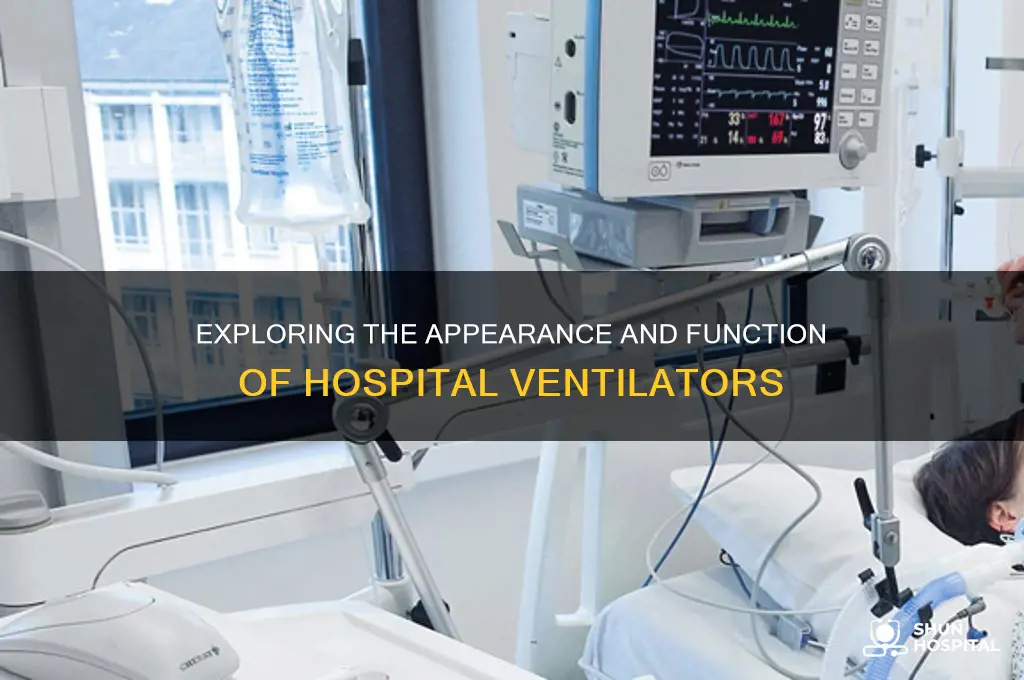
A ventilator, a critical piece of medical equipment in hospitals, is a life-support machine designed to assist or take over the breathing process for patients who cannot breathe adequately on their own. Typically, it appears as a bedside device with a control panel featuring a digital display, various buttons, and dials for adjusting settings such as airflow, oxygen levels, and pressure. Connected to the ventilator is a circuit with tubes that deliver air and oxygen to the patient through an endotracheal tube or mask. The machine often includes alarms and monitors to alert healthcare providers to any changes in the patient’s condition, ensuring precise and continuous respiratory support. Its compact yet robust design allows it to be easily integrated into intensive care units, where it plays a vital role in saving lives.
Explore related products






What You'll Learn
- Ventilator Components: Tubes, monitors, alarms, and settings for air pressure, volume, and oxygen levels
- Machine Design: Compact, wheeled, with a screen, buttons, and a breathing circuit attached
- Patient Connection: Mask or tube inserted into the airway for assisted breathing
- Hospital Placement: Commonly found in ICUs, emergency rooms, and recovery wards
- Brand Variations: Different models (e.g., portable, ICU-grade) with similar core features
![]()
Ventilator Components: Tubes, monitors, alarms, and settings for air pressure, volume, and oxygen levels
A ventilator, often the centerpiece of critical care in hospitals, is a complex yet life-sustaining machine. Its appearance can be intimidating, but understanding its components demystifies its function. At its core, a ventilator is a symphony of tubes, monitors, alarms, and precise settings for air pressure, volume, and oxygen levels, all working in harmony to support breathing.
Consider the tubes first—the lifeline of the ventilator. These include the endotracheal tube, which connects directly to the patient’s airway, and the inspiratory/expiratory tubes that deliver and remove air. Tubes are typically color-coded for clarity: blue for inspiratory (oxygen-rich air) and white for expiratory (exhaled air). Proper tube placement is critical; misalignment can lead to complications like pneumothorax. For pediatric patients, tubes are smaller in diameter, often ranging from 3.0 to 5.0 mm, while adults may require sizes between 7.0 and 9.0 mm.
Monitors and alarms serve as the ventilator’s nervous system, providing real-time feedback and alerts. Monitors display vital parameters such as tidal volume (typically 6–8 mL/kg for adults), respiratory rate (12–20 breaths/min), and oxygen saturation (targeting 92–96%). Alarms are calibrated to trigger at specific thresholds—for instance, a high-pressure alarm may sound if airway pressure exceeds 30 cmH₂O, signaling a potential obstruction. Nurses and respiratory therapists must interpret these alarms swiftly, balancing the need for immediate action with the risk of alarm fatigue.
Settings for air pressure, volume, and oxygen levels are the ventilator’s control panel, fine-tuned to meet individual patient needs. Pressure control modes, like Pressure Support, assist spontaneous breathing by maintaining a set pressure (e.g., 10–15 cmH₂O). Volume control modes deliver a fixed tidal volume, often used in sedated patients. Oxygen levels, adjusted via the FiO₂ (fraction of inspired oxygen), range from 21% (room air) to 100%, depending on the patient’s condition. For ARDS patients, FiO₂ may start at 60–100% to maintain adequate oxygenation.
Practical tips for healthcare providers include double-checking tube connections before initiating ventilation, ensuring alarms are audible but not overly sensitive, and documenting all setting changes. For families, understanding that the ventilator’s noises and alarms are normal can reduce anxiety. In essence, the ventilator’s components are not just mechanical parts but tools of precision, designed to bridge the gap between life and breath.
Beaumont Hospital's County Location in El Paso, Texas Explained
You may want to see also
Explore related products






![]()
Machine Design: Compact, wheeled, with a screen, buttons, and a breathing circuit attached
In the critical care environment of a hospital, ventilators are indispensable, and their design reflects a balance between functionality and user accessibility. A compact, wheeled ventilator is a common sight, often resembling a small cart with a vertical tower housing the essential components. This design choice is deliberate, allowing the machine to be easily maneuvered to the patient's bedside, a crucial feature in dynamic hospital settings where space is at a premium. The wheels, typically lockable, ensure stability during operation and mobility when needed.
The front panel of such a ventilator is a hub of activity, featuring a screen and an array of buttons that serve as the primary interface for healthcare professionals. The screen, often a high-resolution display, provides real-time data on the patient's respiratory status, including tidal volume, respiratory rate, and oxygen concentration. This visual feedback is critical for clinicians to make informed adjustments, ensuring the patient receives the appropriate level of support. For instance, a typical adult patient might require a tidal volume of 6-8 ml/kg of predicted body weight, a setting easily monitored and modified via this interface.
Below the screen, a series of buttons and dials allow for precise control of ventilation parameters. These controls are designed with ergonomics in mind, enabling quick adjustments without compromising accuracy. For example, a simple turn of a dial can increase the oxygen flow rate from 40% to 100% in emergency situations, while dedicated buttons might allow for the selection of different ventilation modes, such as volume-controlled or pressure-controlled ventilation, each suited to specific patient needs.
Attached to the ventilator is the breathing circuit, a critical component that connects the machine to the patient. This circuit typically consists of a series of tubes, filters, and humidifiers, ensuring the air delivered to the patient is sterile, warm, and moist, mimicking natural breathing conditions. The circuit's design is crucial for preventing infections and ensuring patient comfort, especially in long-term ventilation scenarios. Regular maintenance, such as changing filters every 24-48 hours, is essential to maintain the circuit's integrity.
The compact, wheeled design with an integrated screen, controls, and breathing circuit represents a thoughtful approach to ventilator engineering. It prioritizes ease of use, patient safety, and adaptability in various clinical scenarios. This design philosophy ensures that ventilators are not just life-support devices but also tools that empower healthcare providers to deliver precise and responsive care. Whether in an intensive care unit or an emergency department, this type of ventilator design plays a pivotal role in modern medical practice, offering a blend of technology and practicality.
Economic Boom, Hospital Bust: Unraveling the Financial Crisis in Healthcare
You may want to see also
Explore related products






![]()
Patient Connection: Mask or tube inserted into the airway for assisted breathing
The patient connection to a ventilator is a critical interface where life-sustaining technology meets human physiology. Whether through a mask or an endotracheal tube, this connection ensures oxygen delivery and carbon dioxide removal when a patient’s lungs cannot function independently. The choice between a mask and a tube depends on the patient’s condition, the duration of ventilation, and the clinical judgment of the healthcare team. Masks, such as non-invasive ventilation (NIV) interfaces, are often used for patients with mild to moderate respiratory distress, while tubes are reserved for more severe cases requiring full mechanical support.
Mask-based ventilation, such as continuous positive airway pressure (CPAP) or bilevel positive airway pressure (BiPAP), is less invasive and more comfortable for the patient. These masks cover the nose and mouth, delivering pressurized air to keep the airways open. They are commonly used for conditions like chronic obstructive pulmonary disease (COPD) exacerbations or sleep apnea. However, masks require patient cooperation and may not be suitable for those with severe respiratory failure or altered mental status. Proper mask fit is essential to prevent air leaks, which can reduce the effectiveness of the therapy.
In contrast, endotracheal intubation involves inserting a tube directly into the trachea, bypassing the upper airway. This method is used for patients who cannot maintain their airway, have severe respiratory failure, or require prolonged ventilation. The tube is secured in place with tape or a specialized holder and connected to the ventilator via a circuit. Intubation is an invasive procedure performed by trained professionals, often in emergency or intensive care settings. Once in place, the tube allows for precise control of oxygen and pressure delivery, making it ideal for critically ill patients.
The decision to use a mask or tube is guided by factors such as the patient’s oxygen saturation levels, respiratory rate, and overall stability. For instance, a patient with an oxygen saturation below 90% despite supplemental oxygen may require intubation. Conversely, a patient with mild hypoxia and a stable airway might benefit from a mask-based approach. Healthcare providers also consider the risk of complications, such as ventilator-associated pneumonia (VAP), which is more common with intubation due to the direct airway invasion.
Practical tips for caregivers include ensuring the mask is snug but not tight to avoid skin irritation, regularly checking the tube’s position to prevent displacement, and monitoring for signs of discomfort or distress in the patient. For long-term ventilation, tracheostomy—a surgically created opening in the neck—may be considered to provide a more permanent and comfortable airway access. Regardless of the method, continuous monitoring of vital signs and ventilator settings is crucial to optimize patient outcomes and minimize complications. Understanding these patient connections is key to effective ventilator management in hospital settings.
Little Company of Mary Hospital Location: A Comprehensive Guide to Finding It
You may want to see also
Explore related products






![]()
Hospital Placement: Commonly found in ICUs, emergency rooms, and recovery wards
Ventilators are a critical component of modern healthcare, and their placement within a hospital is strategic, reflecting the urgency and complexity of patient needs. In Intensive Care Units (ICUs), ventilators are a staple, often occupying a central position beside patient beds. These machines are life-sustaining, providing essential respiratory support to critically ill patients, such as those with severe pneumonia, acute respiratory distress syndrome (ARDS), or post-surgical complications. The ICU environment is designed for constant monitoring, with ventilators connected to a network of sensors and alarms, ensuring immediate response to any deviations in a patient's condition. For instance, a typical ICU ventilator setup might include a mechanical ventilator with adjustable pressure and volume settings, catering to patients ranging from neonates to adults, with specific modes like pressure control ventilation for ARDS patients, often requiring tidal volumes of 6-8 ml/kg to prevent lung injury.
In the fast-paced environment of emergency rooms (ERs), ventilators serve a different yet equally vital role. Here, they are deployed rapidly to stabilize patients in acute respiratory distress, such as trauma victims or those experiencing severe asthma attacks. ER ventilators are often portable and easily maneuverable, allowing healthcare providers to quickly initiate mechanical ventilation in high-stress situations. A common scenario might involve a patient with a severe anaphylactic reaction, where a ventilator is used to deliver a high flow of oxygen, sometimes with the addition of heliox (a mixture of helium and oxygen) to reduce airway resistance, a technique particularly useful in pediatric cases.
The recovery ward, or step-down unit, presents a unique setting for ventilator use. Patients here are typically transitioning from critical care, requiring less intensive support but still benefiting from assisted ventilation. Ventilators in these areas are often used in weaning modes, gradually reducing support to encourage spontaneous breathing. This process is carefully managed, with protocols dictating the gradual decrease in pressure support levels, typically by 2-4 cm H2O per day, while monitoring for signs of respiratory fatigue or distress. For example, a patient recovering from a prolonged ICU stay might be placed on a ventilator with a pressure support level of 10 cm H2O, which is then reduced daily until they can breathe independently.
The strategic placement of ventilators in these hospital settings is not arbitrary but is guided by the specific needs of the patient population. ICUs demand high-acuity ventilators with advanced features, ERs require rapid deployment and portability, while recovery wards focus on weaning and rehabilitation. Each setting has its own set of challenges and requirements, influencing the design and functionality of the ventilators used. For instance, ventilators in ICUs often have integrated systems for delivering inhaled nitric oxide (iNO) for patients with severe hypoxemia, a feature less critical in other areas.
Understanding the hospital placement of ventilators is crucial for healthcare professionals and administrators alike. It ensures that the right equipment is available in the right place at the right time, optimizing patient care and resource utilization. For instance, knowing that ER ventilators need to be portable and quickly deployable can guide purchasing decisions, while awareness of the weaning protocols in recovery wards can inform staff training and patient management strategies. This knowledge is particularly valuable in resource-limited settings, where efficient allocation of ventilators can significantly impact patient outcomes.
In summary, the placement of ventilators in hospitals is a strategic decision, tailored to the unique demands of ICUs, emergency rooms, and recovery wards. Each setting requires specific ventilator features and capabilities, from advanced monitoring in ICUs to portability in ERs and weaning modes in recovery areas. Recognizing these differences is essential for effective patient care, resource management, and staff training, ultimately contributing to improved health outcomes.
Trauma Care: Doctors Hospital's Emergency Services
You may want to see also
Explore related products






![]()
Brand Variations: Different models (e.g., portable, ICU-grade) with similar core features
Ventilators in hospitals come in various models, each tailored to specific needs yet sharing essential core features. For instance, ICU-grade ventilators are robust, stationary units designed for critical care, offering advanced settings like pressure control and volume-cycled modes. In contrast, portable ventilators are lightweight, battery-operated devices ideal for transport or home use, often featuring simplified interfaces and fewer modes. Despite these differences, both types ensure consistent oxygen delivery, monitor patient vitals, and include alarms for safety—core functions critical to their purpose.
Consider the use case to determine the right model. ICU-grade ventilators are indispensable in intensive care units, where patients require precise, continuous support. For example, a patient with acute respiratory distress syndrome (ARDS) might need a ventilator set to deliver 6–8 mL/kg of tidal volume and 8–10 cmH₂O of positive end-expiratory pressure (PEEP). Portable ventilators, on the other hand, are ideal for patients transitioning from hospital to home or those with chronic conditions like COPD. These devices often weigh under 10 pounds and can operate on battery power for 4–6 hours, ensuring mobility without compromising care.
From a design perspective, both models prioritize user-friendliness and reliability. ICU ventilators typically feature large touchscreens and multiple ports for monitoring and adjusting settings, while portable units streamline controls for ease of use. For instance, a portable ventilator might have a single knob to adjust flow rate and a button to toggle between assist and control modes. Despite these differences, both incorporate fail-safes like backup power and alarm systems to prevent interruptions in care.
When selecting a ventilator, healthcare providers must balance patient needs with practical considerations. ICU-grade models, though expensive and immobile, offer the precision required for critical cases. Portable ventilators, while less versatile, provide flexibility for less acute scenarios. For example, a patient recovering from pneumonia might start on an ICU ventilator but transition to a portable model for rehabilitation. Understanding these brand variations ensures the right tool is chosen for the right situation, optimizing patient outcomes.
In summary, while ventilators vary in size, complexity, and application, their core features remain consistent across models. Whether stationary or portable, each device is engineered to deliver oxygen, monitor patient status, and ensure safety. By focusing on these shared functions and tailoring the choice to the patient’s condition, healthcare providers can navigate brand variations effectively, delivering targeted care with confidence.
Tackling Excessive Hospital Charges: Strategies for Patients to Fight Back
You may want to see also
Frequently asked questions
A ventilator in a hospital typically resembles a small machine with a digital display, control buttons, and a breathing tube connected to a patient’s airway. It often has wheels for mobility and is equipped with alarms and monitoring screens.
No, ventilators can vary in size and design. Some are compact and portable, while others are larger and stationary, depending on their intended use and features.
Visible components include a breathing tube, air filters, a display screen, control panels, alarms, and ports for connecting to oxygen or air supplies.
Ventilators are typically neutral in color, such as white, gray, or beige, to blend with hospital equipment and maintain a sterile appearance.





























