart, kidneys, or liver. Conversely, a BMI exceeding 50 in morbid obesity can cause severe sleep apnea, pulmonary hypertension, and joint degeneration, all of which may necessitate urgent care to prevent respiratory failure or mobility loss.
The risks aren’t just physical; extreme BMIs also exacerbate mental health issues. Severe malnutrition can lead to depression, anxiety, and cognitive impairment, while morbid obesity often correlates with severe depression, body dysmorphia, and social isolation. These psychological complications frequently require dual treatment—both medical stabilization and psychiatric intervention—during hospitalization. For example, a patient with a BMI of 12 might need antidepressants alongside refeeding protocols, while someone with a BMI of 60 could benefit from counseling alongside bariatric surgery preparation.
Practical steps to mitigate these risks include early intervention and monitoring. For individuals with a BMI below 16 or above 45, regular check-ups with a multidisciplinary team—including dietitians, endocrinologists, and mental health professionals—are essential. Gradual, supervised weight restoration or reduction is safer than abrupt changes, as rapid shifts can trigger refeeding syndrome or metabolic crises. For instance, increasing caloric intake by 500–1000 kcal/day under medical supervision can prevent complications in underweight individuals, while a 5–10% weight loss goal over 6 months is recommended for those with extreme obesity.
In conclusion, hospitalization at extreme BMIs is often a last resort to address severe, systemic complications. Recognizing the signs early—such as rapid weight changes, syncope, or persistent infections—can prevent the need for emergency care. Whether through nutritional rehabilitation, surgical intervention, or psychological support, timely and tailored treatment is key to reducing the risks associated with very high or low BMIs.
Mercy Hospitals Across the Nation: Beyond Springfield, MO
You may want to see also
Explore related products






![]()
Hospitalization Criteria by BMI: Medical guidelines for admitting patients based on BMI
BMI thresholds for hospitalization vary widely depending on the medical condition, age, and individual health factors. For instance, patients with anorexia nervosa are often hospitalized when their BMI drops below 15, as this level poses severe risks of organ failure and cardiac complications. In contrast, individuals with obesity-related complications like severe sleep apnea or type 2 diabetes may be admitted for intensive management when their BMI exceeds 40, particularly if conservative treatments have failed. These thresholds are not arbitrary but are grounded in evidence-based guidelines designed to prevent life-threatening complications.
Pediatric hospitalization criteria differ significantly from adult standards. Children and adolescents with a BMI below the 5th percentile for their age group may require hospitalization for malnutrition or failure to thrive, especially if accompanied by developmental delays or severe dehydration. On the other end, adolescents with obesity (BMI above the 95th percentile) may be admitted for bariatric evaluation or management of comorbidities like hypertension or fatty liver disease. Age-specific growth charts, rather than absolute BMI values, guide these decisions to account for developmental variability.
Hospitalization for BMI-related conditions often involves multidisciplinary care. For example, a patient admitted with a BMI of 12 due to an eating disorder will typically receive nutritional rehabilitation, psychiatric support, and medical monitoring for electrolyte imbalances. Conversely, a patient with a BMI of 50 admitted for obesity-related complications may undergo a combination of dietary counseling, physical therapy, and surgical evaluation. The goal is not just to address the BMI but to stabilize the patient and prevent long-term health deterioration.
Critics argue that BMI alone is an insufficient criterion for hospitalization, as it does not account for body composition, muscle mass, or overall health status. For instance, a highly muscular athlete may have a BMI in the "obese" range without associated health risks, while an elderly individual with significant muscle loss may appear within a "normal" BMI range but suffer from malnutrition. Clinicians must therefore supplement BMI with additional assessments, such as waist circumference, lab results, and clinical history, to make informed decisions.
Practical tips for patients and caregivers include monitoring weight trends rather than fixating on single BMI measurements, especially in chronic conditions. For those at risk of hospitalization, maintaining open communication with healthcare providers and adhering to prescribed interventions can delay or prevent the need for admission. Ultimately, BMI-based hospitalization criteria serve as a starting point, but individualized care remains the cornerstone of effective treatment.
Krayzie Bone's Health: Discharged from Hospital?
You may want to see also
Explore related products






![]()
BMI-Related Emergency Cases: Urgent health issues necessitating hospitalization due to BMI extremes
Extreme BMI values, whether excessively high or low, can precipitate medical crises demanding immediate hospitalization. For instance, individuals with a BMI below 15 often face severe malnutrition, leading to organ failure, hypothermia, or cardiac arrhythmias. Conversely, a BMI exceeding 50 can trigger life-threatening conditions like respiratory distress, uncontrolled diabetes, or heart failure. These extremes disrupt the body’s homeostasis, necessitating urgent intervention to stabilize vital functions and prevent irreversible damage.
Consider the case of a 28-year-old with a BMI of 13.5, hospitalized after collapsing due to hypoglycemia and bradycardia. Their lab results showed critically low potassium (2.8 mmol/L) and albumin (2.1 g/dL), indicative of severe starvation. Treatment involved gradual refeeding under ICU monitoring, starting with 10–15 kcal/kg/day to avoid refeeding syndrome, a potentially fatal complication. This example underscores the fragility of the human body when pushed to such limits and the precision required in emergency care.
On the opposite end, a 45-year-old with a BMI of 55 was admitted with acute respiratory failure and lymphedema. Their oxygen saturation dropped to 82% at rest, exacerbated by obstructive sleep apnea and morbid obesity. Emergency management included CPAP therapy, diuretics to reduce fluid overload, and a multidisciplinary approach involving bariatric surgery consultation. Such cases highlight the compounding risks of extreme obesity, where multiple systems fail simultaneously, requiring coordinated, rapid response.
Hospitalization thresholds often correlate with BMI-induced complications rather than BMI alone. For example, a BMI of 16 might warrant admission if accompanied by syncope, amenorrhea, or electrolyte imbalances, while a BMI of 45 could necessitate intervention if paired with hypertension, orthopnea, or venous stasis ulcers. Clinicians must assess not just the number but the clinical context, tailoring interventions to address the root cause—whether malnutrition, metabolic dysfunction, or mechanical stress on organs.
Prevention remains paramount. For those at risk, early intervention—such as nutritional counseling for underweight individuals or lifestyle modifications for the obese—can avert emergencies. Monitoring tools like regular BMI screenings, especially in high-risk groups (adolescents, elderly, post-bariatric patients), provide opportunities for timely intervention. Ultimately, recognizing the red flags of BMI extremes—fatigue, edema, unexplained weight changes—can save lives by prompting swift medical attention before crises escalate.
Mask Policies in Hospitals: What You Need to Know
You may want to see also
Explore related products






![]()
Recovery Post-Hospitalization: Managing BMI after hospitalization to prevent re-admission
Hospitalization often serves as a critical wake-up call for individuals whose BMI has reached levels posing severe health risks. Whether due to obesity-related complications like diabetes, heart disease, or respiratory issues, or malnutrition leading to weakened immunity and organ failure, the BMI threshold for hospitalization varies. However, research suggests that BMIs above 40 or below 16 often correlate with acute medical interventions. Post-hospitalization, managing BMI becomes paramount to prevent re-admission, as the body’s recovery hinges on restoring metabolic balance and addressing underlying health issues.
Step 1: Establish a Structured Nutrition Plan
Upon discharge, consult a registered dietitian to create a personalized meal plan tailored to your BMI and health condition. For those recovering from obesity, aim for a calorie deficit of 500–750 kcal/day to promote gradual weight loss (0.5–1 kg/week). Incorporate lean proteins, whole grains, and fiber-rich vegetables while limiting processed foods and sugars. Conversely, if hospitalization was due to underweight BMI, focus on calorie-dense, nutrient-rich foods like nuts, avocados, and full-fat dairy, targeting a surplus of 500–1000 kcal/day to gain 0.5–1 kg/week. Use tools like food journals or apps to track intake and ensure consistency.
Caution: Avoid Extreme Measures
Post-hospitalization, the body is in a fragile state, and drastic diets or rapid weight changes can exacerbate health issues. For instance, crash dieting in obese individuals can lead to muscle loss and electrolyte imbalances, while aggressive weight gain in underweight patients may strain the cardiovascular system. Always prioritize balanced nutrition over speed. Hydration is equally critical; aim for 2–3 liters of water daily, adjusting for conditions like kidney disease or heart failure.
Step 2: Incorporate Safe Physical Activity
Movement is essential for BMI management, but post-hospitalization, it must be approached cautiously. For overweight individuals, start with low-impact exercises like walking, swimming, or yoga for 20–30 minutes daily, gradually increasing intensity as stamina improves. Underweight patients should focus on strength training to build muscle mass, starting with light resistance bands or bodyweight exercises 2–3 times weekly. Always consult a physical therapist or physician to design a safe, progressive program tailored to your recovery stage.
Analysis: Addressing Psychological Factors
BMI-related hospitalizations often stem from or lead to psychological challenges like stress, anxiety, or disordered eating. Cognitive-behavioral therapy (CBT) or support groups can provide tools to manage emotional triggers tied to eating habits. Mindfulness practices, such as meditation or journaling, can also foster a healthier relationship with food and body image. Ignoring mental health in recovery increases the risk of relapse, making it a critical component of long-term BMI management.
Takeaway: Consistency and Monitoring Are Key
Preventing re-admission requires sustained effort and vigilance. Regular follow-ups with healthcare providers to monitor BMI, blood work, and overall health are non-negotiable. Small, consistent changes in diet and activity yield better results than sporadic, intense efforts. Celebrate progress, no matter how incremental, and view setbacks as opportunities to learn rather than failures. By treating BMI management as a holistic, long-term commitment, you reduce the likelihood of returning to the hospital and improve overall quality of life.
Costing in Hospitality: Enhancing Profitability and Operational Efficiency
You may want to see also
Frequently asked questions
Hospitalization due to BMI often occurs when an individual’s BMI falls below 15 (severe underweight) or exceeds 50 (extreme obesity), as these levels pose significant health risks.
Yes, a very low BMI (below 15) can lead to hospitalization due to complications like malnutrition, organ failure, or severe eating disorders such as anorexia nervosa.
A high BMI (above 40) can cause hospitalization due to conditions like severe sleep apnea, heart failure, type 2 diabetes, or mobility-related injuries.
Hospitalization is typically necessary only if BMI-related complications arise, such as severe dehydration, electrolyte imbalances, or life-threatening obesity-related conditions.
The duration of hospitalization varies depending on the severity of the condition, ranging from a few days for stabilization to several weeks for intensive treatment or surgery.