Sacred Heart Hospital in Cumberland, Maryland, holds a significant place in the region's history, serving as a cornerstone of healthcare for the community for many decades. Established in the early 20th century, the hospital was known for its dedication to providing compassionate care to residents of Allegany County and beyond. However, as healthcare landscapes evolved and financial pressures mounted, Sacred Heart faced numerous challenges. In the late 20th and early 21st centuries, the hospital struggled to remain viable, ultimately leading to its closure in 2009. The shutdown marked the end of an era, leaving many to wonder about the circumstances that led to its demise and the lasting impact on the community. Today, the story of Sacred Heart Hospital serves as a poignant reminder of the complexities surrounding rural healthcare and the resilience of the communities it once served.
Explore related products





What You'll Learn
![]()
Hospital closure reasons
Sacred Heart Hospital in Cumberland, MD, closed its doors in 2009, leaving a void in the community’s healthcare landscape. This closure was not an isolated incident but part of a broader trend affecting rural and small-town hospitals across the United States. Financial strain emerged as the primary culprit, driven by declining reimbursement rates from Medicare and Medicaid, which accounted for over 60% of the hospital’s patient base. When operational costs outpace revenue, even essential services become unsustainable, forcing difficult decisions.
Consider the role of population shifts in hospital viability. Cumberland’s population had been steadily declining since the 1980s, mirroring the economic downturn in Western Maryland’s coal and manufacturing industries. Fewer residents meant fewer patients, and the hospital’s average daily census dropped below 50% capacity in its final years. This underutilization exacerbated financial losses, as fixed costs like staffing and maintenance remained constant while revenue dwindled. For hospitals in similar situations, monitoring census trends and adjusting service models proactively could mitigate risk.
Another critical factor was the inability to compete with larger, better-equipped facilities in nearby metropolitan areas. Patients increasingly sought care at hospitals with advanced technology and specialized services, leaving smaller institutions like Sacred Heart struggling to retain market share. Investments in modern equipment or specialty care were prohibitively expensive, creating a cycle of obsolescence. Hospitals in this predicament might explore partnerships or mergers to pool resources, though such arrangements require careful negotiation to preserve local access to care.
Finally, workforce challenges played a significant role in Sacred Heart’s closure. Rural hospitals often face difficulties recruiting and retaining physicians, nurses, and other healthcare professionals. Sacred Heart’s staffing shortages led to reduced service hours and delayed patient care, further driving patients to alternative facilities. Addressing this issue requires creative solutions, such as offering loan forgiveness programs for healthcare workers in underserved areas or leveraging telemedicine to bridge gaps in expertise.
In summary, Sacred Heart Hospital’s closure was the culmination of financial pressures, demographic changes, competitive disadvantages, and workforce shortages. For communities at risk of losing their hospitals, understanding these interconnected challenges is the first step toward developing strategies to preserve local healthcare access. While no single solution fits all scenarios, a combination of financial restructuring, community engagement, and innovative service delivery models can help sustain vital healthcare services in vulnerable areas.
Hospital Lifting Devices: How Many Are There?
You may want to see also
Explore related products






![]()
Impact on local healthcare
The closure of Sacred Heart Hospital in Cumberland, MD, in 2009 left a significant void in the local healthcare landscape. This 116-bed facility, a cornerstone of the community for over a century, provided essential services, including emergency care, maternity services, and specialized treatments. Its sudden shutdown forced residents to seek alternatives, often traveling greater distances to access comparable care. This disruption highlights the critical role such institutions play in maintaining the health and well-being of rural and underserved populations.
Analyzing the aftermath reveals a cascade of challenges. Emergency response times increased as patients were redirected to hospitals in neighboring towns, sometimes over 30 miles away. This delay can be life-threatening in critical cases, such as heart attacks or strokes, where every minute counts. For instance, the "golden hour" in trauma care—the first 60 minutes after injury—became harder to achieve, potentially worsening outcomes. Additionally, the loss of maternity services meant expectant mothers faced longer commutes, increasing the risk of complications during childbirth.
To mitigate these impacts, local health departments and remaining providers implemented stopgap measures. Mobile health clinics were deployed to offer basic services, and telemedicine programs were expanded to address non-urgent needs. However, these solutions are not without limitations. Telemedicine, while convenient, cannot replace hands-on care for complex conditions. Similarly, mobile clinics lack the capacity to handle emergencies or provide advanced diagnostics. These efforts, though commendable, underscore the need for a more sustainable healthcare infrastructure.
A comparative look at similar closures nationwide reveals a recurring pattern: rural hospitals often struggle with financial viability due to declining populations, lower reimbursement rates, and high operational costs. Sacred Heart’s closure was no exception, driven by mounting debts and insufficient funding. This trend suggests that without targeted policy interventions, such as increased federal funding or incentives for rural healthcare providers, more communities may face similar crises. For Cumberland, the loss of Sacred Heart serves as a cautionary tale, emphasizing the fragility of local healthcare systems and the urgent need for proactive solutions.
Practical steps can be taken to strengthen healthcare resilience in areas vulnerable to hospital closures. First, investing in community health workers can bridge gaps in access, providing preventive care and health education. Second, partnerships between local governments and private healthcare providers can fund essential services. For example, a public-private collaboration could establish a smaller, specialized clinic to address the most pressing needs, such as maternity care or chronic disease management. Finally, advocating for policy changes, like Medicaid expansion or rural hospital grants, can provide the financial stability needed to sustain these institutions. By learning from Cumberland’s experience, other communities can better prepare to safeguard their healthcare futures.
Great Ormond Street Hospital: Size and Impact
You may want to see also
Explore related products






![]()
Former staff and patient stories
The closure of Sacred Heart Hospital in Cumberland, MD, left a void not just in healthcare services but in the personal histories of those who worked and healed within its walls. Former staff and patients carry with them stories that illuminate the hospital’s impact, its challenges, and its legacy. These narratives, often shared in local forums or oral histories, reveal a tapestry of dedication, resilience, and loss. For instance, a former nurse recalls the hospital’s role as a lifeline for the community, particularly during the coal mining era, when injuries were frequent and care was scarce. Such accounts underscore the hospital’s place as more than a building—it was a cornerstone of Cumberland’s identity.
Analyzing these stories, a recurring theme emerges: the human connection fostered within Sacred Heart’s walls. Patients describe nurses who remembered their favorite meals or doctors who explained complex diagnoses with uncommon patience. Staff members speak of a tight-knit family, where long shifts were endured together and triumphs were celebrated collectively. One former physician notes how the hospital’s smaller size allowed for personalized care, a stark contrast to the impersonal nature of larger medical centers. These anecdotes highlight the intangible value of community-based healthcare, a lesson often overlooked in discussions of efficiency and profitability.
To preserve these stories, consider creating a digital or physical archive where former staff and patients can contribute their experiences. Practical steps include organizing community events, such as storytelling nights or oral history workshops, and using platforms like local libraries or social media to collect and share memories. For example, a 72-year-old former patient, who underwent a life-saving surgery at Sacred Heart in the 1980s, could record a video testimonial detailing the care received and its long-term impact. Such efforts not only honor the past but also provide a resource for future generations to understand the hospital’s significance.
Comparatively, the stories of Sacred Heart’s closure offer a cautionary tale about the fragility of rural healthcare. Staff members recount the gradual decline in resources, from outdated equipment to staffing shortages, which ultimately led to the hospital’s demise. Patients describe the disorientation of being redirected to distant facilities, often lacking the familiarity and trust they once relied on. These experiences serve as a reminder that hospitals are not just institutions but lifelines, and their loss reverberates far beyond medical services. By documenting these stories, we can advocate for sustainable healthcare models that prioritize community needs over financial gains.
Finally, the legacy of Sacred Heart Hospital lives on through the people it touched. A former nurse now volunteers at a local clinic, inspired by the care she witnessed and provided. A patient who received critical treatment as a child has since become a healthcare advocate, pushing for policies that protect rural hospitals. These examples demonstrate how individual experiences can catalyze broader change. By amplifying these stories, we not only preserve the memory of Sacred Heart but also inspire action to safeguard the future of healthcare in communities like Cumberland.
Signs of Appendicitis: When to Head to the Hospital
You may want to see also
Explore related products






![]()
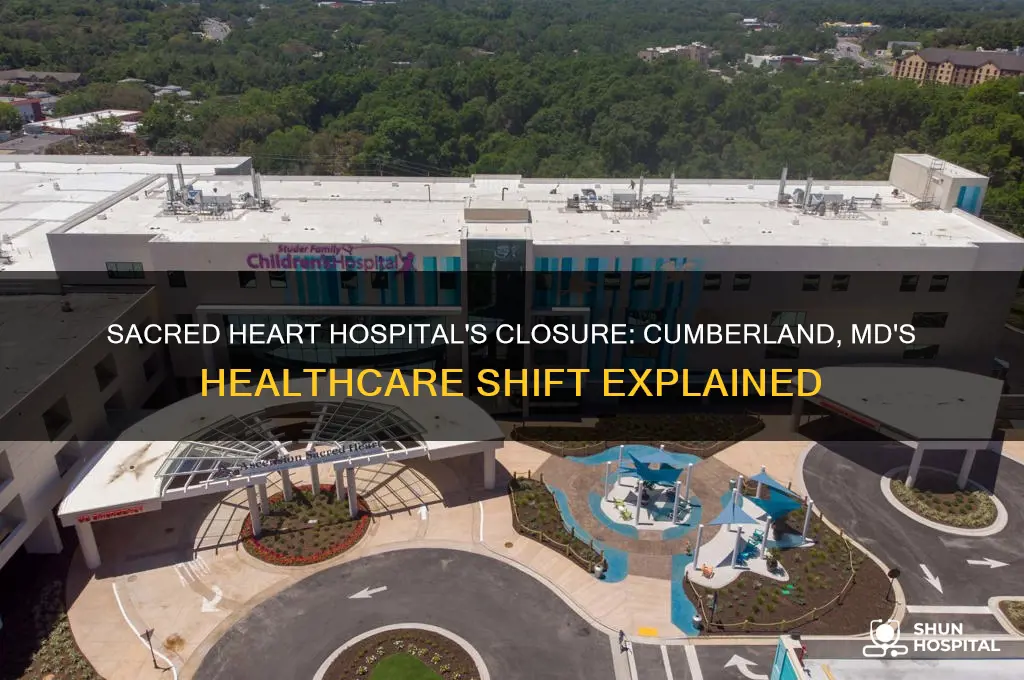
Building’s current status
Sacred Heart Hospital in Cumberland, MD, once a cornerstone of the community, now stands as a relic of the past, its current status a blend of neglect and potential. The building, which ceased operations in 2009 due to financial struggles and consolidation efforts, has since become a subject of local concern and curiosity. Its brick facade, once a symbol of healing, now bears the marks of time—cracked windows, peeling paint, and overgrown vegetation. Despite its deterioration, the structure retains a haunting beauty, a silent witness to decades of medical care and community life.
Analyzing the building’s current state reveals a complex interplay of challenges and opportunities. Structurally, the hospital remains intact, though years of exposure to the elements have taken their toll. The interior, once bustling with activity, is now a maze of empty corridors and abandoned equipment, a stark reminder of its former purpose. Local authorities and preservationists face a dilemma: demolition would erase a piece of history, while restoration requires significant investment. The question of whether to preserve or repurpose the building remains a contentious issue, with no clear resolution in sight.
For those considering the building’s future, practical steps can guide decision-making. First, conduct a thorough structural assessment to determine the extent of damage and feasibility of restoration. Second, explore potential uses, such as converting the space into affordable housing, a community center, or a mixed-use development. Third, engage stakeholders—local residents, historians, and investors—to gather input and build consensus. Caution must be taken to avoid hasty decisions that could lead to irreversible loss of historical value or financial strain.
Comparatively, Sacred Heart Hospital’s fate mirrors that of many defunct hospitals nationwide, where aging infrastructure meets dwindling resources. However, Cumberland’s unique history and the building’s central location offer a distinct advantage. Unlike rural hospitals that fade into obscurity, Sacred Heart’s urban setting presents opportunities for adaptive reuse, blending preservation with modern needs. Cities like Pittsburgh and Detroit have successfully transformed abandoned hospitals into vibrant hubs, offering a blueprint for Cumberland’s future.
Descriptively, the building’s current status evokes a sense of melancholy and possibility. Its towering presence dominates the skyline, a ghostly monument to a bygone era. Yet, within its walls lies untapped potential—spacious rooms, sturdy foundations, and a prime location. Imagine revitalized halls buzzing with activity, or a rooftop garden overlooking the city. With vision and investment, Sacred Heart Hospital could once again become a beacon of hope, not for patients, but for a community seeking renewal.
Which Hospital is Featured in Prodigal Son?
You may want to see also
Explore related products






![]()
Community response and legacy
The closure of Sacred Heart Hospital in Cumberland, MD, left a void that the community has been actively working to fill, blending grief with resilience. Residents organized grassroots initiatives to repurpose the hospital’s resources, such as donating medical equipment to local clinics and converting parts of the facility into a community health hub. These efforts highlight how collective action can mitigate the loss of essential services, even in the face of institutional collapse.
Analyzing the community’s response reveals a shift from dependency on a single institution to a decentralized model of care. For instance, volunteer-led health fairs now provide screenings and education, targeting underserved populations like seniors and low-income families. This approach not only addresses immediate health needs but also fosters a culture of self-reliance, proving that community-driven solutions can bridge gaps left by systemic failures.
To sustain this legacy, consider these actionable steps: first, establish a coalition of local leaders, healthcare providers, and residents to identify ongoing needs. Second, advocate for policy changes that incentivize investment in rural healthcare infrastructure. Finally, leverage digital tools to connect residents with telehealth services, ensuring continuity of care. By combining traditional community organizing with modern innovation, Cumberland can transform loss into a foundation for long-term resilience.
Comparatively, the response in Cumberland stands out when contrasted with communities that faced similar closures but lacked coordinated action. While some towns saw health outcomes deteriorate, Cumberland’s proactive stance has maintained stability. This underscores the importance of swift, unified community engagement in crises, offering a blueprint for other rural areas grappling with healthcare desertification.
Descriptively, the legacy of Sacred Heart Hospital lives on in the stories of those it once served and the spaces it now inspires. The former hospital’s walls, once symbols of healing, now echo with the voices of community meetings and wellness programs. This transformation from a place of treatment to a hub of prevention exemplifies how physical spaces can evolve to meet changing needs, embodying the enduring spirit of a community determined to thrive.
Mastering The Last of Us: Strategies to Conquer the Hospital Level
You may want to see also
Frequently asked questions
Sacred Heart Hospital in Cumberland, MD, closed in 2009 due to financial difficulties and declining patient volumes.
The hospital closed primarily because of financial struggles, including operating losses and the inability to sustain its services in a changing healthcare landscape.
After its closure, the facility was repurposed, and some of its services were absorbed by other healthcare providers in the region, including Western Maryland Health System.
Yes, there were efforts to save the hospital, including community support and discussions about potential partnerships, but these attempts were ultimately unsuccessful.
The building has been repurposed for other uses, though specific details may vary depending on the most recent developments in the area.