In a hospital setting, a transfer unit serves as a specialized area or team dedicated to facilitating the safe and efficient movement of patients between different departments, facilities, or levels of care. This unit plays a critical role in ensuring seamless transitions, whether patients are being moved from the emergency department to an inpatient ward, transferred to an intensive care unit, or discharged to a rehabilitation center. The transfer unit coordinates logistics, verifies medical documentation, and ensures continuity of care by communicating vital patient information to the receiving team. Staffed by trained professionals, including nurses, physicians, and administrative personnel, the unit prioritizes patient safety, minimizes delays, and addresses any complications that may arise during the transfer process. By streamlining these transitions, the transfer unit enhances overall hospital efficiency and improves patient outcomes.
| Characteristics | Values |
|---|---|
| Definition | A specialized unit within a hospital designed to facilitate the safe and efficient transfer of patients between different departments, facilities, or levels of care. |
| Purpose | To streamline patient flow, optimize bed utilization, and ensure continuity of care during transitions. |
| Key Functions | - Coordinating patient transfers between wards, intensive care units (ICUs), emergency departments, and other hospital areas. - Managing bed allocation and discharge planning. - Ensuring smooth communication between healthcare teams during transfers. - Providing short-term observation and stabilization for patients awaiting admission or transfer. |
| Staffing | Typically includes nurses, physicians, and administrative staff trained in transfer protocols and patient assessment. |
| Equipment | Equipped with monitoring devices, basic medical supplies, and communication tools to support patient care during transitions. |
| Location | Often centrally located within the hospital for easy access to various departments. |
| Patient Population | Serves patients requiring transfer due to changes in clinical status, need for specialized care, or bed availability. |
| Benefits | - Reduces delays in patient care. - Improves bed management and hospital efficiency. - Enhances communication and coordination among healthcare providers. - Minimizes risks associated with patient transfers. |
| Challenges | - Requires robust coordination and communication systems. - May face resource constraints during high-volume periods. - Balancing patient needs with operational demands can be complex. |
| Recent Trends | Increased use of digital tools and electronic health records (EHRs) to streamline transfer processes and improve documentation. |
Explore related products






What You'll Learn
- Patient Transfer Process: Steps involved in moving patients safely between hospital departments or facilities
- Transfer Unit Equipment: Essential tools and devices used during patient transfers in hospitals
- Staff Roles in Transfers: Responsibilities of nurses, doctors, and technicians during patient transfers
- Safety Protocols: Guidelines to ensure patient safety and prevent injuries during hospital transfers
- Transfer Documentation: Importance of recording patient transfer details for continuity of care
![]()
Patient Transfer Process: Steps involved in moving patients safely between hospital departments or facilities
In a hospital setting, the patient transfer process is a critical operation that requires precision, coordination, and adherence to safety protocols. Whether moving a patient from the emergency department to the intensive care unit (ICU) or transferring them to a specialized facility, each step must be executed with care to ensure patient stability and continuity of treatment. The process begins with a thorough assessment of the patient’s condition, including vital signs, medical history, and current treatments. This evaluation determines the level of support needed during the transfer, such as oxygen therapy, medication administration, or specialized equipment like ventilators. For instance, a patient on a vasopressor infusion (e.g., norepinephrine at 8–12 mcg/min) requires continuous monitoring to prevent hypotension or hypertension during transit.
Once the assessment is complete, the next step involves preparing the necessary equipment and personnel. This includes securing a transfer bed or stretcher, ensuring all monitoring devices are functional, and assembling a team trained in handling the patient’s specific needs. For high-risk transfers, such as those involving critically ill neonates or patients with spinal injuries, specialized teams like neonatal transport units or spinal immobilization protocols are essential. Communication is key during this phase; the sending and receiving teams must align on the patient’s condition, ongoing treatments, and potential risks. For example, a patient on anticoagulants (e.g., heparin drip at 18 units/kg/hr) requires clear documentation to prevent bleeding complications during the transfer.
The actual transfer is a carefully choreographed sequence of actions. The patient is moved using techniques that minimize disruption to their condition, such as log-rolling for spinal precautions or maintaining head elevation for patients with intracranial hypertension. Medications and intravenous lines are secured to prevent dislodgment, and continuous monitoring is maintained throughout the journey. In inter-facility transfers, ambulances or medical transport vehicles equipped with advanced life support systems are used. For long-distance transfers, air medical services may be employed, requiring additional precautions like pressure regulation in aircraft cabins to avoid complications in patients with respiratory distress.
Post-transfer, the receiving team conducts a handover to ensure seamless continuity of care. This includes verifying the patient’s condition, reviewing medications, and confirming that all necessary documentation has been transferred. Any deviations from the patient’s baseline or incidents during the transfer are documented and addressed immediately. For example, a patient who experienced transient hypoxia during transit may require additional oxygen support or further diagnostic tests upon arrival. This phase underscores the importance of teamwork and clear communication in maintaining patient safety across transitions of care.
While the patient transfer process is standardized, it is not without challenges. Common risks include equipment failure, medication errors, and delays that can exacerbate the patient’s condition. To mitigate these, hospitals implement protocols such as pre-transfer checklists, regular equipment maintenance, and staff training in emergency response. For instance, a checklist might include verifying battery life on portable monitors or ensuring backup oxygen supplies are available. Ultimately, the goal of the patient transfer process is not just to move a patient from one location to another but to do so in a manner that prioritizes their safety, comfort, and ongoing medical needs. By adhering to these steps and remaining vigilant, healthcare teams can ensure that transfers are executed smoothly, even in high-pressure situations.
Cell Phone Signals: A Hospital Equipment Interference Risk
You may want to see also
Explore related products






![]()
Transfer Unit Equipment: Essential tools and devices used during patient transfers in hospitals
Patient transfers in hospitals are critical moments that require precision, safety, and efficiency. The equipment used in these transfers is not just ancillary—it’s foundational to ensuring patient well-being and staff effectiveness. From mobility aids to monitoring devices, each tool serves a specific purpose, often tailored to the patient’s condition, age, and mobility level. For instance, a bariatric patient may require a reinforced stretcher with a weight capacity of 700 lbs or more, while a pediatric transfer might involve smaller, adjustable slings designed for children under 50 lbs. Understanding these tools is essential for anyone involved in patient care.
Consider the transfer board, a deceptively simple device that bridges gaps between surfaces, such as a bed and a wheelchair. Its use requires technique: align the board parallel to the patient’s spine, ensure staff members are positioned on both sides to distribute weight evenly, and avoid abrupt movements that could cause discomfort or injury. Similarly, slide sheets—low-friction fabrics used to reposition patients—are invaluable for reducing manual handling risks. For example, a study in *The Lancet* found that slide sheet use decreased musculoskeletal injuries in healthcare workers by 30%. These tools are not just about moving patients; they’re about preserving dignity and safety.
Monitoring equipment plays a silent but vital role during transfers, particularly for patients with unstable conditions. Portable pulse oximeters, lightweight and battery-operated, provide real-time oxygen saturation levels, critical for patients with respiratory issues. For those on continuous oxygen therapy, a portable oxygen concentrator with a flow rate of 1–5 L/min ensures uninterrupted supply during transit. Defibrillators, though less commonly used, are essential in emergency transfers, with models like the Zoll X Series offering CPR feedback and real-time coaching for responders. These devices transform transfers from passive movements to active, monitored care episodes.
The choice of mobility aids also varies based on patient needs. For short-distance transfers, a wheeled commode chair may suffice, offering both toileting and mobility support. In contrast, sit-to-stand lifts are ideal for patients with partial mobility, using hydraulic or electric mechanisms to assist in standing and transferring. When selecting a lift, consider the patient’s weight, height, and range of motion—a lift with a sling that doesn’t accommodate their size can lead to discomfort or injury. Manufacturers like Arjo and Invacare provide detailed guidelines, such as ensuring the sling’s leg straps are positioned at the widest part of the thigh for stability.
Finally, the role of communication devices cannot be overstated. During transfers, especially in large hospitals, coordination is key. Wireless intercom systems allow staff to communicate hands-free, ensuring everyone is aware of the patient’s status and the transfer’s progress. For patients with cognitive impairments or language barriers, visual aids like picture boards or translation apps can facilitate understanding. A well-equipped transfer unit isn’t just about physical tools—it’s about creating an environment where every stakeholder, from the patient to the nurse, is informed and supported.
In practice, the effectiveness of transfer unit equipment hinges on training and adaptability. Staff should undergo regular drills on equipment use, such as practicing transfers with mannequins of varying weights to simulate real-world scenarios. Hospitals should also conduct equipment audits quarterly, checking for wear and tear, battery life, and compliance with safety standards. By prioritizing both the tools and the training, hospitals can turn patient transfers from potential risks into seamless, safe transitions.
Presenting a Case: A Guide for Hospital Success
You may want to see also
Explore related products






![]()
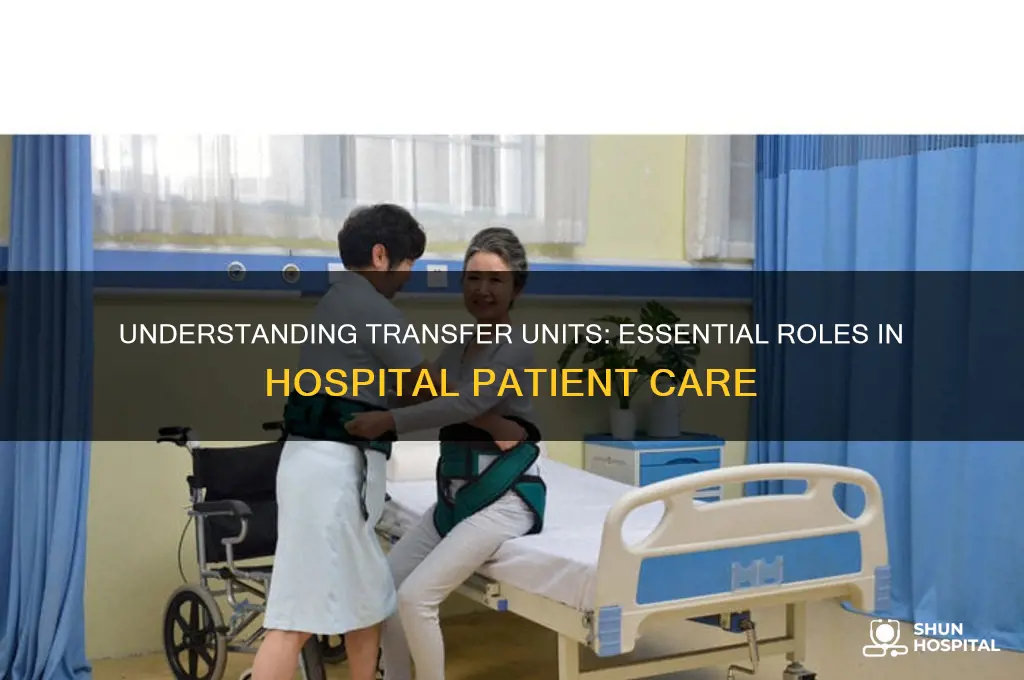
Staff Roles in Transfers: Responsibilities of nurses, doctors, and technicians during patient transfers
In a hospital transfer unit, seamless coordination among staff is critical to ensuring patient safety and continuity of care. Nurses, doctors, and technicians each play distinct roles, and their responsibilities are both interconnected and specialized. Nurses, for instance, serve as the primary point of contact during transfers, conducting thorough assessments to identify potential risks—such as unstable vital signs or medication discrepancies—before the patient leaves the current unit. They are responsible for preparing the patient physically, ensuring all necessary equipment (e.g., IV pumps, oxygen tanks) is functional, and documenting baseline data like pain levels or neurological status. A missed detail here, such as an undocumented allergy, can lead to complications during transit, underscoring the nurse’s role as the first line of defense against errors.
Doctors, on the other hand, provide the clinical oversight that guides the transfer process. They must review the patient’s medical history, current condition, and treatment plan to determine if the transfer is medically appropriate. For example, a patient on a high-dose vasopressor (e.g., norepinephrine at 8 mcg/min) may require stabilization before moving to another unit, as transport stress could exacerbate hemodynamic instability. The physician is also responsible for communicating with the receiving team, ensuring they are aware of critical details like recent surgeries, pending lab results, or changes in medication dosages. Without this step, the receiving team might inadvertently administer a contraindicated medication, such as an NSAID to a patient with acute kidney injury.
Technicians, often overlooked in transfer discussions, are indispensable for managing the logistical and technical aspects of patient movement. Respiratory therapists, for instance, must ensure ventilator settings are optimized for transport, particularly for patients on modes like pressure control (e.g., 20 cmH₂O inspiratory pressure, 6 mL/kg tidal volume). Biomedical technicians verify that monitoring devices, such as ECG leads or pulse oximeters, are calibrated and functioning, as signal loss during transit could delay critical interventions. Phlebotomists may need to draw time-sensitive labs (e.g., PT/INR for anticoagulated patients) immediately before transfer to provide the receiving team with up-to-date data. Each technician’s role is highly specific, yet their collective efforts prevent equipment failures or data gaps that could compromise care.
A comparative analysis of these roles reveals a hierarchy of responsibilities: nurses focus on patient-centered care, doctors on clinical decision-making, and technicians on technical execution. However, effective transfers require more than individual competence—they demand teamwork. For example, during the transfer of a pediatric patient (age 5–12) with a central line, the nurse might secure the line while the technician ensures the infusion pump is battery-powered, and the doctor confirms the child’s sedation level is appropriate for transport. This collaborative approach minimizes risks and ensures continuity, particularly in high-stakes scenarios like inter-hospital transfers or moves to intensive care units.
Ultimately, the success of a patient transfer hinges on clear communication, role awareness, and proactive problem-solving across disciplines. Nurses must advocate for the patient’s immediate needs, doctors must provide strategic direction, and technicians must execute technical tasks flawlessly. Practical tips, such as using checklists for equipment verification or holding brief huddles before transport, can enhance coordination. By understanding and fulfilling their unique responsibilities, staff members collectively safeguard patient well-being during one of the most vulnerable moments in their hospital journey.
Massachusetts Steward Hospital Closures: Which Facilities Are Shutting Down?
You may want to see also
Explore related products






![]()
Safety Protocols: Guidelines to ensure patient safety and prevent injuries during hospital transfers
Hospital transfers are inherently risky, with studies showing that up to 30% of adverse events occur during patient handoffs between departments or facilities. Implementing robust safety protocols is critical to mitigating these risks and ensuring continuity of care. A well-structured transfer unit acts as a centralized hub, coordinating logistics, communication, and clinical oversight to minimize errors and injuries. This begins with a standardized assessment of the patient’s condition, mobility, and equipment needs, ensuring that the transfer team is fully prepared for potential complications. For instance, a patient on a high-dose vasopressor (e.g., norepinephrine >0.2 mcg/kg/min) requires continuous hemodynamic monitoring and a specialized transport team to prevent decompensation during transit.
Effective communication is the backbone of safe transfers. The SBAR (Situation, Background, Assessment, Recommendation) framework provides a clear structure for handoffs, reducing miscommunication by up to 50% in some studies. For example, a nurse transferring a post-operative pediatric patient (age 5) with a morphine PCA (0.02 mg/kg/dose) must communicate the child’s pain score, last dose time, and respiratory rate to the receiving team to prevent opioid-induced respiratory depression. Equally important is the use of checklists, which ensure critical steps—such as securing IV lines, verifying medication reconciliation, and confirming allergy status—are not overlooked.
Equipment failures account for 10–20% of transfer-related incidents, making pre-transfer checks non-negotiable. Portable monitors, oxygen tanks, and battery-operated devices must be tested for functionality and sufficiency. For instance, a ventilator battery should last at least 1.5 times the estimated transfer duration, and backup manual ventilation equipment must be readily available. Additionally, environmental hazards like narrow corridors or uneven surfaces require advance scouting to prevent falls or equipment damage. Staff should practice emergency drills, such as managing a dislodged endotracheal tube during transport, to ensure swift response to crises.
Finally, patient-centered protocols address unique vulnerabilities. For elderly patients (age ≥65), frailty assessments and fall risk mitigation strategies—such as using transfer boards or slings—are essential. Pediatric transfers demand age-appropriate restraints and sedation protocols, with careful titration of medications like midazolam (0.05–0.1 mg/kg) to avoid oversedation. Bariatric patients require specialized stretchers and lifting equipment to prevent skin tears or musculoskeletal injuries to staff. By tailoring protocols to these specific needs, hospitals can significantly reduce transfer-related injuries and enhance overall safety.
In conclusion, a transfer unit’s success hinges on its ability to integrate rigorous safety protocols into every step of the process. From pre-transfer assessments to post-transfer debriefs, each action must prioritize patient stability and risk prevention. Hospitals that adopt these guidelines not only protect patients but also foster a culture of accountability and continuous improvement in care delivery.
Marriott's Big Data Analytics: Revolutionizing Hospitality Industry Leadership
You may want to see also
Explore related products






![]()
Transfer Documentation: Importance of recording patient transfer details for continuity of care
In a hospital setting, patient transfers between units or facilities are commonplace, yet each transition introduces risks to continuity of care. Transfer documentation serves as the bridge that ensures critical information isn’t lost in transit. Without detailed records of the patient’s condition, treatment history, and pending interventions, receiving teams may face delays, misinterpretations, or errors that compromise outcomes. For instance, a patient transferred from the emergency department to the intensive care unit (ICU) requires precise documentation of vital signs, medications administered (e.g., 5 mg of morphine for pain), and any recent procedures (e.g., intubation). Incomplete or inaccurate records can lead to duplicated tests, inappropriate dosing, or overlooked allergies, turning a routine transfer into a critical incident.
Consider the step-by-step process of effective transfer documentation. First, the transferring team must complete a comprehensive handover form, including the patient’s diagnosis, current medications, and recent lab results. Second, verbal communication during the handover is essential but should always be supplemented with written documentation to avoid discrepancies. Third, the receiving team must verify the information, clarify ambiguities, and update the patient’s chart immediately. For pediatric patients, age-specific details such as weight-based medication dosages (e.g., 10 mg/kg of acetaminophen for fever) are critical. Omitting such details can result in underdosing or overdosing, particularly in vulnerable populations like neonates or elderly patients.
The persuasive case for meticulous transfer documentation lies in its role as a safeguard against medical errors. Studies show that up to 70% of sentinel events in hospitals stem from communication failures during patient handoffs. By standardizing documentation protocols, hospitals can reduce these risks significantly. For example, implementing electronic health records (EHRs) with mandatory transfer templates ensures that key fields—such as allergy lists, ongoing infusions (e.g., 200 mL/hr of normal saline), and pending test results—are consistently recorded. This not only enhances patient safety but also improves efficiency by minimizing the need for redundant assessments.
A comparative analysis of hospitals with robust transfer documentation systems versus those with fragmented processes reveals stark differences in patient outcomes. Facilities that prioritize structured handovers and real-time updates experience lower readmission rates, shorter lengths of stay, and higher patient satisfaction scores. For instance, a hospital that adopted a barcode-scanning system for medication reconciliation during transfers reduced medication errors by 40%. In contrast, hospitals relying on paper-based systems or informal verbal handoffs often struggle with inconsistencies, leading to avoidable complications.
In practice, transfer documentation is not just a bureaucratic task but a cornerstone of patient-centered care. Nurses, physicians, and allied health professionals must collaborate to ensure that every detail is captured and communicated. Practical tips include using checklists to verify completeness, involving patients or their families in the process where possible, and conducting regular audits to identify gaps in documentation practices. For example, a checklist might include verifying the patient’s identity, confirming the reason for transfer, and documenting the last dose of antibiotics (e.g., 1 g of ceftriaxone at 0800). By treating transfer documentation as a shared responsibility, healthcare teams can maintain continuity of care and uphold the highest standards of safety.
Illinois Newborn Drug Testing: What Hospitals Do?
You may want to see also
Frequently asked questions
A transfer unit in a hospital is a designated area or team responsible for coordinating the safe and efficient movement of patients between departments, floors, or facilities. It ensures proper documentation, communication, and continuity of care during transitions.
The transfer unit is typically managed by a multidisciplinary team, including nurses, physicians, and administrative staff, who work together to oversee patient transfers and ensure compliance with hospital protocols.
The primary purpose of a transfer unit is to streamline patient transitions, minimize delays, and maintain patient safety by ensuring all necessary information and resources are in place before, during, and after the transfer.
A transfer unit ensures patient safety by verifying patient identification, reviewing medical records, coordinating with receiving departments, and ensuring appropriate staffing and equipment are available during the transfer process.