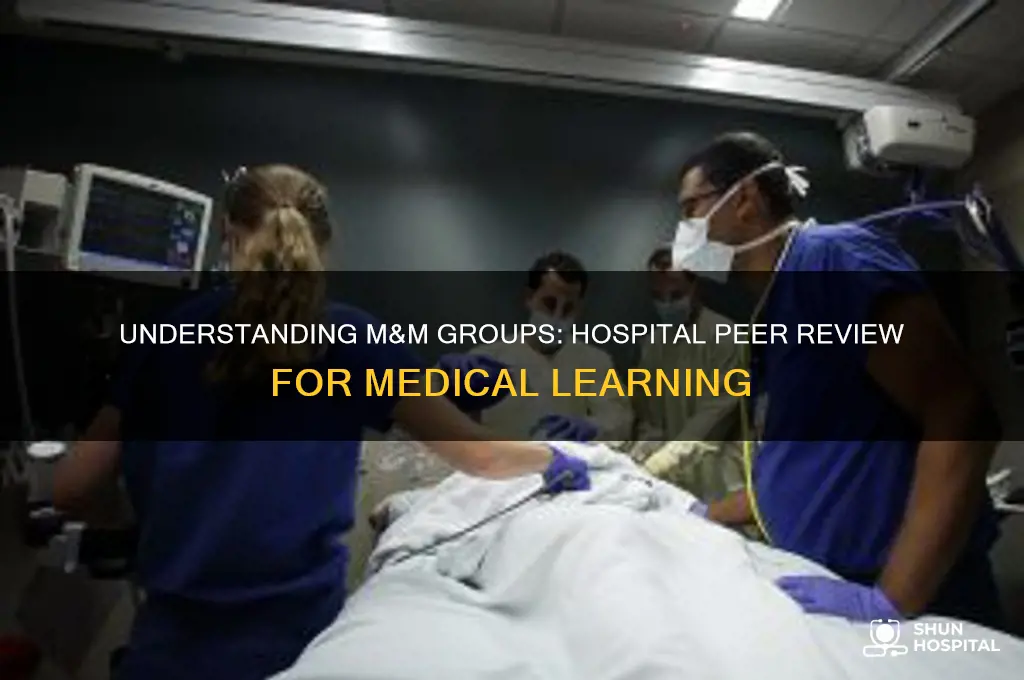
An M&M group, or Morbidity and Mortality Conference, is a structured meeting held in hospitals to review and discuss patient cases that involve complications, unexpected outcomes, or deaths. These sessions serve as a critical tool for continuous quality improvement, education, and fostering a culture of transparency among healthcare professionals. Typically led by physicians, the conferences aim to identify systemic issues, share best practices, and enhance patient care by analyzing what went well and what could be improved in specific cases. Participation is often multidisciplinary, involving nurses, residents, and other staff, ensuring a comprehensive perspective on patient safety and clinical decision-making.
| Characteristics | Values |
|---|---|
| Purpose | To review and discuss unexpected or adverse patient outcomes in a structured and confidential setting. |
| Full Name | Morbidity and Mortality (M&M) Conference |
| Participants | Physicians, nurses, residents, and other healthcare professionals involved in patient care. |
| Frequency | Typically held monthly or quarterly, depending on the institution. |
| Confidentiality | Protected under peer review laws to encourage open and honest discussion. |
| Focus | System failures, medical errors, complications, and preventable deaths. |
| Goals | Improve patient safety, identify trends, enhance clinical skills, and promote a culture of learning. |
| Structure | Case presentations, discussions, and actionable recommendations. |
| Documentation | Minutes and outcomes are recorded but not part of the patient's medical record. |
| Accreditation | Often required by accrediting bodies like The Joint Commission for hospitals. |
| Legal Protection | Discussions are generally not admissible in legal proceedings due to peer review protections. |
| Outcomes | Implementation of process improvements, policy changes, and educational initiatives. |
Explore related products






What You'll Learn
- M&M Conference Purpose: Discusses medical errors, complications, and ways to improve patient care and outcomes
- Participants in M&M: Includes physicians, nurses, residents, and other healthcare professionals involved in case reviews
- Case Presentation Format: Structured review of patient cases, focusing on errors, outcomes, and lessons learned
- Confidentiality in M&M: Protected discussions to encourage open dialogue without fear of legal repercussions
- Benefits of M&M: Enhances clinical skills, fosters teamwork, and reduces medical errors in hospitals
![]()
M&M Conference Purpose: Discusses medical errors, complications, and ways to improve patient care and outcomes
Medical errors are the third leading cause of death in the United States, accounting for an estimated 250,000 lives lost annually. This staggering statistic underscores the critical need for transparent, constructive discussions about mistakes and complications in healthcare settings. Enter the M&M (Morbidity and Mortality) Conference, a structured forum where medical professionals dissect adverse events to identify systemic failures, individual oversights, and opportunities for improvement. Unlike disciplinary hearings, these conferences foster a blame-free environment focused on learning and prevention, ensuring that each error translates into actionable insights rather than recurring tragedies.
Consider a hypothetical scenario: A 62-year-old diabetic patient admitted for a routine knee replacement develops septic shock post-surgery due to an undiagnosed wound infection. At an M&M Conference, the case would be presented anonymously, with participants analyzing the timeline of care—from pre-op assessments to post-op monitoring. Key questions might include: Was the infection missed during pre-surgical screening? Did the surgical team adhere to sterile protocols? How could earlier intervention have altered the outcome? By breaking down the event step-by-step, attendees identify gaps—such as inadequate wound assessment tools or communication breakdowns between shifts—and propose solutions like mandatory pre-op infection checklists or standardized handoff protocols.
The structure of an M&M Conference is deliberate, designed to maximize learning while minimizing defensiveness. Typically led by a moderator, the session follows a standardized format: case presentation, open discussion, root cause analysis, and actionable recommendations. For instance, after reviewing a case where a pediatric patient received a tenfold overdose of heparin due to a decimal error, the group might recommend implementing double-checking protocols for high-risk medications and integrating dose-range alerts in the electronic health record system. Such specificity ensures that discussions yield tangible changes, not just abstract lessons.
Critics often question whether discussing errors openly might increase liability risks or erode trust in healthcare providers. However, evidence suggests the opposite: hospitals with robust M&M programs consistently report lower malpractice claims and higher patient satisfaction scores. Transparency builds trust, both among staff and with the public. For example, a study published in *JAMA Surgery* found that hospitals that disclosed errors and offered compensation proactively saw a 28% reduction in lawsuits compared to those that did not. This comparative data highlights the persuasive argument for embracing, not avoiding, these difficult conversations.
Ultimately, the purpose of an M&M Conference extends beyond error analysis—it’s about cultivating a culture of continuous improvement. By treating complications as collective learning opportunities rather than individual failures, healthcare teams can systematically reduce risks. Practical tips for maximizing conference effectiveness include involving multidisciplinary participants (nurses, pharmacists, technicians), incorporating simulation exercises to test proposed solutions, and tracking implementation of recommendations over time. In this way, the M&M Conference becomes not just a meeting, but a cornerstone of safer, more responsive patient care.
Ashford Hospitality Trust: A Smart Investment Move?
You may want to see also
Explore related products






![]()
Participants in M&M: Includes physicians, nurses, residents, and other healthcare professionals involved in case reviews
Morbidity and Mortality (M&M) conferences are a cornerstone of medical education and quality improvement, bringing together a diverse group of healthcare professionals to review complex cases and identify areas for enhancement. At the heart of these conferences are the participants—physicians, nurses, residents, and other healthcare professionals—whose collective expertise drives meaningful discussions and actionable insights. Each participant brings a unique perspective, ensuring a comprehensive analysis of patient outcomes and systemic processes.
Consider the role of physicians, often the primary decision-makers in patient care. Their involvement in M&M conferences is critical, as they provide clinical context, explain treatment rationale, and highlight diagnostic challenges. For instance, a senior attending physician might dissect a case where a patient experienced an adverse drug reaction, detailing the thought process behind the prescribed medication and its dosage—say, 50 mg of a beta-blocker for a 65-year-old with hypertension. This level of specificity fosters a deeper understanding of the case and encourages evidence-based practice.
Nurses, on the other hand, offer a frontline perspective that is equally invaluable. Their insights into patient monitoring, symptom management, and communication gaps can reveal systemic issues that physicians might overlook. For example, a nurse might point out that a post-operative patient’s pain was inadequately managed due to delayed medication administration, prompting a discussion on improving workflow protocols. This collaborative approach ensures that M&M conferences address both clinical and operational aspects of care.
Residents and trainees play a dual role in these conferences: as learners and as contributors. Their participation sharpens their critical thinking skills and exposes them to real-world complexities. A resident might present a case they managed, such as a misdiagnosed appendicitis in a pediatric patient, and receive feedback from more experienced colleagues. This not only enhances their education but also fosters a culture of accountability and continuous learning.
Finally, the inclusion of other healthcare professionals—pharmacists, therapists, and social workers—broadens the scope of M&M conferences. A pharmacist, for instance, could highlight a medication error stemming from a misinterpreted prescription, while a physical therapist might discuss how delayed rehabilitation impacted a patient’s recovery. This multidisciplinary approach ensures that all facets of patient care are scrutinized, leading to more holistic solutions.
In practice, organizing an effective M&M conference requires careful consideration of participant roles. Facilitators should encourage active engagement, ensure all voices are heard, and guide discussions toward constructive outcomes. For example, using anonymized cases can reduce defensiveness, while structured frameworks like the "root cause analysis" method can keep the focus on systemic improvements rather than individual blame. By leveraging the diverse expertise of its participants, an M&M group can transform case reviews into opportunities for meaningful change, ultimately enhancing patient safety and care quality.
Kaiser Family Foundation Insights: Interpreter Services in U.S. Hospitals
You may want to see also
Explore related products

$13.99 $15.9





![]()
Case Presentation Format: Structured review of patient cases, focusing on errors, outcomes, and lessons learned
Morbidity and Mortality (M&M) conferences are a cornerstone of medical education and quality improvement in hospitals, providing a structured forum for reviewing patient cases to identify errors, analyze outcomes, and derive actionable lessons. The case presentation format is critical to this process, as it ensures a systematic and reflective approach to learning from both successes and failures. A well-structured case presentation begins with a concise summary of the patient’s demographics, chief complaint, and relevant medical history, setting the stage for a detailed timeline of events. This chronological framework highlights decision points, interventions, and deviations from expected outcomes, making it easier to pinpoint critical errors or oversights. For instance, a 62-year-old male with a history of diabetes presenting with chest pain might have a timeline that includes initial triage, diagnostic delays, and eventual complications, such as a missed myocardial infarction due to misinterpreted lab results.
The analytical phase of the presentation shifts focus to the errors identified, categorizing them into systems failures, cognitive biases, or technical mistakes. For example, a delay in administering a 325 mg aspirin for suspected acute coronary syndrome could stem from a miscommunication during shift change, while a failure to recognize hyperkalemia (potassium >5.5 mmol/L) might result from overreliance on automated lab alerts. This step requires a balance of objectivity and empathy, as it involves critiquing decisions without assigning blame. Tools like the SBAR (Situation, Background, Assessment, Recommendation) framework can help structure this analysis, ensuring clarity and completeness. The goal is not to assign fault but to understand the root causes of errors, whether they lie in individual actions, team dynamics, or institutional protocols.
The outcomes section of the presentation must go beyond clinical results to include both patient-centered and systemic impacts. For a 78-year-old female with a hip fracture who developed a pressure ulcer during hospitalization, the outcome might include prolonged recovery, increased healthcare costs, and diminished quality of life. This part of the presentation should also address whether the error was preventable and what immediate corrective actions were taken, such as initiating a wound care protocol or escalating to a higher level of nursing care. By quantifying outcomes—for example, a 20% increase in hospital stay duration or a $15,000 rise in treatment costs—the presentation underscores the tangible consequences of errors, reinforcing the urgency of learning from them.
The final and most critical component of the case presentation is the lessons learned, which should be specific, actionable, and tailored to the audience. For a case involving a medication error, such as administering 10 mg of warfarin instead of 5 mg to an elderly patient, recommendations might include double-checking high-risk medications, implementing barcode scanning systems, or providing refresher training on anticoagulant dosing for staff. These lessons should be framed as systemic improvements rather than individual corrections, such as revising the hospital’s medication reconciliation process for patients over 65. Practical tips, like creating a checklist for high-risk medications or designating a pharmacist to review complex regimens, can make these lessons immediately applicable.
In conclusion, a structured case presentation format transforms M&M conferences from mere case reviews into powerful tools for education and change. By meticulously dissecting errors, analyzing outcomes, and distilling actionable lessons, healthcare teams can foster a culture of continuous improvement. This approach not only enhances patient safety but also empowers clinicians to approach their practice with greater awareness and accountability. Whether addressing a diagnostic delay in a pediatric patient or a procedural complication in a surgical case, the format ensures that every case contributes to a safer, more effective healthcare system.
Hospital Bound: Packing Essentials for Your Newborn
You may want to see also
Explore related products

$29.97

$72.01 $79.74

$48.85


![]()
Confidentiality in M&M: Protected discussions to encourage open dialogue without fear of legal repercussions
Morbidity and Mortality (M&M) conferences are a cornerstone of medical education and quality improvement, providing a forum for healthcare professionals to discuss adverse patient outcomes and identify opportunities for learning and system enhancement. However, the success of these conferences hinges on the willingness of participants to engage in candid, open dialogue. This is where confidentiality becomes paramount. Without assurances that their words will not be used against them in legal proceedings, clinicians may hesitate to share critical insights, hindering the very purpose of M&M conferences.
To foster an environment of trust, many hospitals implement confidentiality protections for M&M discussions. These safeguards are often rooted in legal frameworks, such as the Peer Review Protection Act in the United States, which shields peer review proceedings from discovery in litigation. For instance, statements made during an M&M conference cannot be subpoenaed or used as evidence in malpractice lawsuits. This legal protection encourages participants to speak freely about errors, near misses, and systemic issues without fear of personal or professional repercussions.
Consider a scenario where a surgical team discusses a complication that arose during a complex procedure. Without confidentiality, team members might downplay their role or omit critical details to avoid liability. However, with protected discussions, they can openly analyze the sequence of events, identify contributing factors, and propose preventive measures. This transparency not only aids in individual learning but also strengthens institutional protocols, ultimately improving patient safety.
Practical implementation of confidentiality in M&M conferences requires clear guidelines. Hospitals should establish written policies outlining the scope of protection, permissible participants, and the consequences of breaches. For example, attendees might be required to sign confidentiality agreements, and discussions should be limited to authorized personnel. Additionally, facilitators must emphasize the purpose of the conference—learning, not blame—to reinforce a culture of openness.
In conclusion, confidentiality in M&M conferences is not merely a legal formality but a critical tool for fostering a culture of continuous improvement in healthcare. By protecting discussions from legal exposure, hospitals empower clinicians to engage in honest, constructive dialogue that drives systemic change. As healthcare systems evolve, maintaining robust confidentiality measures will remain essential to ensuring that M&M conferences fulfill their potential as catalysts for safer, more effective patient care.
Mayo Clinic: A Teaching Hospital?
You may want to see also
Explore related products





![]()
Benefits of M&M: Enhances clinical skills, fosters teamwork, and reduces medical errors in hospitals
Morbidity and Mortality (M&M) conferences are a cornerstone of medical education and quality improvement in hospitals. These structured meetings, where clinical cases with adverse outcomes are discussed, serve as a powerful tool for enhancing clinical skills, fostering teamwork, and reducing medical errors. By dissecting complex cases, healthcare professionals gain insights into diagnostic and therapeutic pitfalls, promoting a culture of continuous learning and patient safety.
Consider the analytical approach: during an M&M session, a case of a 62-year-old patient with a misdiagnosed myocardial infarction is presented. The discussion highlights how an over-reliance on initial negative troponin levels led to a delayed diagnosis. This deep dive into the case not only sharpens diagnostic acumen but also underscores the importance of integrating clinical judgment with laboratory results. For instance, clinicians learn to re-evaluate patients presenting with chest pain, even if initial tests appear normal, by considering factors like ECG changes or risk profiles. This targeted learning directly translates to improved patient care, reducing the likelihood of similar errors in the future.
From an instructive standpoint, M&M conferences provide a structured framework for skill enhancement. Participants are encouraged to ask probing questions, such as, "What alternative diagnostic pathways could have been pursued?" or "How could communication between teams have been improved?" These inquiries foster critical thinking and problem-solving skills. For example, a resident might learn to escalate concerns more effectively by using SBAR (Situation, Background, Assessment, Recommendation) communication techniques, ensuring that critical information is conveyed clearly and promptly. Such practical takeaways are immediately applicable to daily practice, enhancing both individual and team performance.
Persuasively, the collaborative nature of M&M conferences cannot be overstated. By bringing together physicians, nurses, pharmacists, and other healthcare providers, these sessions break down silos and promote interdisciplinary understanding. A case involving a medication error, for instance, might reveal gaps in the prescribing and dispensing process. Through open dialogue, teams identify systemic issues—such as unclear medication labels or inadequate handoff protocols—and collaboratively devise solutions. This teamwork not only strengthens relationships but also creates a safer, more efficient care environment.
Finally, the comparative perspective highlights the long-term benefits of M&M conferences in reducing medical errors. Studies show that hospitals with regular M&M sessions experience a 15-20% decrease in adverse events over time. For example, a hospital that implemented monthly M&M conferences saw a significant reduction in central line-associated bloodstream infections (CLABSIs) after identifying and addressing lapses in sterile technique during line placements. This data-driven approach reinforces the value of M&M conferences as a proactive strategy for error prevention, rather than a reactive response to incidents.
Incorporating M&M conferences into hospital culture requires commitment but yields substantial returns. By enhancing clinical skills, fostering teamwork, and reducing errors, these sessions are not just educational tools—they are essential mechanisms for improving patient outcomes and advancing the practice of medicine.
Unveiling the Iconic Hospital Name in the ER TV Series
You may want to see also
Frequently asked questions
M&M stands for Morbidity and Mortality, which refers to a regular conference or meeting where healthcare professionals discuss patient cases with adverse outcomes or complications to improve patient care and safety.
An M&M group typically includes physicians, nurses, residents, and other healthcare professionals involved in patient care. The group may also invite experts from specific fields to provide insights and recommendations.
The primary purpose of an M&M group is to identify systemic issues, improve clinical practices, and enhance patient outcomes by analyzing cases with morbidity or mortality. It fosters a culture of continuous learning and quality improvement within the healthcare team.































