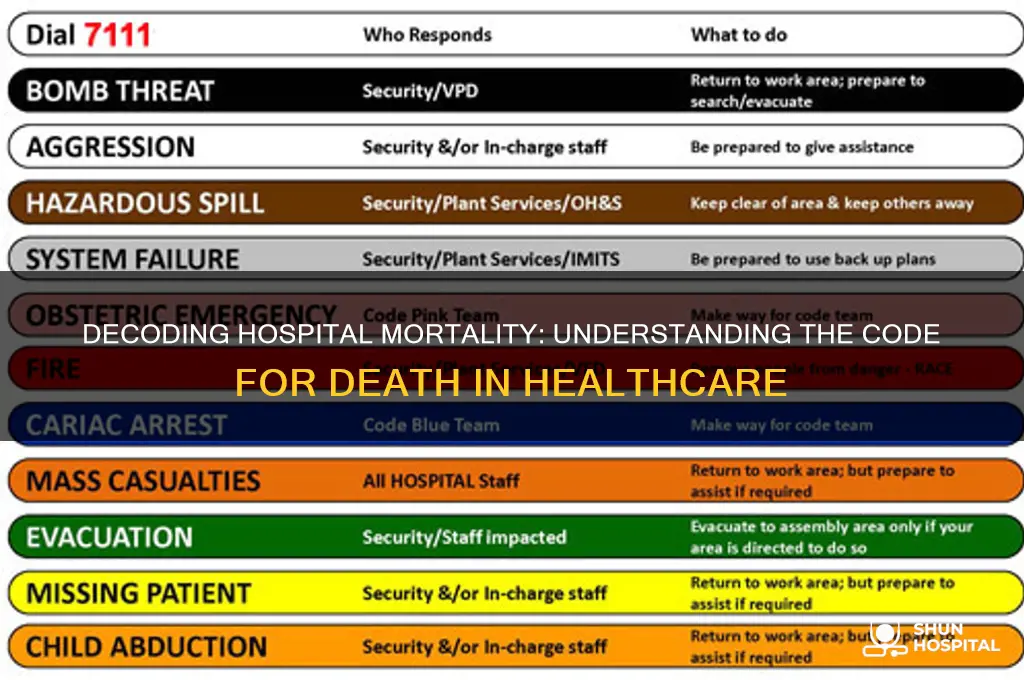
The term code for death in a hospital often refers to specific protocols or codes used by medical staff to discreetly communicate the occurrence of a patient's death without alarming other patients or visitors. One of the most commonly recognized codes is Code 99, though its usage varies by institution and region. These codes are part of a broader system designed to maintain a calm and professional environment while ensuring that appropriate procedures, such as notifying family members and initiating post-mortem care, are followed. Understanding these codes highlights the balance hospitals strive to achieve between compassion and operational efficiency in sensitive situations.
Explore related products






What You'll Learn
- ICD-10 Codes for Death: Understanding the specific ICD-10 codes used to document death in medical records
- Death Certification Process: Steps and protocols for certifying death in a hospital setting
- Cause of Death Coding: Guidelines for accurately coding the underlying cause of death in hospitals
- Death Notification Procedures: How hospitals inform families and handle death notifications professionally
- Legal and Ethical Aspects: Legal requirements and ethical considerations when documenting death in healthcare
![]()
ICD-10 Codes for Death: Understanding the specific ICD-10 codes used to document death in medical records
In the realm of medical coding, the International Classification of Diseases, 10th Revision (ICD-10), provides a comprehensive framework for documenting various health conditions, including death. When a patient passes away in a hospital setting, accurate coding is crucial for statistical analysis, reimbursement, and quality improvement initiatives. The ICD-10 codes for death are not merely administrative placeholders; they convey essential information about the circumstances and underlying causes of mortality. Understanding these codes is vital for healthcare professionals, coders, and administrators to ensure precise documentation and compliance with regulatory standards.
The ICD-10 system categorizes death codes under Chapter XX: External causes of morbidity, with specific subcategories for different scenarios. For instance, R99 is the code for "Other ill-defined and unknown causes of mortality," often used when the exact cause of death is uncertain. This code serves as a temporary placeholder until further investigation or autopsy results provide more definitive information. In contrast, Z00-Z99 codes are used for factors influencing health status and contact with health services, which may include encounters related to administrative or legal aspects of death. It is essential to differentiate between these categories to avoid misclassification, which can skew data and impact healthcare decision-making.
One critical aspect of ICD-10 death coding is the distinction between the manner of death and the cause of death. The manner of death refers to whether the death was natural, accidental, homicidal, suicidal, or undetermined, while the cause of death identifies the disease, injury, or complication directly leading to mortality. For example, a patient who dies from a heart attack (I21, Acute myocardial infarction) would have this condition listed as the cause of death. If the heart attack occurred during a motor vehicle accident (V00-V99), the manner of death would be classified as accidental. Properly linking these codes ensures a comprehensive and accurate representation of the circumstances surrounding the patient’s demise.
Practical tips for coding death in ICD-10 include reviewing all available documentation, such as physician notes, autopsy reports, and death certificates, to identify the most precise codes. Coders should also be aware of sequencing rules, which dictate the order of codes based on their relevance to the patient’s case. For example, the underlying cause of death should be listed first, followed by contributing conditions or complications. Additionally, coders must stay updated on ICD-10 revisions and guidelines, as changes may affect code selection and reporting requirements. By adhering to these best practices, healthcare organizations can maintain data integrity and support initiatives aimed at improving patient outcomes and public health.
In conclusion, ICD-10 codes for death are a specialized yet critical component of medical documentation. They require careful consideration of the patient’s clinical history, the circumstances of death, and applicable coding guidelines. Mastery of these codes not only ensures compliance with regulatory standards but also contributes to a deeper understanding of mortality trends and healthcare delivery. As the healthcare landscape continues to evolve, the accurate use of ICD-10 death codes will remain an indispensable tool for professionals dedicated to advancing patient care and public health.
Hospital Water Birth Guide: Steps, Benefits, and Preparation Tips
You may want to see also
Explore related products





![]()
Death Certification Process: Steps and protocols for certifying death in a hospital setting
In hospital settings, the term "code" often refers to emergency protocols, but when it comes to death, there is no universal "code for death." Instead, hospitals follow a structured Death Certification Process to ensure accuracy, compliance, and respect for the deceased and their families. This process involves multiple steps, each governed by strict protocols to maintain legal and ethical standards.
The first step in the death certification process is pronouncing death, which must be done by a qualified medical professional, typically a physician. This involves verifying the absence of vital signs—such as heartbeat, breathing, and pupil response—using clinical judgment and, in some cases, diagnostic tools like electrocardiograms (ECGs) or ultrasound. Once death is confirmed, the time of death is recorded to the nearest minute, a critical detail for legal and administrative purposes. Practical tip: Ensure all monitoring equipment is functioning correctly before pronouncing death to avoid errors.
Following the pronouncement, the completion of the death certificate is initiated. This document is a legal record that requires precise information, including the cause and manner of death. Physicians must adhere to guidelines from the World Health Organization (WHO) or local health authorities, such as the International Classification of Diseases (ICD) codes, to accurately report the underlying cause of death. For example, if a patient dies from metastatic lung cancer, the physician would specify "malignant neoplasm of bronchus or lung (C34)" as the primary cause. Caution: Inaccurate or incomplete certification can lead to legal complications or delays in funeral arrangements.
The next step involves notification and documentation. Hospital staff must inform the deceased’s next of kin or designated representative, offering condolences and providing clear, compassionate communication. Simultaneously, the death is logged in the hospital’s electronic health record (EHR) system, and relevant paperwork, such as organ donation consent forms (if applicable), is processed. Comparative analysis: Some hospitals use automated systems to streamline this step, reducing the risk of human error and ensuring timely notifications.
Finally, the transfer of the body to the morgue or funeral home is coordinated. This step requires adherence to infection control protocols, such as placing the body in a sealed bag and ensuring proper labeling. Hospitals often collaborate with external agencies, like coroners or medical examiners, if the death is unexpected, violent, or occurs under suspicious circumstances. Takeaway: A well-executed death certification process not only fulfills legal requirements but also provides closure for families and maintains the integrity of healthcare systems.
Exploring the UK NHS: Total Number of Hospitals Revealed
You may want to see also
Explore related products





![]()
Cause of Death Coding: Guidelines for accurately coding the underlying cause of death in hospitals
Accurate coding of the underlying cause of death in hospitals is critical for public health surveillance, epidemiological research, and healthcare policy. The International Classification of Diseases (ICD) provides a standardized framework for this purpose, ensuring consistency across institutions and countries. However, determining the correct code requires a nuanced understanding of the patient’s clinical history, the sequence of events leading to death, and the rules governing cause-of-death selection. Misclassification can skew mortality statistics, impacting resource allocation and disease prevention strategies.
The process begins with identifying the immediate cause of death—the final disease or condition directly leading to the fatal outcome. For example, if a patient dies from septic shock, sepsis is the immediate cause. However, coding does not stop here. Clinicians must trace back to the underlying cause, the disease or injury that initiated the chain of events. In the sepsis example, the underlying cause might be pneumonia or a urinary tract infection. This step demands careful review of medical records, including lab results, imaging, and physician notes, to establish a clear etiological link.
One common challenge is distinguishing between contributing conditions and the underlying cause. For instance, diabetes mellitus may be listed as a comorbidity in a patient who dies from a myocardial infarction. While diabetes can exacerbate cardiovascular risk, it is not the underlying cause unless it directly contributed to the fatal event, such as through diabetic ketoacidosis. Coders must apply ICD guidelines rigorously, such as Rule 1 (select the underlying cause), which emphasizes choosing the disease or injury that initiated the morbid sequence. Training and regular audits are essential to minimize errors in this judgment-intensive process.
Pediatric and maternal deaths require special attention due to their unique coding considerations. For infants, conditions like low birth weight or congenital anomalies often underlie deaths, necessitating precise documentation of prenatal and postnatal factors. Maternal deaths, though rare, demand scrutiny of pregnancy-related complications, such as postpartum hemorrhage or pre-eclampsia. Coders should reference the ICD’s Maternal Mortality chapter and collaborate with obstetricians to ensure accuracy. Age-specific guidelines, such as those for perinatal deaths (ICD-PM), further refine coding in these populations.
Finally, technology can enhance the accuracy and efficiency of cause-of-death coding. Electronic health records (EHRs) with built-in decision support tools can flag inconsistencies or missing data, prompting coders to revisit the case. Natural language processing (NLP) algorithms can extract relevant information from unstructured text, such as physician notes, reducing manual effort. However, these tools are not infallible and should complement, not replace, human judgment. Regular updates to ICD guidelines and ongoing education for coding staff are equally vital to maintain the integrity of mortality data.
Nemours Hospital at Lake Nona: Location and Directions Guide
You may want to see also
Explore related products




![]()
Death Notification Procedures: How hospitals inform families and handle death notifications professionally
In hospitals, the code for death is often referred to as "Code Blue" when a patient is in cardiac or respiratory arrest, but the actual declaration of death follows specific protocols. Once a patient has passed, medical professionals use the term "expired" or document the time of death with precision. However, the most critical aspect of this process is what comes next: notifying the family. Death notification procedures are a delicate, structured practice designed to deliver the news with compassion and professionalism while addressing the emotional and logistical needs of the bereaved.
The first step in death notification is assigning the task to a trained individual, typically a physician or senior nurse, who can provide clear, accurate information. This person should be prepared to answer questions about the circumstances of the death, though medical jargon should be avoided. The notification should occur in a private, quiet space to ensure confidentiality and allow the family to grieve without interruption. Hospitals often offer a designated bereavement room for this purpose, equipped with tissues, water, and a calm atmosphere. If the family is not present, the notifier should contact them promptly via phone, ensuring they understand the urgency without revealing the news outright until a private conversation can be arranged.
A key aspect of professional death notification is the use of clear, empathetic language. Phrases like "I’m sorry for your loss" or "Your loved one has passed away" are direct yet compassionate. Avoid euphemisms such as "They’ve gone to sleep," which can confuse or delay acceptance of the reality. The notifier should also offer practical next steps, such as arranging to see the deceased, contacting a funeral home, or accessing grief counseling services. Hospitals often provide a checklist or pamphlet to guide families through immediate decisions, reducing their sense of overwhelm.
Cultural and religious considerations play a significant role in death notification procedures. For example, some families may wish to perform rituals immediately, while others may need time to gather extended relatives. Hospitals should train staff to be sensitive to these differences, asking families about their preferences rather than making assumptions. In cases where the death was sudden or traumatic, involving a social worker or chaplain can provide additional emotional support. Documentation is also crucial; the notifier should record the time, method, and recipient of the notification, as well as any immediate requests from the family.
Finally, hospitals must prepare staff for the emotional toll of delivering death notifications. Regular training and debriefing sessions can help healthcare providers process their own feelings and maintain professionalism. Role-playing scenarios, for instance, can build confidence in handling difficult conversations. Hospitals should also encourage self-care practices, such as taking breaks after notifications or accessing employee assistance programs. By prioritizing both the needs of the family and the well-being of staff, hospitals can ensure that death notifications are handled with the utmost care and respect.
Attendance Allowance: Hospital Stay Impact
You may want to see also
Explore related products






![]()
Legal and Ethical Aspects: Legal requirements and ethical considerations when documenting death in healthcare
Documenting death in healthcare is not merely a procedural task; it is a legally binding act with profound ethical implications. In the United States, the legal requirement for death certification is governed by the Model Death Certificate, which mandates specific details such as the immediate cause of death, antecedent causes, and contributing conditions. Physicians must complete this within 48 hours of death, ensuring accuracy to avoid legal repercussions, including potential malpractice claims or investigations by medical boards. In the UK, the Medical Certificate of Cause of Death (MCCD) follows a similar rigor, requiring verification by a registered medical practitioner. These documents are not just administrative forms—they are critical for public health data, estate settlements, and insurance claims, making precision non-negotiable.
Ethically, the documentation of death demands sensitivity and respect for the deceased and their family. While legal requirements focus on factual accuracy, ethical considerations extend to the manner in which the process is handled. For instance, disclosing the cause of death to family members requires balancing transparency with compassion, particularly in cases involving stigmatized conditions like suicide or overdose. Healthcare providers must navigate this delicate terrain, ensuring that the family’s right to know is respected without causing undue distress. This ethical duty is further complicated when the cause of death is uncertain or controversial, necessitating clear communication and, if necessary, involvement of a medical examiner or coroner.
A critical ethical dilemma arises when the cause of death is unclear or disputed. In such cases, healthcare providers must resist the temptation to speculate or provide incomplete information. Instead, they should initiate a referral to a coroner or medical examiner, as required by law in many jurisdictions. This step not only ensures compliance with legal standards but also upholds ethical integrity by prioritizing accuracy over expediency. For example, in cases of sudden infant death syndrome (SIDS), thorough documentation and referral are essential to provide closure for families and contribute to public health research.
Practical tips for healthcare professionals include maintaining detailed patient records leading up to death, as these can serve as critical evidence in legal proceedings. For instance, documenting the administration of end-of-life medications, such as morphine (commonly given in doses of 2.5–5 mg every 1–4 hours for pain management), is essential. Additionally, involving a multidisciplinary team, including nurses and social workers, can provide a more comprehensive account of the patient’s final days, reducing the risk of oversight. Finally, staying updated on local and national guidelines, such as the CDC’s National Vital Statistics System, ensures that documentation practices remain current and compliant.
In conclusion, the legal and ethical aspects of documenting death in healthcare require a meticulous approach that balances factual accuracy with human compassion. By adhering to legal mandates, navigating ethical dilemmas with care, and employing practical strategies, healthcare providers can fulfill their professional obligations while honoring the dignity of the deceased and their families. This dual responsibility underscores the gravity of the task and the need for ongoing education and reflection in this critical area of practice.
Hospital Refuses Treatment? Know Your Rights and Next Steps
You may want to see also
Frequently asked questions
There is no universal "code" for death in hospitals, but the term "Code Blue" is often used to indicate a cardiac arrest or a patient in immediate need of resuscitation. Death is typically documented in medical records with specific terminology, such as "expired" or "time of death."
Hospital staff do not use secret codes to announce a patient’s death. Instead, clear and professional communication is used, often involving phrases like "the patient has passed away" or "time of death has been noted."
"Code 99" is not a standard medical code. In some facilities, it may be used informally to indicate a security or behavioral issue, but it is not related to death. Always refer to your hospital’s specific protocols for accurate information.



























