
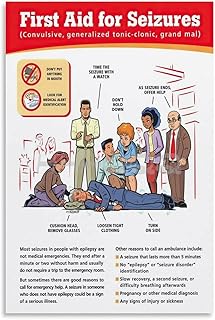
In hospitals, having immediate access to essential emergency equipment is critical for effectively managing seizures, which can range from mild to life-threatening. Key items should include a crash cart with medications like benzodiazepines (e.g., lorazepam or diazepam) for rapid seizure control, oxygen delivery systems to ensure adequate respiration, and suction devices to prevent aspiration. Additionally, a bite block or padded tongue depressor can protect the patient’s airway, while a timer or clock helps monitor seizure duration. Proximity to a defibrillator is vital for addressing cardiac complications, and soft restraints or padding should be available to prevent injury during convulsions. Ensuring this equipment is readily accessible in high-risk areas like emergency departments and inpatient units can significantly improve patient outcomes during seizure events.
| Characteristics | Values |
|---|---|
| Oxygen Therapy | Oxygen source (e.g., oxygen tank, wall outlet), nasal cannula, mask |
| Airway Management | Suction device, oral/nasal airway, bag-valve-mask (BVM), laryngoscope |
| Monitoring Equipment | Pulse oximeter, blood pressure monitor, ECG machine, capnography |
| Medications | Benzodiazepines (e.g., lorazepam, diazepam), anticonvulsants (e.g., IV phenytoin) |
| Timing Device | Stopwatch or timer to monitor seizure duration |
| Protective Padding | Soft pads or blankets to prevent injury during convulsions |
| IV Access | IV supplies (e.g., catheter, saline, tape) for rapid medication delivery |
| Seizure Alarm | Wearable or bed-based seizure detection devices (if available) |
| Emergency Protocols | Clear, accessible guidelines for seizure management |
| Patient Positioning Aids | Log roll pillow or wedge to maintain side-lying position |
| Communication Tools | Emergency call system or phone for rapid response team activation |
| Personal Protective Equipment (PPE) | Gloves, gown, mask for healthcare providers |
| Documentation Tools | Chart or electronic system for recording seizure details and interventions |
| Lighting Control | Dimmable lights or eye protection to reduce sensory overload |
| Temperature Monitoring | Thermometer to check for fever, which may trigger seizures |
| Glucose Monitoring | Glucometer and glucose supplies to rule out hypoglycemia |
Explore related products





What You'll Learn
- Defibrillator Access: Ensure AEDs are nearby for cardiac emergencies during or after seizures
- Oxygen Supply: Quick access to oxygen tanks and masks for respiratory distress
- Suction Devices: Essential for clearing airways of vomit or secretions during seizures
- Protective Padding: Soft pads or helmets to prevent head injuries from falls
- Emergency Medications: Stock benzodiazepines (e.g., lorazepam) for prolonged or severe seizures
![]()
Defibrillator Access: Ensure AEDs are nearby for cardiac emergencies during or after seizures
Seizures can trigger cardiac complications, including arrhythmias or sudden cardiac arrest, particularly in individuals with pre-existing heart conditions or prolonged seizure activity. Ensuring immediate access to automated external defibrillators (AEDs) is critical in hospital settings, where rapid response can mean the difference between life and death. AEDs are designed for ease of use, providing voice prompts and visual instructions to guide even untrained bystanders through the defibrillation process. Hospitals must strategically place these devices in high-traffic areas, such as emergency departments, neurology wards, and intensive care units, to minimize response time during a cardiac emergency.
The placement of AEDs should follow a systematic approach, considering both accessibility and visibility. Wall-mounted units with clear signage are ideal, ensuring they are not obstructed by equipment or furniture. Regular drills and training sessions for staff can reinforce familiarity with AED locations and operation, reducing hesitation during emergencies. For pediatric patients, hospitals should stock AEDs with adjustable energy settings, as children require lower defibrillation doses—typically 2 to 4 joules per kilogram for infants and 4 joules per kilogram for older children—compared to adults, who receive a standard shock of 120 to 200 joules.
While AEDs are user-friendly, their effectiveness relies on prompt activation. Hospitals should implement protocols that prioritize AED retrieval alongside seizure management, such as administering oxygen and ensuring airway patency. For instance, if a patient experiences a prolonged seizure (status epilepticus) followed by cardiac instability, the simultaneous use of anti-seizure medications like benzodiazepines and AED preparation can optimize outcomes. Coordination among healthcare teams is essential to avoid delays, as every minute without defibrillation reduces survival rates by 7-10% in cardiac arrest cases.
Comparing AED access in hospitals versus public spaces highlights the advantage of a controlled healthcare environment. Unlike public AEDs, which may be underutilized due to fear or lack of awareness, hospital staff are trained to act swiftly. However, this advantage is nullified if AEDs are not readily available. Hospitals should conduct periodic audits of AED placement and functionality, including battery checks and pad expiration dates, to ensure reliability. By treating AED access as a non-negotiable component of seizure emergency preparedness, hospitals can better safeguard patients from the potentially fatal cardiac consequences of seizures.
Streamlining Healthcare: Effective Hospital Management Strategies
You may want to see also
Explore related products





![]()
Oxygen Supply: Quick access to oxygen tanks and masks for respiratory distress
Seizures can lead to respiratory distress, a life-threatening complication where breathing becomes labored or stops altogether. During a seizure, the body’s normal breathing patterns may be disrupted, causing hypoxia—a dangerous lack of oxygen to the brain and vital organs. Immediate access to oxygen supply is critical in these moments, as it can stabilize the patient until the seizure subsides or further medical intervention is administered. Without prompt oxygen administration, the risk of permanent brain damage or death increases significantly.
In a hospital setting, oxygen tanks and masks should be strategically placed in every area where seizures are likely to occur, such as emergency departments, neurology wards, and intensive care units. Portable oxygen tanks with flowmeters are ideal, as they allow for rapid adjustment of oxygen delivery rates. For adults, a typical initial oxygen flow rate ranges from 4 to 10 liters per minute, depending on the severity of respiratory distress. Pediatric patients require lower flow rates, typically 1 to 2 liters per minute for infants and 2 to 4 liters per minute for older children, adjusted based on weight and clinical condition. Always use a mask that fits securely to minimize oxygen leakage and ensure effective delivery.
The process of administering oxygen during a seizure must be seamless and efficient. Staff should be trained to recognize signs of respiratory distress, such as cyanosis (bluish skin), gasping, or irregular breathing. Once identified, the oxygen mask should be applied immediately, with the flow rate set to deliver high-concentration oxygen (80-100%). If the patient is unconscious or unable to breathe effectively, bag-mask ventilation may be necessary, using a self-inflating bag attached to the oxygen source. Continuous monitoring of oxygen saturation levels via pulse oximetry is essential to guide adjustments in oxygen therapy.
While oxygen is a critical intervention, it is not without risks. Over-oxygenation can occur, particularly in patients with chronic lung conditions like COPD, leading to respiratory acidosis. To mitigate this, healthcare providers should aim to provide the lowest oxygen concentration necessary to maintain adequate oxygen saturation, typically above 92% for adults and 94% for children. Additionally, oxygen tanks must be regularly inspected to ensure they are fully charged and functional, as empty or malfunctioning equipment can delay treatment during a critical moment.
In summary, quick access to oxygen tanks and masks is non-negotiable in hospital settings where seizures are managed. Proper placement, staff training, and adherence to dosage guidelines ensure that respiratory distress is addressed swiftly and effectively. By prioritizing oxygen supply as part of seizure emergency protocols, hospitals can significantly reduce the risk of complications and improve patient outcomes during these high-stakes events.
Personal Health and Hygiene: Essential Practices in Hospitality Excellence
You may want to see also
Explore related products




![]()
Suction Devices: Essential for clearing airways of vomit or secretions during seizures
Seizures can lead to vomiting or excessive salivation, both of which pose immediate risks of airway obstruction. Suction devices are critical in these moments, providing a rapid and effective means to clear the airway and prevent aspiration pneumonia or suffocation. Portable suction units, such as the ASPITRA® or similar models, are ideal for hospital settings due to their maneuverability and consistent suction power, typically ranging from 80 to 500 mmHg. These devices should be pre-assembled with sterile catheters (sizes 10–14 French for adults, 6–8 French for children) and placed within arm’s reach of seizure response areas.
The process of using a suction device requires precision to avoid trauma to the airway mucosa. Insert the catheter no deeper than necessary—generally 10–15 cm for adults—and apply intermittent suction (2–3 seconds at a time) rather than continuous pulling. Over-suctioning can cause hypoxia, so limit each pass to less than 10 seconds. For pediatric patients, use lower suction pressures (below 100 mmHg) and smaller catheters to minimize risk. Always have a backup device or manual suction bulb available in case of mechanical failure.
Hospitals should prioritize training staff in suction techniques as part of seizure response protocols. Simulation drills can reinforce proper catheter insertion angles (30–45 degrees for adults) and the importance of monitoring oxygen saturation during the procedure. Additionally, ensure suction devices are regularly maintained: check battery life on portable units, replace filters, and confirm tubing is free of cracks or blockages. A malfunctioning device in an emergency is a preventable hazard.
While suction devices are indispensable, they are not a standalone solution. Pair their use with positioning the patient in the recovery position (head tilted downward) to facilitate drainage. For patients with recurrent seizures or known aspiration risks, consider pre-emptively placing a suction catheter nearby during monitoring. This proactive approach can save critical seconds when a seizure occurs. In all cases, suctioning should be followed by immediate reassessment of airway patency and oxygenation status.
Should You Visit Your Ex-Girlfriend in the Hospital? A Guide
You may want to see also
Explore related products





![]()
Protective Padding: Soft pads or helmets to prevent head injuries from falls
Seizures can lead to sudden falls, making head injuries a significant risk. Protective padding, such as soft pads or helmets, serves as a critical safeguard in hospital settings. These devices are designed to absorb impact, reducing the likelihood of skull fractures, concussions, or intracranial bleeding. While they may not eliminate all risks, their presence can mitigate the severity of injuries, particularly in patients with frequent or unpredictable seizures.
Instructive guidelines for implementing protective padding emphasize proper fit and placement. Helmets should be adjustable, ensuring a snug but comfortable fit without restricting blood flow or causing discomfort. Soft pads, often made of foam or gel, can be strategically placed on hard surfaces like floors or bedside tables. For pediatric patients, age-appropriate designs are essential, as children’s heads are proportionally larger and more vulnerable to injury. Regular checks for wear and tear are also crucial, as damaged padding loses its protective efficacy.
A comparative analysis highlights the advantages of helmets over traditional soft pads in certain scenarios. Helmets provide 360-degree protection, making them ideal for patients with violent or prolonged seizures. However, they may be less practical for long-term use due to heat retention and potential social stigma. Soft pads, on the other hand, are more discreet and versatile, suitable for targeted protection in high-risk areas. Hospitals often adopt a combination approach, tailoring solutions to individual patient needs and seizure characteristics.
Persuasively, the cost-benefit analysis of protective padding is undeniable. While the initial investment in quality padding may seem significant, it pales in comparison to the financial and emotional costs of treating head injuries. Studies show that hospitals incorporating such measures experience fewer seizure-related complications, leading to shorter hospital stays and reduced healthcare expenditures. Moreover, the peace of mind for both patients and caregivers is invaluable, fostering a safer and more trusting care environment.
Descriptively, imagine a hospital room equipped with protective padding: a soft, contoured helmet rests on a bedside table, ready for immediate use, while foam pads line the floor beneath the bed. These simple yet effective tools transform the space into a safer haven for seizure-prone patients. Their presence is a tangible reminder of the hospital’s commitment to proactive, patient-centered care, blending functionality with compassion.
Dr. Jeffrey Prem's Surgical Practice at Aultman Hospital: Facts Revealed
You may want to see also
Explore related products




![]()
Emergency Medications: Stock benzodiazepines (e.g., lorazepam) for prolonged or severe seizures
In the critical moments of managing prolonged or severe seizures, benzodiazepines like lorazepam are indispensable. These medications act rapidly to suppress abnormal electrical activity in the brain, making them the first-line treatment for status epilepticus—a life-threatening condition where seizures persist for more than five minutes or occur repeatedly without recovery. Lorazepam, in particular, is favored for its quick onset (within 1-3 minutes when administered intravenously) and high efficacy, even in refractory cases. Its availability in pre-filled syringes or vials ensures immediate access, a crucial factor when every second counts.
Administering lorazepam requires precision and adherence to protocols. The standard adult dose is 4 mg given intravenously over 2 minutes, with an additional 4 mg after 10-15 minutes if seizures persist. For pediatric patients, the dose is weight-based, typically 0.1 mg/kg, with a maximum of 4 mg per dose. Caution is advised in elderly patients or those with respiratory compromise, as benzodiazepines can depress breathing. Monitoring vital signs, particularly respiratory rate and oxygen saturation, is essential during and after administration.
The choice of lorazepam over other benzodiazepines, such as diazepam, is often driven by its water solubility, which eliminates the need for propylene glycol—a solvent associated with rare but severe adverse reactions. Additionally, lorazepam’s longer half-life provides sustained anticonvulsant effects, reducing the likelihood of seizure recurrence. However, its intravenous route necessitates trained personnel and access to a secure IV line, highlighting the need for preparedness in hospital settings.
Stocking lorazepam in emergency carts or code trays ensures it is immediately available in seizure emergencies. Hospitals should maintain a sufficient supply, with regular checks to ensure vials or pre-filled syringes are within their expiration dates and stored properly. Staff training on dosage, administration, and monitoring is equally critical, as errors can lead to oversedation or respiratory depression. In resource-limited settings, having a clear protocol for rapid procurement or alternative administration methods (e.g., intramuscular or intranasal routes) can be lifesaving.
Ultimately, benzodiazepines like lorazepam are not just medications—they are a lifeline in the acute management of severe seizures. Their presence in hospital emergency equipment is non-negotiable, but their effectiveness hinges on proper storage, accessibility, and skilled administration. By prioritizing these factors, healthcare facilities can ensure timely intervention, minimizing the risk of seizure-related complications and improving patient outcomes.
Hospitals and CT Scans: 24/7 Emergency Care
You may want to see also
Frequently asked questions
Essential equipment includes oxygen delivery systems (e.g., nasal cannula or mask), suction devices, a bite block or padded tongue depressor, a timer or clock to monitor seizure duration, and access to emergency medications like benzodiazepines (e.g., lorazepam or diazepam).
A bite block or padded tongue depressor is used to prevent the patient from biting their tongue or injuring their mouth during a seizure. It should be placed between the molars, not the front teeth, to avoid blocking the airway.
Emergency medications like benzodiazepines should be stored in a readily accessible location, clearly labeled, and pre-prepared in pre-drawn syringes or auto-injectors (e.g., diazepam rectal gel) to ensure quick administration. Staff should be trained in proper dosing and routes of administration.































