A punctured lung, also known as a pneumothorax, is a serious condition that often requires hospitalization for proper treatment and monitoring. The normal hospital stay length for a punctured lung can vary significantly depending on the severity of the injury, the patient's overall health, and the treatment approach. In mild cases, where a small pneumothorax resolves on its own or with minimal intervention, patients may only need a short hospital stay of 1 to 2 days. However, more severe cases, especially those requiring procedures such as chest tube insertion or surgery, may necessitate a longer stay, typically ranging from 3 to 7 days. Factors such as complications, the need for additional treatments, or underlying health conditions can further extend the hospitalization period. Always consult with a healthcare provider for a personalized assessment and treatment plan.
| Characteristics | Values |
|---|---|
| Average Hospital Stay Length | 3 to 5 days (for stable cases without complications) |
| Factors Influencing Length of Stay | Severity of injury, presence of complications, need for chest tube |
| Mild to Moderate Cases | 2 to 4 days |
| Severe Cases (e.g., tension pneumothorax) | 5 to 7 days or longer, often requiring ICU care |
| Cases Requiring Surgery | 5 to 10 days or more, depending on the procedure and recovery |
| Complications (e.g., infection, bleeding) | Adds 2 to 5 days or more to the stay |
| Observation Period | 6 to 24 hours for minor cases to monitor stability |
| Outpatient Management | Rare, only for very small pneumothoraces without symptoms |
| Follow-Up Care | Outpatient follow-up within 1 to 2 weeks after discharge |
| Recovery Time Post-Discharge | 1 to 2 weeks for mild cases; up to 6 weeks for severe cases |
Explore related products






What You'll Learn
![]()
Factors Influencing Stay Length
The duration of a hospital stay for a punctured lung, or pneumothorax, varies widely, influenced by a complex interplay of medical and individual factors. Understanding these factors can help patients and caregivers set realistic expectations and prepare for recovery. Here’s a breakdown of what determines how long someone might stay hospitalized.
Severity and Type of Pneumothorax: The extent of lung collapse is a primary determinant. A small, spontaneous pneumothorax (less than 20% lung collapse) may require only observation and oxygen therapy, often resulting in a 1–3 day stay. In contrast, a tension pneumothorax, a life-threatening condition where air builds up in the pleural space, demands immediate chest tube insertion and intensive monitoring, potentially extending the stay to 5–7 days or more. Secondary pneumothorax, often linked to underlying conditions like COPD or cystic fibrosis, may require longer stays (up to 10 days) to manage complications and stabilize the patient.
Treatment Approach: The chosen treatment significantly impacts stay length. Conservative management, such as needle aspiration for small pneumothoraces, can lead to shorter stays (1–2 days) if successful. However, if a chest tube is inserted, the average stay increases to 3–5 days, depending on how quickly the lung re-expands. For recurrent pneumothoraces, surgical interventions like pleurodesis or video-assisted thoracoscopic surgery (VATS) are often necessary, adding 5–7 days to the hospital stay due to post-operative recovery.
Patient-Specific Factors: Age, overall health, and comorbidities play critical roles. Younger, otherwise healthy patients with no underlying lung disease typically recover faster, often discharged within 2–3 days. Older adults or those with conditions like diabetes, heart disease, or compromised immune systems may face prolonged stays (up to 7–10 days) due to slower healing and increased infection risk. Smoking status is another key factor; smokers often experience delayed recovery, as nicotine impairs lung tissue repair.
Complications and Response to Treatment: Unforeseen complications, such as infection, bleeding, or air leakage, can extend the stay. For instance, a persistent air leak may require the chest tube to remain in place for 5–7 days or longer. Additionally, patients who don’t respond well to initial treatment may need alternative interventions, such as switching from needle aspiration to chest tube placement, adding days to their stay.
Hospital Protocols and Resource Availability: Institutional policies and resource constraints also influence stay length. Some hospitals prioritize rapid turnover, discharging stable patients with outpatient follow-up, while others may keep patients longer for observation. Availability of diagnostic tools, such as CT scans or ultrasound, can expedite decision-making, potentially shortening stays. Conversely, staffing shortages or bed availability may inadvertently prolong hospitalization.
In summary, while a typical hospital stay for a punctured lung ranges from 1–7 days, the actual duration is highly individualized. Patients should discuss their specific circumstances with healthcare providers to understand their expected timeline and prepare for potential variations.
Unveiling the Count: C-Level Contacts in US Hospitals
You may want to see also
Explore related products




![]()
Typical Recovery Timeline
A punctured lung, or pneumothorax, often requires hospitalization, but the length of stay varies widely based on severity, treatment method, and individual health factors. For small, stable pneumothoraces, some patients may be discharged within 24 hours after observation and oxygen therapy. However, more severe cases, especially those requiring chest tube insertion or surgery, typically extend hospital stays to 3–5 days. Understanding the recovery timeline is crucial for managing expectations and planning post-discharge care.
Initial Hospital Phase (Days 1–3): During the first few days, the focus is on stabilizing the lung and monitoring for complications. If a chest tube is inserted, it remains in place until X-rays confirm the lung has fully re-expanded, which can take 2–4 days. Pain management is critical during this period, often involving medications like acetaminophen or ibuprofen, and occasionally opioids for severe discomfort. Patients are encouraged to breathe deeply and cough to prevent fluid buildup, though this must be balanced with pain tolerance.
Transition to Home Recovery (Days 4–14): Once discharged, recovery continues at home, with restrictions on strenuous activities, heavy lifting, and air travel for 4–6 weeks. Follow-up appointments are scheduled within 1–2 weeks to assess healing and remove any sutures. During this phase, gradual resumption of light activities is advised, but overexertion can delay healing or cause recurrence. Symptoms like mild chest pain or fatigue are common but should improve steadily.
Long-Term Healing (Weeks 4–12): Full recovery of lung function typically takes 6–12 weeks, depending on the extent of the injury. Patients with pre-existing conditions like COPD or asthma may experience a slower recovery. Regular exercise, such as walking or gentle stretching, aids in restoring lung capacity. Avoiding smoking is critical, as it impairs healing and increases the risk of recurrence. Persistent shortness of breath or chest pain warrants immediate medical attention.
Preventing Recurrence: Recurrent pneumothorax is a risk, especially in young, tall individuals or those with underlying lung diseases. Lifestyle modifications, such as quitting smoking and avoiding activities with rapid pressure changes (e.g., scuba diving), are essential. In some cases, surgical interventions like pleurodesis or bullectomy may be recommended to prevent future episodes. Understanding these stages empowers patients to actively participate in their recovery and reduce long-term risks.
Steps to Secure a Hospital Board Member Position Successfully
You may want to see also
Explore related products






![]()
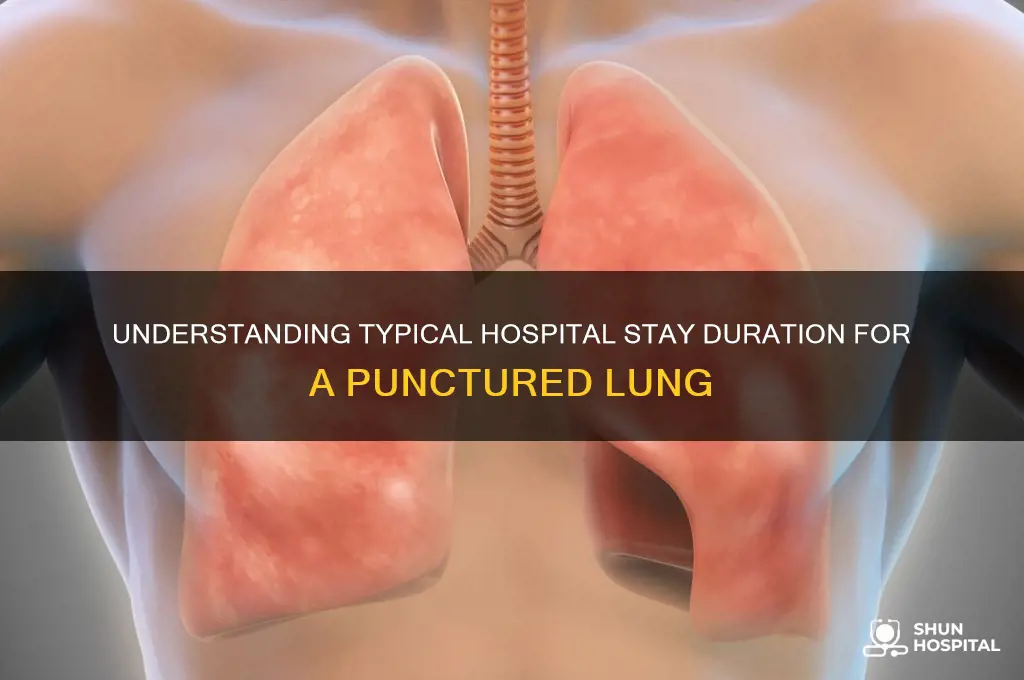
Severe Cases vs. Mild Cases
The severity of a punctured lung, medically known as a pneumothorax, dictates the length and intensity of hospital care. Mild cases, where the lung collapse is less than 20%, often resolve with minimal intervention. Patients may receive a simple chest tube to drain air and are typically monitored for 24 to 48 hours. If the lung re-expands without complications, discharge can occur within 1 to 3 days, followed by outpatient follow-ups to ensure healing.
Contrastingly, severe cases—defined by a lung collapse exceeding 50% or complications like tension pneumothorax—demand aggressive management. These patients often require larger chest tubes, prolonged suction, and continuous monitoring in an intensive care unit (ICU). Hospital stays extend to 5 to 7 days or longer, depending on response to treatment. In some instances, surgical intervention, such as video-assisted thoracoscopic surgery (VATS), becomes necessary to repair damaged tissue or prevent recurrence, further prolonging recovery time.
Age and comorbidities play a critical role in differentiating care between mild and severe cases. Younger, healthy individuals with mild pneumothorax often recover swiftly, while older adults or those with conditions like COPD may face extended stays due to slower healing and higher risk of complications. For example, a 25-year-old with a 15% lung collapse might be discharged within 2 days, whereas a 60-year-old with a 60% collapse and asthma could remain hospitalized for a week or more.
Practical tips for patients include adhering strictly to post-discharge instructions, such as avoiding air travel or strenuous activity for 6 to 8 weeks. Severe case patients should monitor for signs of recurrence, like sudden chest pain or shortness of breath, and seek immediate care if symptoms arise. Understanding the distinction between mild and severe cases empowers patients to anticipate recovery timelines and take proactive steps in their care.
In summary, while mild pneumothorax cases often resolve with short hospital stays and conservative management, severe cases require intensive treatment and longer recovery periods. Tailored care based on severity, age, and health status ensures optimal outcomes, highlighting the importance of individualized medical approaches in managing this condition.
Assemblies of God Group Hospitalization Plans: What You Need to Know
You may want to see also
Explore related products






![]()
Post-Surgery Hospital Duration
The duration of a hospital stay following surgery for a punctured lung, or pneumothorax, varies widely based on individual factors such as the severity of the injury, the patient’s overall health, and the type of treatment required. On average, patients with a simple pneumothorax treated with a chest tube can expect a hospital stay of 2 to 5 days. However, complications such as recurrent air leaks, infection, or the need for surgical intervention (e.g., thoracotomy or video-assisted thoracoscopic surgery, VATS) can extend this stay to 5 to 7 days or longer. Monitoring for stability in lung function and ensuring the chest tube is effectively draining air are critical determinants of discharge timing.
For patients undergoing VATS, a minimally invasive procedure often used for recurrent or complex pneumothorax, the hospital stay is typically 3 to 5 days. This shorter duration is due to smaller incisions, reduced postoperative pain, and quicker recovery times compared to open surgery. However, older adults or those with comorbidities like chronic obstructive pulmonary disease (COPD) may require additional days for close observation and management of respiratory complications. Pain control, often managed with opioids or non-steroidal anti-inflammatory drugs (NSAIDs), is also a factor, as inadequate pain management can delay mobility and recovery.
Instructively, patients and caregivers should prepare for a hospital stay by understanding key milestones that indicate readiness for discharge. These include stable vital signs, minimal to no air leak from the chest tube, ability to breathe comfortably without supplemental oxygen, and tolerance of oral pain medication. Before leaving the hospital, patients should receive clear instructions on wound care, activity restrictions (e.g., avoiding heavy lifting for 4 to 6 weeks), and signs of complications to monitor, such as shortness of breath, chest pain, or fever. Follow-up appointments with a pulmonologist or surgeon are typically scheduled within 1 to 2 weeks to assess healing and remove sutures or staples if necessary.
Comparatively, hospital stays for pneumothorax differ significantly from those for other thoracic conditions. For instance, a lobectomy for lung cancer may require 5 to 7 days, while a pleural effusion treated with drainage might only necessitate 1 to 2 days. Pneumothorax falls in the middle, with its duration influenced by the need for procedural intervention and the patient’s response to treatment. Hospitals often use standardized protocols to streamline care, but individualized assessment remains essential, particularly for high-risk patients.
Persuasively, reducing hospital stay duration without compromising care is a priority for both patients and healthcare systems. Early mobilization, effective pain management, and proactive monitoring of complications are evidence-based strategies to achieve this. For example, encouraging patients to walk within 24 hours of chest tube insertion (when stable) can improve lung expansion and reduce the risk of pneumonia. Additionally, hospitals adopting enhanced recovery protocols, which include optimized fluid management and early nutrition, have reported shorter stays and higher patient satisfaction. By focusing on these practices, healthcare providers can ensure safe and efficient recovery for pneumothorax patients.
Hospital Liens: Can They Attach to Your Home?
You may want to see also
Explore related products






![]()
Discharge Criteria for Patients
The length of hospital stay for a punctured lung, or pneumothorax, varies widely depending on the severity of the injury, the patient's overall health, and the treatment required. While some patients may be discharged within 24 to 48 hours, others might require a stay of several days or even weeks. Discharge criteria are carefully evaluated to ensure the patient’s safety and recovery, balancing medical necessity with the benefits of home-based care.
Stability of Vital Signs is the cornerstone of discharge readiness. Patients must demonstrate consistent respiratory stability, with normal oxygen saturation levels (typically above 92% on room air) and a stable heart rate. For instance, a patient with a small, spontaneous pneumothorax who shows no signs of respiratory distress and maintains oxygen saturation above 94% may be considered for early discharge. In contrast, those requiring supplemental oxygen or showing signs of tension pneumothorax will likely need prolonged monitoring.
Resolution of Symptoms plays a critical role in determining discharge eligibility. Patients should report minimal to no chest pain, shortness of breath, or discomfort during deep breaths. A follow-up chest X-ray or CT scan is often performed to confirm re-expansion of the lung and absence of recurrent pneumothorax. For example, a repeat X-ray 6–12 hours after chest tube removal is standard to ensure the lung remains fully expanded before discharge.
Patient Education and Follow-Up Planning are essential components of safe discharge. Patients must understand activity restrictions, such as avoiding heavy lifting or strenuous exercise for 4–6 weeks, and recognize warning signs of recurrence (e.g., sudden chest pain, difficulty breathing). A clear follow-up plan with a pulmonologist or primary care physician within 1–2 weeks is crucial. For high-risk patients, such as those with recurrent pneumothorax or underlying lung disease, closer monitoring and potential referral to a thoracic surgeon may be warranted.
Individualized Assessment ensures that discharge criteria are tailored to the patient’s unique circumstances. Factors like age, comorbidities, and social support influence readiness for home recovery. For instance, an elderly patient with COPD may require additional oxygen therapy or home health services, while a young, otherwise healthy individual might be discharged with minimal restrictions. Ultimately, discharge is a collaborative decision involving the healthcare team, patient, and caregivers, prioritizing both medical stability and the patient’s ability to manage recovery outside the hospital setting.
Ambetter In-Network Hospitals: Where to Get Covered Care
You may want to see also
Frequently asked questions
The typical hospital stay for a punctured lung (pneumothorax) ranges from 2 to 5 days, depending on severity, treatment method, and individual recovery.
Yes, a fully collapsed lung often requires a longer stay (3–7 days) compared to a partial pneumothorax (1–3 days), as it may need more intensive treatment like chest tubes or surgery.
Minor cases of pneumothorax may be monitored as an outpatient if stable, but most require at least a short hospital stay (1–2 days) for observation and treatment, such as oxygen therapy or chest tube insertion.













![The Ultimate Hospital Stay Activity Book For Adults: XXL Large Print Relaxing Activities, Memory Games & Brain Puzzles for Patients and Families [1-2 Players!]](https://m.media-amazon.com/images/I/61aUayZHnXL._AC_UY218_.jpg)