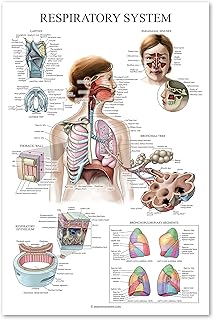
A respiratory therapist plays a critical role in hospitals by specializing in the assessment, treatment, and management of patients with breathing difficulties and cardiopulmonary disorders. These healthcare professionals work across various hospital settings, including intensive care units, emergency departments, and neonatal wards, to provide life-saving care for patients of all ages. Their responsibilities include administering oxygen therapy, managing ventilators, performing diagnostic tests like arterial blood gas analysis, and educating patients on breathing exercises and disease management. Respiratory therapists also collaborate with physicians and other healthcare teams to develop and implement treatment plans, ensuring optimal respiratory function and improving patients’ quality of life. Their expertise is particularly vital in treating conditions such as asthma, chronic obstructive pulmonary disease (COPD), pneumonia, and acute respiratory distress syndrome (ARDS).
| Characteristics | Values |
|---|---|
| Patient Care | Provide direct care to patients with respiratory conditions, including assessing, diagnosing, and treating breathing disorders. |
| Ventilator Management | Manage and monitor mechanical ventilators for patients who cannot breathe on their own. |
| Airway Management | Perform procedures such as intubation, tracheostomy care, and suctioning to maintain clear airways. |
| Oxygen Therapy | Administer oxygen therapy and monitor patients' oxygen levels to ensure adequate respiratory function. |
| Pulmonary Function Testing | Conduct tests to measure lung capacity, volumes, and gas exchange, aiding in diagnosis and treatment planning. |
| Inhalation Therapy | Administer inhaled medications and nebulizer treatments to manage conditions like asthma and COPD. |
| Emergency Response | Respond to respiratory emergencies, such as cardiac arrests, by providing immediate interventions like CPR and airway management. |
| Patient Education | Educate patients and their families on respiratory care, disease management, and the use of home respiratory equipment. |
| Collaborative Care | Work closely with physicians, nurses, and other healthcare professionals to develop and implement patient care plans. |
| Equipment Maintenance | Ensure respiratory equipment is properly maintained, calibrated, and functioning correctly. |
| Documentation | Maintain detailed patient records, including treatment plans, progress notes, and test results. |
| Specialized Care | Provide specialized care in areas like neonatal, pediatric, or adult critical care, depending on their certification and expertise. |
| Research and Development | Participate in research studies to advance respiratory care practices and technologies. |
| Infection Control | Follow strict protocols to prevent the spread of respiratory infections, especially in high-risk areas like ICUs. |
| Rehabilitation | Assist in pulmonary rehabilitation programs to help patients improve lung function and overall health. |
| Ethical Practice | Adhere to ethical standards and patient confidentiality in all aspects of care. |
Explore related products






What You'll Learn
- Patient Assessment: Evaluate lung function, medical history, and symptoms to determine appropriate respiratory care
- Oxygen Therapy: Administer oxygen via masks, nasal cannulas, or ventilators to improve breathing
- Airway Management: Clear airways using suctioning, chest physiotherapy, and breathing exercises
- Ventilator Care: Monitor and adjust mechanical ventilators for critically ill patients
- Emergency Response: Assist in codes, CPR, and acute respiratory distress interventions
![]()
Patient Assessment: Evaluate lung function, medical history, and symptoms to determine appropriate respiratory care
Respiratory therapists are often the first line of defense in identifying and addressing respiratory distress, a condition that can rapidly deteriorate if left untreated. Patient assessment is a critical skill in their arsenal, requiring a meticulous approach to evaluate lung function, medical history, and symptoms. This process is not merely a checklist but a dynamic interplay of clinical judgment and technical expertise.
The Art of Observation and Inquiry
A thorough patient assessment begins with keen observation. Respiratory therapists note subtle cues like labored breathing, accessory muscle use, or cyanosis, which can indicate hypoxia. Simultaneously, they engage patients in detailed questioning, probing for symptoms such as wheezing, coughing, or chest tightness. For instance, a patient with a history of COPD might present with increased sputum production, signaling an exacerbation. Pediatric patients, especially those under 5, may exhibit retractions or nasal flaring, requiring age-specific interpretation. The therapist must also consider environmental factors, such as exposure to allergens or pollutants, which can exacerbate conditions like asthma.
Tools of the Trade: Measuring Lung Function
Objective data is paramount in respiratory care. Therapists employ tools like spirometry to measure forced vital capacity (FVC) and forced expiratory volume in one second (FEV1), critical for diagnosing obstructive or restrictive lung diseases. For patients unable to perform spirometry, peak flow meters offer a simpler alternative. Arterial blood gas (ABG) analysis provides insights into oxygenation and acid-base balance, with normal PaO2 levels ranging from 75 to 100 mmHg. Therapists must interpret these results in context—a PaO2 of 60 mmHg in a COPD patient might be their baseline, while it would indicate severe hypoxia in a healthy adult.
Medical History: Uncovering Hidden Clues
A patient’s medical history is a treasure trove of information. Therapists scrutinize records for conditions like heart failure, which can cause pulmonary edema, or cystic fibrosis, associated with recurrent infections. Medication lists are equally vital—beta-blockers, for example, can trigger bronchospasm in asthmatics. Therapists also assess compliance with prescribed therapies, such as inhaler use or CPAP for sleep apnea. For elderly patients, polypharmacy and comorbidities like diabetes can complicate respiratory care, necessitating tailored interventions.
Synthesizing Data for Actionable Care
The final step in patient assessment is synthesizing findings to devise a care plan. For instance, a patient with a history of asthma, presenting with a FEV1 of 50% predicted and a PaO2 of 70 mmHg, might require bronchodilators like albuterol (2.5 mg via nebulizer) and systemic steroids. Therapists must also anticipate risks—a postoperative patient with reduced lung function might need incentive spirometry to prevent atelectasis. This holistic approach ensures that interventions are not only evidence-based but also patient-centered, addressing both immediate needs and long-term management.
Mastering patient assessment allows respiratory therapists to bridge the gap between diagnosis and treatment, ensuring that every breath counts. Their ability to integrate clinical findings with technical data transforms lives, particularly in acute settings where timely intervention is critical.
Boston Hospitals: Preparedness Exemplified
You may want to see also
Explore related products





![]()
Oxygen Therapy: Administer oxygen via masks, nasal cannulas, or ventilators to improve breathing
Respiratory therapists are often the first line of defense in managing acute and chronic respiratory conditions, and oxygen therapy is one of their most critical interventions. Administering oxygen via masks, nasal cannulas, or ventilators is a precise science, requiring careful assessment of the patient’s oxygenation status and tailored delivery methods. For instance, a nasal cannula, which delivers 24% to 40% oxygen at flow rates of 1–6 liters per minute, is ideal for patients with mild to moderate hypoxemia, such as those with COPD or pneumonia. In contrast, non-rebreather masks, delivering up to 90% oxygen at 10–15 liters per minute, are reserved for severe cases like respiratory distress or trauma. The choice of device depends on the patient’s needs, with therapists continuously monitoring oxygen saturation levels to avoid complications like oxygen toxicity or hypercapnia.
The process of administering oxygen therapy involves more than just attaching a device to a patient. Respiratory therapists must first evaluate the patient’s medical history, current condition, and arterial blood gas results to determine the appropriate oxygen concentration and flow rate. For example, a patient with chronic obstructive pulmonary disease (COPD) may require lower oxygen concentrations (e.g., 24–28%) to avoid suppressing their respiratory drive, while a post-surgical patient might need higher levels temporarily. Therapists also educate patients on proper device use, such as ensuring nasal cannula prongs fit snugly or teaching them how to use a ventilator interface. This hands-on approach ensures both efficacy and patient comfort, reducing anxiety and improving adherence to therapy.
One of the most complex applications of oxygen therapy is its use in mechanical ventilation, where respiratory therapists play a pivotal role. Ventilators deliver oxygen under pressure, often in intensive care units, for patients with severe respiratory failure, such as those with ARDS or post-operative complications. Therapists must adjust settings like tidal volume (typically 6–8 mL/kg of predicted body weight), PEEP (positive end-expiratory pressure), and FiO2 (fraction of inspired oxygen) to optimize lung function while minimizing injury. For instance, high PEEP levels (e.g., 10–15 cm H2O) may be used to recruit collapsed alveoli in ARDS patients, but this requires careful monitoring to avoid barotrauma. The therapist’s expertise ensures that ventilation supports breathing without causing harm, making them indispensable in critical care settings.
Despite its life-saving benefits, oxygen therapy is not without risks, and respiratory therapists are trained to mitigate these. Prolonged exposure to high oxygen concentrations can lead to absorption atelectasis or oxidative stress, particularly in neonates and patients with chronic lung disease. Therapists must also watch for signs of respiratory acidosis in COPD patients, who may retain CO2 when given excessive oxygen. Practical tips include using humidified oxygen to prevent mucosal drying and regularly assessing skin integrity around mask or cannula sites to avoid pressure injuries. By balancing the therapeutic benefits with potential risks, respiratory therapists ensure oxygen therapy remains a safe and effective intervention across diverse patient populations.
Washington Hospital: Non-Profit Healthcare for All
You may want to see also
Explore related products






![]()
Airway Management: Clear airways using suctioning, chest physiotherapy, and breathing exercises
Respiratory therapists are often the first line of defense in ensuring patients can breathe effectively, especially in critical care settings. One of their most vital roles is airway management, which involves clearing obstructions and optimizing lung function. This is achieved through techniques like suctioning, chest physiotherapy, and breathing exercises, each tailored to the patient’s specific needs. These interventions are not one-size-fits-all; they require precision, skill, and an understanding of the patient’s condition, whether it’s a child with cystic fibrosis or an elderly patient recovering from pneumonia.
Suctioning is a cornerstone of airway management, particularly for patients who cannot clear their own secretions. Respiratory therapists use sterile catheters connected to a suction device to remove mucus, blood, or other obstructions from the airway. The process must be performed carefully to avoid trauma to the airway mucosa. For example, in pediatric patients, therapists use smaller catheters and apply suction for no more than 5–10 seconds at a time, as prolonged suctioning can lead to hypoxia. In adults, the technique may involve deeper insertion and controlled negative pressure, typically between -200 to -300 mmHg, depending on the patient’s tolerance and the severity of the obstruction. Proper technique is critical to prevent complications like bronchospasm or airway injury.
Chest physiotherapy complements suctioning by mobilizing secretions, making them easier to clear. This involves manual techniques such as percussion (clapping on the chest or back) and vibration, which dislodge mucus from the airway walls. Postural drainage is another key component, positioning the patient so gravity helps move secretions toward the upper airway. For instance, a patient with a right lower lobe consolidation might be positioned in a left side-lying, head-down position for 10–15 minutes. Chest physiotherapy is particularly effective in patients with conditions like COPD or cystic fibrosis, where mucus buildup is a chronic issue. However, it requires careful assessment of the patient’s cardiovascular stability, as the procedure can increase oxygen demand.
Breathing exercises are the third pillar of airway management, focusing on improving lung expansion and gas exchange. Therapists teach patients techniques like diaphragmatic breathing, pursed-lip breathing, and incentive spirometry. Diaphragmatic breathing, for example, encourages the use of the diaphragm rather than accessory muscles, reducing the work of breathing. This is especially beneficial for patients with acute respiratory distress or post-surgical patients who need to prevent atelectasis. Incentive spirometry, often used after abdominal or thoracic surgery, involves inhaling through a device to improve lung volumes. Patients are typically instructed to take 10–15 breaths per hour, aiming for a target volume displayed on the device. These exercises not only clear airways but also empower patients to actively participate in their recovery.
While these techniques are effective, they are not without risks. Over-suctioning can lead to hypoxia or barotrauma, chest physiotherapy may exacerbate fatigue in debilitated patients, and improper breathing exercises can strain already compromised respiratory systems. Respiratory therapists must balance the benefits of these interventions with potential drawbacks, continuously monitoring patients for signs of distress. For instance, if a patient becomes tachycardic or desaturates during chest physiotherapy, the session should be paused or modified. Ultimately, airway management is a dynamic process, requiring therapists to adapt their approach based on real-time patient responses and evolving clinical conditions.
HCA Hospitals: Unlocking Cellular Plan Discounts for Employees and Patients
You may want to see also
Explore related products






![]()
Ventilator Care: Monitor and adjust mechanical ventilators for critically ill patients
Mechanical ventilation is a lifeline for critically ill patients whose lungs cannot sustain adequate oxygenation or carbon dioxide removal on their own. Respiratory therapists are the primary specialists responsible for managing these life-support systems, ensuring they function optimally while minimizing risks like ventilator-induced lung injury (VILI). This task demands precision, as even minor adjustments to settings like tidal volume (typically 6–8 mL/kg of predicted body weight) or positive end-expiratory pressure (PEEP, often titrated between 5–15 cm H₂O) can significantly impact patient outcomes. Without constant monitoring and expert intervention, mechanical ventilation can become a double-edged sword, exacerbating rather than alleviating respiratory distress.
The process begins with assessing the patient’s condition through waveform analysis, arterial blood gas (ABG) interpretation, and clinical observation. For instance, a rising plateau pressure (>30 cm H₂O) signals increased airway resistance or lung stiffness, requiring immediate intervention to prevent barotrauma. Respiratory therapists must also consider the patient’s age, comorbidities, and disease severity; a 70-year-old with acute respiratory distress syndrome (ARDS) may tolerate lower tidal volumes (4–6 mL/kg) compared to a younger patient with asthma. Adjustments are made incrementally, balancing oxygenation goals (PaO₂ 55–80 mmHg) with the risk of over-ventilation.
One critical aspect of ventilator care is weaning—gradually reducing mechanical support as the patient’s lungs recover. This involves daily assessments using tools like the Rapid Shallow Breathing Index (RSBI), where a score <105 suggests readiness for extubation. However, premature weaning can lead to reintubation, which increases mortality risk by up to 40%. Therapists must therefore weigh objective data against subjective cues, such as patient fatigue or anxiety, to determine the optimal timing. Protocols like spontaneous breathing trials (SBTs), conducted for 30–120 minutes, provide structured frameworks for this decision-making process.
Cautions abound in ventilator management, particularly in pediatric and neonatal populations. Infants, for example, require specialized modes like high-frequency oscillatory ventilation (HFOV) due to their immature lungs and higher compliance. Overlooking details like circuit humidification can lead to mucus plugging, while inadequate sedation monitoring may result in patient-ventilator asynchrony, prolonging dependence. Respiratory therapists must stay vigilant, cross-checking alarms, and troubleshooting issues like air leaks or circuit obstructions in real time.
In conclusion, ventilator care is both an art and a science, requiring technical expertise, critical thinking, and empathy. By meticulously monitoring parameters, interpreting data, and tailoring interventions to individual needs, respiratory therapists play a pivotal role in bridging the gap between machine and patient. Their decisions directly influence survival rates, length of stay, and long-term pulmonary function, making them indispensable members of the critical care team. Mastery of this skill set transforms mechanical ventilation from a mere intervention into a carefully orchestrated therapy, restoring life’s most fundamental rhythm—the breath.
Understanding the Role of the Department of Health and Human Services
You may want to see also
Explore related products






![]()
Emergency Response: Assist in codes, CPR, and acute respiratory distress interventions
In the high-stakes environment of a hospital, respiratory therapists are often the first responders to life-threatening respiratory emergencies. When a "code blue" is called, signaling cardiac or respiratory arrest, these specialists spring into action, their expertise in airway management and ventilation becoming the linchpin of survival. Unlike nurses or physicians, respiratory therapists bring a focused skill set to the code team, ensuring that oxygenation and ventilation are optimized during CPR and defibrillation. Their presence can mean the difference between a successful resuscitation and a tragic outcome.
Consider the mechanics of CPR: while chest compressions are critical, they only circulate existing oxygen in the bloodstream. Without proper ventilation, oxygen levels plummet, rendering compressions ineffective. Respiratory therapists step in to secure airways, often using advanced techniques like endotracheal intubation or supraglottic airway devices. For instance, during a code, a therapist might administer 100% oxygen via a bag-valve mask, ensuring maximal oxygen delivery with each breath. In pediatric cases, they adjust tidal volumes to 5–7 mL/kg to avoid barotrauma, a precision that general responders may lack.
Acute respiratory distress syndrome (ARDS) presents another arena where respiratory therapists shine. This condition, often triggered by sepsis, pneumonia, or trauma, causes fluid buildup in the lungs, drastically reducing oxygen exchange. Therapists employ strategies like prone positioning—placing patients face down to improve ventilation—or adjust ventilator settings to deliver low tidal volumes (6 mL/kg) and higher PEEP (positive end-expiratory pressure) to keep alveoli open. For example, a patient with ARDS might require PEEP levels of 12–15 cm H2O, a delicate balance that only a trained therapist can manage to prevent lung injury.
The role of respiratory therapists in emergency response extends beyond technical skills to leadership and coordination. During a code, they often direct the team on ventilation timing, ensuring it doesn’t interfere with compressions. In ARDS cases, they collaborate with intensivists to interpret arterial blood gas results and fine-tune therapies. This dual role as both technician and strategist underscores their indispensability in crises. Without their intervention, even the most well-executed CPR or ventilator support could fail to address the root of respiratory failure.
Finally, the psychological demands of this role cannot be overlooked. Responding to codes or managing ARDS patients requires resilience and quick thinking under pressure. Therapists must remain calm while making split-second decisions, such as whether to initiate high-flow nasal cannula therapy or switch to non-invasive ventilation. Their ability to act decisively, backed by deep knowledge of respiratory physiology, transforms them from support staff into frontline heroes in the battle against respiratory emergencies. In hospitals, their hands-on expertise is not just beneficial—it’s vital.
Hospital Discharge Essentials: Is a Car Seat Mandatory for Newborns?
You may want to see also
Frequently asked questions
A respiratory therapist assesses, treats, and manages patients with breathing difficulties or cardiopulmonary disorders. They administer medications, perform diagnostic tests, and operate equipment like ventilators to support patient breathing.
Yes, respiratory therapists work with patients of all ages, from newborns to the elderly, in various hospital settings, including intensive care units, emergency rooms, and neonatal wards.
Respiratory therapists provide treatments such as oxygen therapy, aerosol medications, chest physiotherapy, and mechanical ventilation. They also educate patients on breathing exercises and disease management.
Respiratory therapists work closely with physicians, nurses, and other healthcare providers to develop and implement patient care plans. They play a critical role in emergency response teams and participate in multidisciplinary rounds.