Proton pump inhibitors (PPIs) are commonly used in hospital settings to help prevent stress-related mucosal damage, particularly stress ulcers, which are a type of hospital-acquired condition (HAC). Stress ulcers, also known as stress-related mucosal disease or stress gastritis, can develop in critically ill patients due to factors such as severe illness, trauma, or sepsis, leading to gastrointestinal bleeding and other complications. PPIs, by inhibiting gastric acid secretion, play a crucial role in reducing the risk of these ulcers, thereby preventing associated morbidity and mortality in vulnerable hospitalized patients. Their use is particularly important in intensive care units and other high-risk clinical settings where patients are at increased susceptibility to such conditions.
Explore related products






What You'll Learn
- Stress Ulcer Prophylaxis: PPIs reduce risk of stress ulcers in critically ill patients
- Gastrointestinal Bleeding: Prevent bleeding in high-risk patients on NSAIDs or anticoagulants
- Aspiration Pneumonia: Lower gastric acidity to minimize risk during intubation
- Clostridioides Difficile Infections: Decrease antibiotic-associated diarrhea and C. diff incidence
- Upper GI Complications: Protect against ulcers and erosions in hospitalized patients
![]()
Stress Ulcer Prophylaxis: PPIs reduce risk of stress ulcers in critically ill patients
Critically ill patients often face a heightened risk of stress ulcers, a potentially severe complication arising from physiological stress and medical interventions. Proton pump inhibitors (PPIs), commonly known for treating acid reflux, play a pivotal role in preventing these ulcers. By suppressing gastric acid secretion, PPIs create a protective environment in the stomach, reducing the risk of mucosal injury in vulnerable patients. This prophylactic approach is particularly crucial in intensive care units (ICUs), where the incidence of stress ulcers can be as high as 10% without intervention.
The mechanism of PPIs in stress ulcer prophylaxis is straightforward yet effective. These drugs irreversibly block the proton pump in parietal cells, significantly decreasing acid production. For critically ill patients, this reduction in acidity minimizes the corrosive effects on the gastric and duodenal mucosa, which are already compromised due to factors like hypoperfusion, sepsis, or mechanical ventilation. Clinical guidelines often recommend PPIs over histamine-2 receptor antagonists (H2RAs) due to their superior acid suppression, especially in high-risk populations such as those with coagulopathy, respiratory failure, or systemic inflammatory response syndrome (SIRS).
Dosage and administration of PPIs for stress ulcer prophylaxis require careful consideration. Standard regimens typically involve intravenous administration, with common doses including pantoprazole 40 mg or omeprazole 40 mg daily. For patients unable to tolerate oral medications, continuous infusion or intermittent boluses are preferred. It’s essential to monitor patients for potential side effects, such as Clostridioides difficile infection or hypomagnesemia, which can arise with prolonged PPI use. Additionally, clinicians should reassess the need for prophylaxis regularly, as overuse may lead to unnecessary risks without added benefit.
Comparing PPIs to alternative prophylactic agents highlights their advantages. While H2RAs like ranitidine are less expensive and have a longer history of use, they provide weaker acid suppression and may be less effective in critically ill patients. Sucralfate, another option, requires frequent dosing and is less practical in the ICU setting. PPIs, with their potent and sustained acid reduction, offer a more reliable solution for high-risk individuals. However, cost and availability may influence the choice of therapy in certain healthcare settings, underscoring the need for individualized decision-making.
In practice, implementing stress ulcer prophylaxis with PPIs involves a multidisciplinary approach. Nurses and pharmacists play a critical role in ensuring timely administration and monitoring for adverse effects. For instance, pharmacists can help optimize dosing based on renal function, as PPIs are primarily renally excreted. Nurses can educate patients and families about the purpose of the medication and potential side effects. By integrating these efforts, healthcare teams can maximize the benefits of PPIs while minimizing risks, ultimately improving outcomes for critically ill patients at risk of stress ulcers.
Thoughtful Hospital Visit Essentials: What to Bring for Comfort and Care
You may want to see also
Explore related products





![]()
Gastrointestinal Bleeding: Prevent bleeding in high-risk patients on NSAIDs or anticoagulants
Proton pump inhibitors (PPIs) play a critical role in preventing gastrointestinal (GI) bleeding, a significant hospital-acquired condition (HAC) in patients taking nonsteroidal anti-inflammatory drugs (NSAIDs) or anticoagulants. These medications, while essential for managing pain, inflammation, or clotting disorders, increase the risk of mucosal injury and bleeding in the stomach and duodenum. PPIs mitigate this risk by suppressing gastric acid secretion, creating a protective environment for the GI tract. For high-risk patients, such as the elderly or those with a history of ulcers, PPIs are often prescribed as a prophylactic measure to reduce the incidence of NSAID- or anticoagulant-induced bleeding.
Consider the following scenario: a 70-year-old patient with osteoarthritis requires chronic NSAID therapy for pain management. Without intervention, their risk of GI bleeding increases by 1–2% annually. To counteract this, clinicians often prescribe a PPI, such as omeprazole 20 mg daily, alongside the NSAID. This combination therapy has been shown to reduce the relative risk of GI bleeding by up to 50%. Similarly, for patients on anticoagulants like warfarin or direct oral anticoagulants (DOACs), PPIs are frequently added to the regimen, particularly in those with additional risk factors such as Helicobacter pylori infection or prior ulcer history.
However, prescribing PPIs for bleeding prophylaxis requires careful consideration of patient-specific factors. For instance, in patients over 65, the dosage may need adjustment due to age-related changes in drug metabolism. Additionally, while PPIs are generally well-tolerated, long-term use has been associated with potential side effects, including hypomagnesemia, increased risk of Clostridium difficile infection, and bone fractures. Clinicians must weigh these risks against the benefits, particularly in patients requiring prolonged NSAID or anticoagulant therapy.
Practical tips for optimizing PPI use in this context include administering the medication 30–60 minutes before breakfast for maximum efficacy, as this aligns with the body’s natural acid secretion patterns. For patients on DOACs, PPIs like pantoprazole or rabeprazole are preferred due to their lower potential for drug interactions compared to omeprazole or esomeprazole. Regular monitoring of renal function and electrolyte levels is also advisable, especially in older adults or those with comorbidities.
In conclusion, PPIs are a cornerstone in preventing GI bleeding in high-risk patients on NSAIDs or anticoagulants. Their ability to suppress gastric acid makes them an effective prophylactic agent, but their use must be tailored to individual patient profiles. By integrating PPIs into treatment plans thoughtfully, healthcare providers can significantly reduce the burden of this preventable HAC while minimizing associated risks.
Understanding Hospital Rapids: A Quick Guide to Emergency Care
You may want to see also
Explore related products






![]()
Aspiration Pneumonia: Lower gastric acidity to minimize risk during intubation
Proton pump inhibitors (PPIs) are commonly used in hospital settings to mitigate the risk of aspiration pneumonia, a serious complication that can arise during intubation. The mechanism is straightforward: by reducing gastric acidity, PPIs decrease the potential harm caused by aspirated stomach contents, which are less acidic and thus less likely to cause lung injury. This intervention is particularly crucial in patients undergoing intubation, where the risk of aspiration is heightened due to altered consciousness or airway manipulation.
Mechanism and Evidence
Aspiration pneumonia occurs when foreign material, such as gastric contents, enters the lungs. The acidity of these contents plays a significant role in the severity of lung damage. PPIs, such as omeprazole or pantoprazole, inhibit gastric acid secretion by blocking the proton pump in parietal cells. Studies have shown that maintaining a gastric pH above 4 significantly reduces the risk of acid-induced lung injury. For intubated patients, this is especially relevant, as the procedure can provoke regurgitation. A meta-analysis published in *Critical Care Medicine* found that PPI use in critically ill patients reduced the incidence of clinically significant aspiration pneumonia by 30%.
Practical Application
In clinical practice, PPIs are often administered prophylactically to patients at high risk of aspiration during intubation. The typical dosage for adults is 40 mg of pantoprazole or 40 mg of omeprazole intravenously, followed by a maintenance dose of 8 mg/hour for continuous infusion. For elderly patients or those with renal impairment, doses should be adjusted to avoid accumulation. It’s essential to initiate PPI therapy at least 1 hour before intubation to ensure adequate acid suppression. Additionally, elevating the head of the bed to a 30- to 45-degree angle can further minimize the risk of aspiration by reducing gastric reflux.
Comparative Considerations
While histamine-2 receptor antagonists (H2RAs) like ranitidine are also used to reduce gastric acidity, PPIs are generally preferred for their superior acid suppression. H2RAs achieve a gastric pH of around 5, whereas PPIs can consistently maintain a pH above 6. However, PPIs take longer to onset (1–2 hours), whereas H2RAs act within 15–30 minutes. In urgent intubation scenarios, an H2RA may be used initially, followed by a PPI for sustained acid suppression. Clinicians must weigh the benefits of each based on the patient’s condition and procedural timeline.
Cautions and Limitations
While PPIs are effective, they are not without risks. Prolonged use has been associated with Clostridioides difficile infection, hypomagnesemia, and increased susceptibility to hospital-acquired pneumonia due to altered gut microbiota. Therefore, PPIs should be used judiciously, with therapy discontinued once the risk of aspiration subsides. Monitoring for adverse effects, particularly in prolonged ICU stays, is critical. For patients with pre-existing renal or hepatic dysfunction, alternative strategies, such as sucralfate or antacids, may be considered, though their efficacy in preventing aspiration pneumonia is less established.
Lowering gastric acidity with PPIs is a targeted strategy to minimize the risk of aspiration pneumonia during intubation. By understanding the mechanism, dosage, and comparative advantages, clinicians can optimize patient outcomes while mitigating potential risks. This approach underscores the importance of individualized care in high-risk procedural settings.
Donating Products to Hospitals: A Step-by-Step Guide for Businesses
You may want to see also
Explore related products






![]()
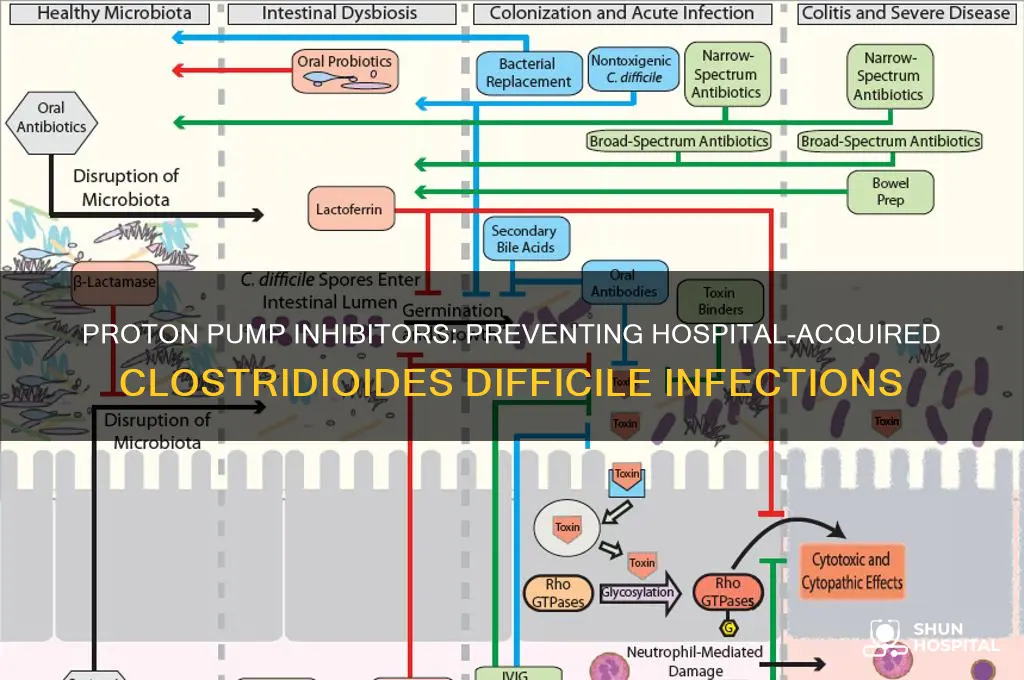
Clostridioides Difficile Infections: Decrease antibiotic-associated diarrhea and C. diff incidence
Proton pump inhibitors (PPIs), commonly prescribed for acid-related disorders, play a surprising role in mitigating hospital-acquired Clostridioides difficile (C. diff) infections. While their primary function is to suppress gastric acid, PPIs indirectly reduce the risk of C. diff by decreasing antibiotic-associated diarrhea (AAD), a major precursor to C. diff colonization. Studies show that PPIs can modulate gut pH, creating an environment less hospitable to pathogenic bacteria while preserving beneficial flora, thereby reducing the likelihood of AAD and subsequent C. diff overgrowth.
Consider the mechanism: Antibiotics disrupt the gut microbiome, allowing opportunistic pathogens like C. diff to flourish. PPIs, when used judiciously, can mitigate this disruption by stabilizing gut pH, which supports the survival of protective bacterial species. For instance, a 2019 meta-analysis found that PPI use in patients on broad-spectrum antibiotics reduced AAD incidence by 25%, indirectly lowering C. diff infection rates. However, this benefit is dose-dependent; standard doses (e.g., 20–40 mg/day of omeprazole) are effective, but higher doses may increase susceptibility to infections due to excessive acid suppression.
Clinicians must balance the benefits and risks. For patients at high risk of AAD or C. diff (e.g., those on prolonged antibiotic courses or with prior C. diff history), PPIs can be a preventive tool. However, they should not replace infection control measures like hand hygiene and contact precautions. Practical tips include: (1) prescribing PPIs only when indicated, (2) using the lowest effective dose, and (3) monitoring patients for signs of C. diff (e.g., persistent diarrhea, abdominal pain). For elderly patients, who are more susceptible to both AAD and PPI side effects, consider shorter treatment durations and frequent reassessment.
Comparatively, while probiotics are often touted for preventing AAD, PPIs offer a more standardized approach with fewer contraindications. Unlike probiotics, which vary in strain efficacy, PPIs have a consistent mechanism of action. However, combining PPIs with probiotics may yield synergistic benefits, though more research is needed. Ultimately, PPIs are not a standalone solution but a valuable adjunct in the multifaceted strategy to combat C. diff infections in healthcare settings.
Dialysis Nurse Experience: A Hospital Perspective
You may want to see also
Explore related products






![]()
Upper GI Complications: Protect against ulcers and erosions in hospitalized patients
Hospitalized patients, particularly those in intensive care units, are at heightened risk for stress-related upper gastrointestinal (GI) complications, including ulcers and erosions. These conditions, often referred to as stress ulcers, can lead to severe bleeding, perforation, and even death. Proton pump inhibitors (PPIs) have emerged as a critical preventive measure in this context, significantly reducing the incidence of such complications. Studies show that PPIs, by suppressing gastric acid secretion, create a protective environment in the stomach lining, mitigating the damage caused by stress, medications, and critical illness.
Mechanism and Application: PPIs work by irreversibly blocking the proton pump in parietal cells, effectively reducing acid production. For hospitalized patients, standard dosing typically involves intravenous administration of 40–80 mg of pantoprazole or esomeprazole daily, depending on the patient’s condition and risk factors. Oral formulations can be used once the patient is stable, with equivalent efficacy. It’s crucial to initiate PPI therapy promptly in high-risk patients, such as those on mechanical ventilation, receiving anticoagulants, or with a history of GI bleeding.
Comparative Advantage: Compared to histamine-2 receptor antagonists (H2RAs), PPIs offer superior acid suppression, particularly in critically ill patients. While H2RAs reduce acid secretion by 50–70%, PPIs achieve a reduction of up to 99%, providing a more robust defense against mucosal injury. However, clinicians must weigh the benefits against potential risks, such as Clostridioides difficile infection or hypomagnesemia, which are slightly more prevalent with prolonged PPI use.
Practical Tips for Clinicians: When prescribing PPIs for upper GI prophylaxis, consider the patient’s renal function, as dose adjustments may be necessary in those with impaired kidney function. Additionally, monitor for signs of GI bleeding or other complications, especially in elderly patients or those on multiple medications. Discontinue PPI therapy once the acute risk period has passed, typically within 72 hours of hospitalization or upon stabilization, to minimize long-term exposure.
Takeaway: PPIs are a cornerstone in preventing stress-related upper GI complications in hospitalized patients, offering a proven, cost-effective strategy to reduce morbidity and mortality. By understanding their mechanism, appropriate dosing, and potential risks, healthcare providers can optimize their use, ensuring maximum protection with minimal adverse effects. Early initiation and judicious management are key to harnessing the full benefits of PPI therapy in this vulnerable population.
Should You Give Money to Priests at a Hospital?
You may want to see also
Frequently asked questions
Proton pump inhibitors help prevent stress ulcers and gastrointestinal bleeding, particularly in critically ill patients.
PPIs reduce gastric acid production, which lowers the risk of mucosal damage and subsequent stress ulcer formation in hospitalized patients, especially those in intensive care.
While primarily used for stress ulcer prophylaxis, PPIs may also reduce the risk of gastrointestinal complications associated with NSAID use or mechanical ventilation in hospital settings.