Phase 1 at Georgetown Hospital Surgery Center marks the initial stage of the surgical process, focusing on pre-operative preparation and patient assessment. This critical phase ensures that patients are physically and mentally ready for surgery, involving a comprehensive evaluation by the medical team, including surgeons, anesthesiologists, and nurses. During Phase 1, patients undergo necessary tests, such as blood work and imaging, receive detailed instructions about fasting and medication management, and have the opportunity to ask questions to alleviate any concerns. This stage is designed to minimize risks, optimize outcomes, and provide a clear understanding of the surgical journey ahead, setting the foundation for a safe and successful procedure.
| Characteristics | Values |
|---|---|
| Definition | Phase 1 in Georgetown Hospital Surgery Center refers to the initial stage of a surgical procedure, focusing on pre-operative preparation and patient evaluation. |
| Primary Focus | Ensuring patient safety, confirming surgical details, and preparing the patient for surgery. |
| Key Activities | - Patient check-in and registration - Verification of patient identity and consent forms - Review of medical history and allergies - Administration of pre-operative medications (if required) - Placement of IV lines - Final confirmation of surgical site and procedure |
| Personnel Involved | - Nurses - Anesthesiologists - Surgeons - Administrative staff |
| Location | Pre-operative area or holding area within the surgery center. |
| Duration | Typically 30 minutes to 2 hours, depending on the complexity of the case. |
| Patient Involvement | Patients are actively involved in providing information and confirming details. |
| Outcome | Patient is prepared and cleared for the surgical procedure (Phase 2). |
| Importance | Critical for preventing errors, ensuring patient readiness, and aligning the surgical team. |
Explore related products






What You'll Learn
- Pre-Surgery Preparation: Patient evaluation, medical history review, and anesthesia consultation
- Surgical Planning: Procedure details, surgeon briefing, and operating room scheduling
- Patient Admission: Check-in, consent forms, and pre-op instructions
- Anesthesia Administration: Induction process, monitoring, and patient stabilization
- Operating Room Setup: Equipment sterilization, instrument arrangement, and team briefing
![]()
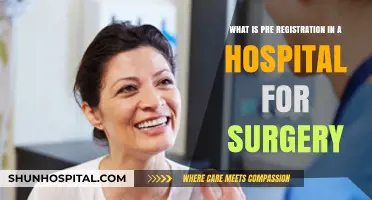
Pre-Surgery Preparation: Patient evaluation, medical history review, and anesthesia consultation
Phase 1 at Georgetown Hospital Surgery Center is a critical juncture where the foundation for a safe and successful surgical experience is laid. This initial stage, often overlooked by patients, involves a meticulous process of pre-surgery preparation, encompassing patient evaluation, medical history review, and anesthesia consultation. Each step is designed to identify potential risks, tailor the surgical plan, and ensure the patient’s readiness for the procedure.
Patient evaluation begins with a comprehensive physical examination, assessing vital signs, organ function, and overall health status. For instance, a 65-year-old patient with hypertension may require additional cardiac monitoring, while a 30-year-old with asthma might need pulmonary function tests. This evaluation often includes laboratory tests such as blood counts, coagulation profiles, and metabolic panels to detect anomalies like anemia, diabetes, or kidney dysfunction. For example, a hemoglobin level below 12 g/dL may necessitate iron supplementation before surgery. Practical tips for patients include fasting as instructed (typically 8–12 hours before surgery) and avoiding medications like aspirin or NSAIDs that can increase bleeding risk.
Medical history review is equally vital, as it uncovers conditions or medications that could complicate surgery. A history of allergies, previous surgeries, or chronic illnesses like diabetes or heart disease must be documented. For instance, a patient on warfarin may need to switch to a low-molecular-weight heparin to reduce bleeding risks. Age-specific considerations are also crucial: pediatric patients may require specialized anesthesia techniques, while elderly patients often need adjustments for polypharmacy. Patients should bring a detailed list of medications, including dosages and frequencies, to this review. A persuasive argument here is that transparency in medical history can prevent life-threatening complications during surgery.
Anesthesia consultation is the final pillar of Phase 1, where the anesthesiologist determines the safest anesthesia type and dosage. This consultation involves discussing the patient’s preferences, such as general anesthesia versus regional blocks, and addressing fears or misconceptions. For example, a patient undergoing knee surgery might opt for a spinal block instead of general anesthesia to reduce postoperative nausea. Dosage calculations are tailored to factors like weight, age, and comorbidities—a 70 kg adult might receive 2–3 mg/kg of propofol for induction, while a child would receive a lower dose. Practical advice includes informing the anesthesiologist about previous reactions to anesthesia and adhering to pre-anesthesia fasting guidelines to minimize aspiration risks.
In comparison to other surgical centers, Georgetown’s Phase 1 stands out for its interdisciplinary approach, where surgeons, anesthesiologists, and nurses collaborate to create a personalized care plan. This phase is not merely administrative but a proactive measure to anticipate challenges and optimize outcomes. The takeaway for patients is clear: active participation in Phase 1 by providing accurate information and following instructions can significantly enhance surgical safety and recovery. By treating this stage as a partnership rather than a formality, patients and providers alike contribute to a seamless surgical journey.
Government-Run Hospitals: Who's in Charge?
You may want to see also
Explore related products






![]()
Surgical Planning: Procedure details, surgeon briefing, and operating room scheduling
Phase 1 in Georgetown Hospital Surgery Center is the critical foundation of surgical success, where meticulous planning transforms a medical concept into a precise, executable procedure. This stage involves a trifecta of essential components: detailed procedure mapping, comprehensive surgeon briefing, and strategic operating room scheduling. Each element is interdependent, ensuring that every surgery is not only technically sound but also logistically feasible and patient-centered.
Consider the procedure details as the blueprint of the surgery. This phase demands an exhaustive documentation of the surgical steps, including the type of anesthesia (e.g., general, regional, or local), estimated duration, and specific instruments required. For instance, a laparoscopic cholecystectomy might necessitate a high-definition camera, harmonic scalpel, and a 5-mm trocar set. Additionally, the surgical team must outline potential complications, such as bleeding or organ injury, and prepare contingency plans. For pediatric patients, age-specific considerations like smaller instrument sizes and adjusted anesthesia dosages (e.g., 1-2 mg/kg of propofol for induction in children under 10) are crucial. This level of detail ensures that the surgical team is fully prepared to address any scenario, minimizing risks and optimizing outcomes.
Surgeon briefing is the bridge between theoretical planning and practical execution. During this step, the lead surgeon convenes with the surgical team to review the procedure details, patient-specific factors, and potential challenges. This briefing is not a one-way communication but an interactive session where team members can raise concerns or suggest improvements. For example, a nurse might point out that a patient’s history of hypertension requires careful monitoring of intraoperative blood pressure, while an anesthesiologist could recommend a lower dose of fentanyl (e.g., 0.5-1 mcg/kg) to avoid respiratory depression. Effective briefing fosters a cohesive team dynamic, ensuring that everyone is aligned on the surgical goals and their individual roles.
Operating room scheduling is the logistical backbone of Phase 1, requiring a delicate balance between efficiency and patient safety. Georgetown Hospital employs a centralized scheduling system that prioritizes urgency, complexity, and resource availability. High-acuity cases, such as emergency trauma surgeries, are slotted first, while elective procedures are scheduled based on surgeon availability and OR capacity. For instance, a total knee replacement might be scheduled in the morning when the surgical team is freshest, while shorter procedures like hernia repairs are grouped in the afternoon to maximize OR utilization. Practical tips include allocating buffer time between cases (e.g., 30 minutes) to account for unexpected delays and ensuring that all necessary equipment is pre-checked to avoid last-minute cancellations.
In conclusion, Phase 1 at Georgetown Hospital Surgery Center is a multifaceted process that demands precision, collaboration, and foresight. By meticulously detailing procedures, conducting thorough surgeon briefings, and optimizing OR scheduling, the center sets the stage for safe, efficient, and successful surgeries. This phase is not merely administrative but a proactive measure to anticipate challenges, streamline workflows, and ultimately deliver the highest standard of patient care.
When to Seek Hospital Care for Thoracic Back Pain: A Guide
You may want to see also
Explore related products
![Moon Phase - Phase 1 [DVD]](https://m.media-amazon.com/images/I/61wdMbPhccL._AC_UL320_.jpg)




![]()
Patient Admission: Check-in, consent forms, and pre-op instructions
Phase 1 at Georgetown Hospital Surgery Center begins with patient admission, a critical step that sets the tone for the entire surgical experience. This process is meticulously designed to ensure patient safety, streamline operations, and address any concerns before the procedure. Upon arrival, patients are greeted by a dedicated admissions team who verifies their identity, confirms the scheduled surgery, and collects essential demographic and insurance information. Efficiency here is key, as delays can ripple through the day’s schedule, affecting not only the patient but also subsequent cases.
Check-in is more than a bureaucratic formality; it’s the first line of defense against errors. Patients are required to present a valid photo ID and insurance card, ensuring accuracy in billing and medical records. For minors or incapacitated adults, legal guardians must provide additional documentation, such as custody papers or power of attorney. This step also includes a brief health screening—questions about recent illnesses, medication changes, or allergies—to flag potential risks that could impact the surgery. Pro tip: Arrive 15 minutes early to allow buffer time for unexpected delays, like parking or last-minute document retrieval.
Consent forms are the cornerstone of ethical medical practice, and Georgetown Hospital takes this seriously. Patients are presented with detailed documents outlining the procedure, its risks, benefits, and alternatives. Staff members are trained to explain these forms in plain language, ensuring patients understand what they’re agreeing to. For complex surgeries, this may involve a consultation with the surgeon or anesthesiologist. A common oversight? Forgetting reading glasses. Patients over 40 should bring them to review fine print comfortably. Once signed, these forms are scanned into the electronic health record, creating a permanent, accessible record.
Pre-op instructions are the final piece of the admission puzzle, and adherence is non-negotiable. Patients receive a tailored checklist based on their procedure and health status. Common directives include fasting guidelines (e.g., no food or drink after midnight for morning surgeries), medication adjustments (e.g., holding blood thinners 48 hours prior), and hygiene protocols (e.g., showering with antibacterial soap the night before). For pediatric patients, parents are advised to bring a comfort item, like a stuffed animal, to ease anxiety. Non-compliance can lead to cancellations—a 2022 study found that 12% of surgical delays were due to patients ignoring pre-op instructions.
In conclusion, Phase 1 at Georgetown Hospital Surgery Center is a multi-layered process that prioritizes safety, clarity, and efficiency. By mastering check-in, consent, and pre-op protocols, patients not only contribute to their own care but also help maintain the center’s reputation for excellence. Remember: Preparation is as vital as the surgery itself. Follow instructions meticulously, ask questions when in doubt, and arrive ready to participate in your care journey.
In-Person Hospital Job Applications: A Step-by-Step Guide to Success
You may want to see also
Explore related products






![]()
Anesthesia Administration: Induction process, monitoring, and patient stabilization
Phase 1 in Georgetown Hospital Surgery Center is the critical pre-operative phase where anesthesia administration begins, setting the stage for a safe and controlled surgical environment. This phase is a meticulous process that demands precision, vigilance, and a deep understanding of patient physiology. The induction process is the first step, where the anesthesiologist administers medications to achieve a state of unconsciousness and analgesia, ensuring the patient is comfortably transitioned into surgery.
Induction Process: A Delicate Balance
Induction typically starts with pre-oxygenation, where the patient breathes 100% oxygen for 3–5 minutes to saturate the lungs, providing a reserve in case of apnea during drug administration. For adults, common induction agents include propofol (1.5–2.5 mg/kg IV) or etomidate (0.1–0.3 mg/kg IV), chosen based on the patient’s medical history and the surgery’s requirements. Pediatric patients often receive sevoflurane via inhalation due to its rapid onset and smooth induction. Opioids like fentanyl (1–2 mcg/kg IV) or remifentanil may be added for analgesia, while neuromuscular blocking agents such as rocuronium (0.6–1.0 mg/kg IV) are used to facilitate intubation. The goal is to achieve unconsciousness within 10–30 seconds of drug administration, ensuring the patient is unaware and pain-free.
Monitoring: The Eyes and Ears of Anesthesia
Once induction is complete, continuous monitoring becomes paramount. Standard monitors include electrocardiography (ECG), pulse oximetry (SpO2), non-invasive blood pressure (NIBP), and end-tidal CO2 (EtCO2) to track ventilation. For high-risk patients or complex surgeries, invasive monitoring such as arterial lines or central venous catheters may be employed. Anesthesiologists must remain vigilant for signs of hypotension, hypoxia, or hypercarbia, adjusting the anesthetic plan in real-time. For instance, a sudden drop in blood pressure may require a fluid bolus or vasopressor, while inadequate ventilation demands immediate intervention to prevent respiratory acidosis.
Patient Stabilization: The Bridge to Surgery
Stabilization focuses on maintaining hemodynamic and respiratory stability while ensuring the patient’s airway is secure. After intubation, the anesthesiologist confirms proper tube placement using capnography and chest auscultation. Mechanical ventilation is initiated, targeting a tidal volume of 6–8 mL/kg and a respiratory rate of 10–14 breaths per minute to maintain normocarbia. Temperature management is also critical, as anesthesia can impair thermoregulation; warming blankets or fluid warmers are often used to prevent hypothermia. Practical tips include pre-warming IV fluids and using forced air warming devices to maintain core temperature.
Cautions and Considerations
While induction and stabilization are routine, complications can arise. For example, propofol may cause hypotension in hypovolemic patients, necessitating careful titration. Pediatric patients are particularly sensitive to respiratory depression, requiring lower doses and closer monitoring. Allergic reactions to neuromuscular blocking agents, though rare, can be life-threatening and demand immediate recognition and treatment. Anesthesiologists must also consider the patient’s comorbidities, such as asthma or heart disease, which may alter drug selection and dosing.
Phase 1 in Georgetown Hospital Surgery Center is a complex yet systematic process that lays the groundwork for a safe surgical experience. From the precise induction of anesthesia to vigilant monitoring and stabilization, every step is designed to protect the patient’s well-being. By adhering to evidence-based protocols and remaining adaptable to individual patient needs, anesthesia providers ensure a seamless transition from the pre-operative phase to the operating room, setting the stage for successful surgical outcomes.
Johns Hopkins Hospital: A Nonprofit Healthcare Powerhouse
You may want to see also
Explore related products


![Marvel Cinematic Universe: Phase One Ultimate Collector's Limited Edition Briefcase Legacy [3D + Blu-Ray, Region Free]](https://m.media-amazon.com/images/I/71jqMDjuWmL._AC_UL320_.jpg)

![Moon Phase - Phase 1 [Import anglais]](https://m.media-amazon.com/images/I/81i2BOMRJcL._AC_UL320_.jpg)

![]()
Operating Room Setup: Equipment sterilization, instrument arrangement, and team briefing
In the critical first phase of surgery at Georgetown Hospital Surgery Center, the operating room setup is a meticulously orchestrated process that ensures patient safety and surgical success. Equipment sterilization stands as the cornerstone of this phase, employing advanced techniques such as autoclaving at 134°C for 18 minutes to eliminate all microorganisms, including spores. This process is not just a regulatory requirement but a moral imperative, as a single unsterile instrument can lead to catastrophic postoperative infections. For instance, surgical site infections (SSIs) account for 22% of all healthcare-associated infections, underscoring the gravity of this step. Sterilization protocols are rigorously verified using biological and chemical indicators, ensuring that every clamp, scalpel, and tray meets the highest standards of asepsis.
Instrument arrangement follows sterilization, transforming the operating room into a functional workspace tailored to the specific procedure. This is not merely about placing tools on a tray but involves strategic organization to optimize efficiency and minimize disruptions. For example, in a laparoscopic cholecystectomy, instruments like the grasper, scissors, and clip applier are arranged in a clockwise pattern around the surgeon’s dominant hand, reducing reach time by up to 30%. This ergonomic layout is critical, as studies show that surgeons who experience fewer instrument-related delays complete procedures 15% faster on average. Each instrument is checked against a standardized checklist, ensuring nothing is missing or misplaced, a practice that has reduced procedural delays by 20% at Georgetown.
Team briefing is the final, yet equally vital, component of Phase 1, serving as the linchpin for communication and coordination. Conducted immediately before the patient enters the OR, this briefing follows the WHO Surgical Safety Checklist, a 19-item protocol that includes verification of patient identity, procedure site, and consent. Research indicates that teams that consistently complete this briefing experience a 47% reduction in surgical complications. During the briefing, roles are clarified, potential risks are discussed, and contingency plans are outlined. For instance, in a complex cardiac case, the anesthesiologist might highlight the need for rapid blood availability, while the surgeon emphasizes the critical timing of graft placement. This proactive dialogue fosters a shared mental model among the team, enhancing situational awareness and responsiveness.
While each of these elements—sterilization, arrangement, and briefing—is distinct, their synergy defines the success of Phase 1. A sterile instrument is useless if it cannot be located quickly, and the most organized OR becomes chaotic without clear communication. Georgetown’s approach exemplifies this integration, where sterilization logs are reviewed during the team briefing, and instrument trays are arranged based on the surgeon’s preferences discussed in pre-op meetings. This holistic strategy not only streamlines the surgical workflow but also reinforces a culture of accountability and precision, hallmarks of a world-class surgical center. By mastering these components, Georgetown ensures that Phase 1 sets the stage for a seamless and safe surgical experience.
Government Hospitals and Public Service Loan Forgiveness: Eligibility Explained
You may want to see also
Frequently asked questions
Phase 1 in Georgetown Hospital Surgery Center refers to the initial stage of the surgical process, which typically includes pre-operative preparation, patient evaluation, and admission procedures.
During Phase 1, patients undergo pre-operative assessments, such as medical history reviews, physical exams, and necessary lab tests. They also receive instructions for surgery day and complete any required paperwork.
The duration of Phase 1 varies but generally takes a few hours to a day, depending on the complexity of the surgery and the patient’s specific needs.
Yes, Phase 1 is a mandatory step for all surgical procedures at Georgetown Hospital Surgery Center to ensure patient safety, proper preparation, and adherence to medical protocols.