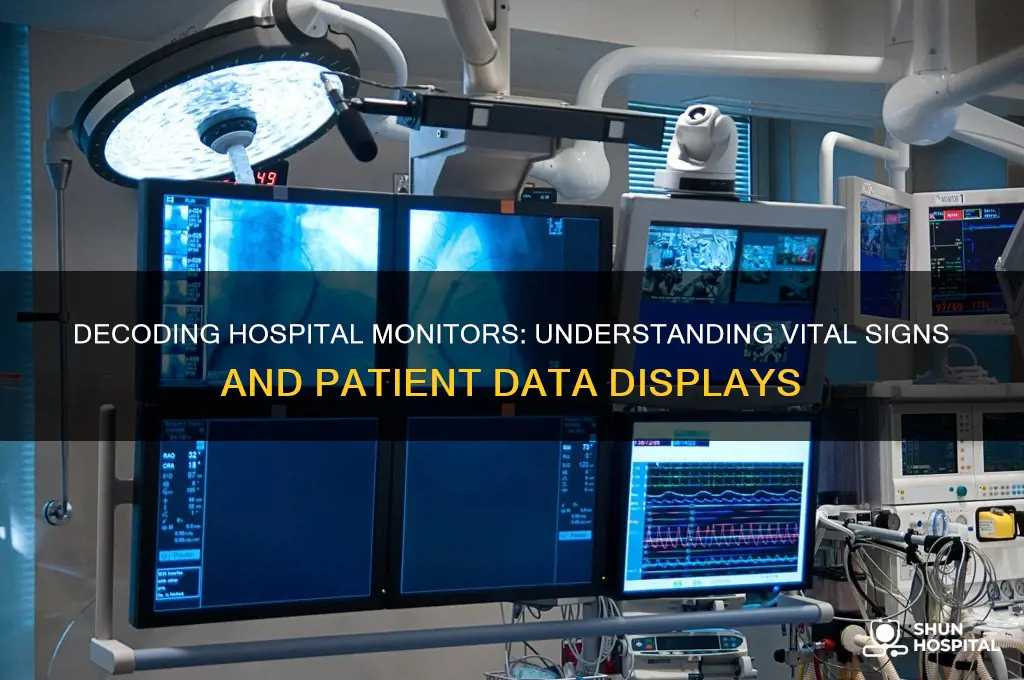
Hospital monitors are essential devices used in healthcare settings to continuously track and display vital physiological parameters of patients, ensuring timely intervention in critical situations. These monitors typically read key metrics such as heart rate, blood pressure, respiratory rate, oxygen saturation (SpO2), and body temperature, providing real-time data to healthcare professionals. Advanced monitors may also display electrocardiogram (ECG) readings, blood glucose levels, and other specialized parameters depending on the patient’s condition. The information displayed on these monitors is crucial for assessing a patient’s stability, detecting abnormalities, and guiding treatment decisions, making them indispensable tools in intensive care units, operating rooms, and emergency departments.
Explore related products






What You'll Learn
- Heart Rate Monitoring: Tracks beats per minute, indicating cardiac health and circulation status
- Blood Pressure Readings: Measures systolic/diastolic pressure to assess cardiovascular function
- Oxygen Saturation (SpO2): Evaluates oxygen levels in blood, vital for respiratory health
- Electrocardiogram (ECG): Records heart’s electrical activity to detect arrhythmias or damage
- Respiratory Rate: Monitors breaths per minute, reflecting lung function and overall health
![]()
Heart Rate Monitoring: Tracks beats per minute, indicating cardiac health and circulation status
Heart rate monitoring is a cornerstone of patient assessment in hospitals, offering a real-time window into cardiac function and overall circulation. By tracking beats per minute (BPM), clinicians can detect abnormalities that signal anything from stress to life-threatening conditions. A resting adult heart rate typically falls between 60 and 100 BPM, though athletes may exhibit rates as low as 40 BPM due to enhanced cardiac efficiency. Deviations from this range—tachycardia (elevated rate) or bradycardia (reduced rate)—prompt further investigation, often paired with other vital signs like blood pressure and oxygen saturation. This simple metric, when contextualized, becomes a powerful diagnostic tool.
Consider the scenario of a post-surgical patient whose heart rate climbs to 120 BPM while at rest. This could indicate pain, infection, or fluid imbalance, necessitating immediate intervention. Conversely, a sudden drop to 50 BPM in an elderly patient might reflect medication side effects or cardiac conduction issues. Continuous monitoring, often via bedside telemetry or wearable devices, allows healthcare teams to respond swiftly to such fluctuations. For instance, beta-blockers may be adjusted in a hypertensive patient if their heart rate remains persistently high despite adequate blood pressure control. Precision in interpretation hinges on understanding the patient’s baseline and clinical context.
Pediatric populations present unique challenges in heart rate monitoring. Newborns, for example, have a normal range of 100–160 BPM, while toddlers average 80–130 BPM. Failure to account for age-specific norms can lead to misdiagnosis. In children, a heart rate above 180 BPM often signals distress, such as dehydration or sepsis, requiring urgent attention. Parents and caregivers can use portable monitors at home to track trends, but should consult a pediatrician if readings consistently deviate from expected ranges. This proactive approach bridges the gap between hospital and home care, fostering early detection of potential issues.
Practical tips for accurate heart rate monitoring include ensuring the patient is at rest for at least 5 minutes before measurement and avoiding readings immediately after physical activity or emotional stress. For patients with arrhythmias, manual pulse checks over 60 seconds provide more reliable data than automated monitors, which may misinterpret irregular rhythms. Nurses and caregivers should document not only the rate but also the rhythm—regular, irregular, or ectopic—to aid in diagnosis. In critical care settings, integrating heart rate data with other parameters, such as respiratory rate and temperature, paints a comprehensive picture of the patient’s condition.
Ultimately, heart rate monitoring transcends mere number-tracking; it’s a dynamic narrative of cardiac health and systemic circulation. Whether in the ICU, emergency department, or outpatient clinic, this vital sign serves as an early warning system, guiding treatment decisions and improving outcomes. By mastering its interpretation and application, healthcare providers can transform raw data into actionable insights, ensuring timely and targeted care for every patient.
Good Samaritan Hospital: A Trauma Center?
You may want to see also
Explore related products






![]()
Blood Pressure Readings: Measures systolic/diastolic pressure to assess cardiovascular function
Blood pressure readings are a cornerstone of patient monitoring in hospitals, offering critical insights into cardiovascular health. These readings measure two key values: systolic pressure, the force exerted on artery walls when the heart beats, and diastolic pressure, the force when the heart rests between beats. Together, they provide a snapshot of how effectively the heart is pumping blood and how much resistance the blood encounters in the arteries. For instance, a reading of 120/80 mmHg indicates a systolic pressure of 120 and a diastolic pressure of 80, which is considered optimal for most adults. Understanding these numbers is essential for diagnosing conditions like hypertension, hypotension, or cardiovascular disease, making blood pressure monitoring a vital tool in both routine check-ups and emergency care.
Interpreting blood pressure readings requires context, as values can vary based on age, health status, and even the time of day. For adults, systolic pressure below 120 mmHg and diastolic below 80 mmHg is generally healthy, while readings consistently above 130/80 mmHg may indicate hypertension. In children, normal ranges differ significantly; for example, a 6-year-old typically has a systolic pressure around 95 mmHg, while a teenager’s may be closer to 110 mmHg. Hospital monitors often use automated cuffs that inflate and deflate to measure these pressures, providing quick and accurate results. However, manual auscultation with a stethoscope and sphygmomanometer remains a gold standard for precision, especially in critical care settings.
The practical application of blood pressure readings extends beyond diagnosis. For patients with hypertension, lifestyle modifications such as reducing sodium intake, increasing physical activity, and managing stress can help lower systolic and diastolic pressures. Medications like ACE inhibitors or beta-blockers may be prescribed for more severe cases, with dosages tailored to individual needs. For instance, a patient with a systolic pressure of 160 mmHg might start with 10 mg of lisinopril daily, adjusted based on response. Monitoring blood pressure regularly allows healthcare providers to track progress and adjust treatment plans effectively, ensuring optimal cardiovascular function.
One often overlooked aspect of blood pressure readings is their role in predicting long-term health outcomes. Elevated systolic pressure, in particular, is a strong predictor of stroke, heart attack, and kidney disease. For example, a sustained systolic pressure above 140 mmHg increases the risk of coronary artery disease by 50%. Hospitals use this data not only to manage acute conditions but also to educate patients on preventive measures. Simple tips like using a home blood pressure monitor, maintaining a balanced diet, and avoiding smoking can significantly reduce cardiovascular risks. By focusing on both immediate and long-term implications, blood pressure readings serve as a powerful tool for proactive healthcare.
In hospital settings, blood pressure monitoring is often integrated into continuous patient surveillance systems, especially in intensive care units. These systems alert healthcare providers to sudden changes, such as a drop in systolic pressure below 90 mmHg, which could indicate shock or dehydration. Rapid intervention in such cases can be life-saving. For example, a patient post-surgery might require intravenous fluids or vasopressors to stabilize their blood pressure. This real-time data ensures that medical teams can respond swiftly to fluctuations, maintaining cardiovascular stability and improving patient outcomes. Whether in routine care or critical situations, blood pressure readings remain indispensable in hospital monitoring.
Shiftboard: Streamlining Hospital and Clinic Scheduling for Optimal Efficiency
You may want to see also
Explore related products






![]()
Oxygen Saturation (SpO2): Evaluates oxygen levels in blood, vital for respiratory health
Oxygen saturation, often abbreviated as SpO2, is a critical metric measured by hospital monitors to assess the percentage of oxygen-saturated hemoglobin in the blood relative to the total hemoglobin. Typically displayed as a percentage, a normal SpO2 level ranges between 95% and 100% for healthy individuals. Values below 90% are considered low and may indicate hypoxemia, a condition where the blood is not adequately oxygenated, posing serious risks to organ function. This measurement is non-invasive, usually obtained via a pulse oximeter clipped to a patient’s finger, toe, or earlobe, making it a convenient yet essential tool in clinical settings.
The importance of SpO2 monitoring cannot be overstated, particularly in respiratory care. Conditions such as chronic obstructive pulmonary disease (COPD), asthma, pneumonia, and COVID-19 often compromise lung function, directly affecting oxygen uptake. For instance, during a severe asthma attack, airway constriction can reduce oxygen exchange, leading to SpO2 levels dropping below 92%. In such cases, supplemental oxygen therapy is administered to restore levels to a safe range, typically targeting 92–96% for most patients, though specific goals may vary based on underlying conditions like COPD, where lower targets (88–92%) are sometimes acceptable to avoid CO2 retention.
Monitoring SpO2 is not limited to acute care; it plays a pivotal role in post-operative recovery, sleep studies, and home health management. For example, patients with sleep apnea may experience nocturnal desaturation events, where SpO2 levels plummet during apneic episodes. Continuous monitoring helps diagnose such conditions and evaluate the efficacy of treatments like CPAP therapy. Similarly, pediatric patients, especially premature infants, require close SpO2 surveillance due to underdeveloped lungs, with target ranges often set between 91% and 95% to balance oxygenation and potential retinal damage from excessive oxygen exposure.
While pulse oximetry is highly reliable, certain factors can skew readings. Dark nail polish, cold extremities, poor circulation, and movement artifacts may lead to inaccurate measurements. Clinicians must verify suspicious readings through arterial blood gas analysis, the gold standard for assessing oxygenation. Additionally, SpO2 monitors do not measure oxygen delivery to tissues or ventilation adequacy, underscoring the need for holistic patient assessment. Despite these limitations, SpO2 remains a cornerstone of respiratory monitoring, offering real-time insights that guide timely interventions and improve patient outcomes.
Distance from Eastern Illinois University to Decatur Memorial Hospital
You may want to see also
Explore related products






![]()
Electrocardiogram (ECG): Records heart’s electrical activity to detect arrhythmias or damage
The electrocardiogram (ECG) is a cornerstone of cardiac monitoring, capturing the heart’s electrical impulses through a series of waves and intervals. By placing electrodes on the chest, arms, and legs, the ECG translates these signals into a visual graph, revealing patterns like the P wave (atrial depolarization), QRS complex (ventricular depolarization), and T wave (ventricular repolarization). Deviations from normal waveforms—such as prolonged QT intervals or irregular QRS complexes—can indicate arrhythmias, ischemia, or structural damage. For instance, a flattened T wave may suggest myocardial ischemia, while a missing P wave could signal atrial fibrillation. Understanding these patterns is critical for timely diagnosis and intervention.
Interpreting an ECG requires both precision and context. A standard 12-lead ECG provides a comprehensive view of the heart’s electrical activity from multiple angles, allowing clinicians to localize abnormalities. For example, ST-segment elevation in leads II, III, and aVF often points to inferior wall myocardial infarction. However, factors like age, medication use, and electrolyte imbalances can confound readings. A 60-year-old patient with chest pain and an ECG showing ST depression in leads V4-V6 warrants immediate attention, as this could indicate posterior wall ischemia. Always correlate ECG findings with clinical symptoms and additional tests like troponin levels for accurate assessment.
For healthcare providers, mastering ECG interpretation is a skill honed through practice and education. Start by familiarizing yourself with normal values: a heart rate of 60–100 bpm, PR interval of 0.12–0.20 seconds, and QRS duration of 0.06–0.10 seconds. Use systematic approaches like the "I inspect, I interpret, I integrate" method: inspect the rhythm and rate, interpret waveforms and intervals, and integrate findings with patient history. Online resources, such as ECG libraries or simulation tools, can aid learning. For trainees, practicing on diverse cases—from sinus tachycardia to ventricular fibrillation—builds confidence and accuracy.
Patients undergoing ECG monitoring should be aware of its non-invasive nature and minimal risks. The procedure typically takes 5–10 minutes, with no pain or downtime. However, anxiety or movement can distort readings, so remaining still and relaxed is essential. If a 24-hour Holter monitor is prescribed, patients should maintain a diary of symptoms and activities to correlate with ECG data. For those with implantable loop recorders, understanding that these devices continuously monitor for arrhythmias over months to years can alleviate concerns. Clear communication with healthcare providers ensures that ECG results are interpreted accurately and acted upon promptly.
In critical care settings, continuous ECG monitoring is indispensable for detecting life-threatening arrhythmias like ventricular tachycardia or bradycardia. Nurses and physicians must be vigilant for alarm triggers, such as heart rates below 40 bpm or above 140 bpm, and respond according to protocol. For instance, a patient with a heart rate of 180 bpm and regular rhythm may require intravenous adenosine (6–12 mg) to terminate paroxysmal supraventricular tachycardia. Conversely, a patient with a heart rate of 35 bpm and dizziness may need transcutaneous pacing or atropine (0.5–1 mg IV). Proactive monitoring and swift action can prevent complications and save lives.
Analytical Chemists: Enhancing Hospital Diagnostics and Patient Care
You may want to see also
Explore related products






![]()
Respiratory Rate: Monitors breaths per minute, reflecting lung function and overall health
Hospital monitors are the silent sentinels of patient care, tracking vital signs that reveal the body’s internal state. Among these, respiratory rate—the number of breaths per minute—stands as a critical yet often overlooked metric. A normal adult breathes 12 to 20 times per minute at rest, but deviations signal trouble. For instance, a rate below 12 may indicate respiratory depression, often seen in opioid overdose or severe head injury, while a rate above 25 suggests distress, common in pneumonia or heart failure. Pediatric norms differ: newborns breathe 30–60 times per minute, toddlers 20–30, and school-aged children 18–25. These ranges underscore why respiratory rate is a non-negotiable parameter in hospital monitoring.
Monitoring respiratory rate isn’t just about counting breaths—it’s about interpreting what those numbers mean for lung function and overall health. For example, rapid, shallow breathing (tachypnea) can indicate acid buildup in the blood, a hallmark of diabetic ketoacidosis or sepsis. Conversely, slow, labored breathing (bradypnea) may reflect opioid toxicity or brainstem dysfunction. Nurses and clinicians use this data to triage patients, adjust treatments, and predict outcomes. A sudden increase in respiratory rate, for instance, might prompt a chest X-ray to rule out pulmonary embolism. Thus, this metric serves as both a diagnostic tool and an early warning system.
To measure respiratory rate accurately, clinicians observe chest rise and fall for a full minute, especially in non-verbal patients or those with cognitive impairments. Automated monitors, while convenient, can miss nuances like Cheyne-Stokes respiration (periodic breathing) or Kussmaul respirations (deep, rapid breathing in metabolic acidosis). Practical tips include ensuring the patient is at rest, as anxiety or pain can artificially elevate the rate. For children, distraction techniques—like counting objects in a picture—prevent hyperventilation from nervousness. Accurate measurement is key, as even small errors can lead to misdiagnosis or delayed intervention.
Comparatively, respiratory rate is often overshadowed by more dramatic vitals like heart rate or blood pressure, yet it’s equally predictive of deterioration. Studies show that an elevated respiratory rate is a stronger predictor of in-hospital mortality than other single parameters. It’s also a core component of early warning scores (e.g., NEWS2), which stratify patients by risk. Despite its importance, respiratory rate remains underutilized in some settings due to time constraints or reliance on technology. Advocates argue for its prioritization, citing cases where timely recognition of abnormal breathing saved lives. In this light, respiratory rate isn’t just a number—it’s a narrative of the body’s struggle or resilience.
Finally, integrating respiratory rate into routine monitoring requires education and protocol adherence. Hospitals should train staff to recognize abnormal patterns and act swiftly. For instance, a post-operative patient with a respiratory rate of 28 warrants oxygen therapy and potential reversal of sedatives. Home caregivers can also monitor breathing patterns in chronic conditions like COPD, using portable pulse oximeters to track rate and oxygen saturation. By elevating respiratory rate from a passive observation to an active diagnostic tool, healthcare providers can enhance patient safety and outcomes. After all, every breath counts—literally.
Jak pocieszyć chorego w szpitalu: przydatne zwroty po polsku
You may want to see also
Frequently asked questions
Hospital monitors typically read vital signs such as heart rate, blood pressure, respiratory rate, oxygen saturation (SpO2), and body temperature. Some advanced monitors may also display electrocardiogram (ECG) readings, blood pressure trends, and other specific parameters depending on the patient’s condition.
Hospital monitors measure oxygen levels in the blood using a pulse oximeter, which is a non-invasive device clipped onto a patient’s finger, toe, or earlobe. It emits light through the skin to measure the amount of oxygen bound to hemoglobin in the blood, displaying the result as SpO2 (oxygen saturation percentage).
Yes, hospital monitors can detect irregular heart rhythms through ECG (electrocardiogram) readings. They track the electrical activity of the heart and display it as a waveform, allowing healthcare providers to identify abnormalities such as arrhythmias, tachycardia, or bradycardia.