Navigating the complexities of medical billing requires a clear understanding of the appropriate claim forms for different healthcare services. When it comes to inpatient hospital claims, selecting the correct form is crucial to ensure accurate reimbursement and compliance with regulatory requirements. The primary form used for inpatient hospital claims in the United States is the UB-04, also known as the CMS-1450, which is specifically designed to capture detailed information about the patient's stay, including diagnoses, procedures, and charges. Using the wrong form can lead to claim denials, delays in payment, and potential audits, making it essential for healthcare providers to familiarize themselves with the UB-04 and its proper usage.
Explore related products




What You'll Learn
![]()
Understanding Claim Form Types
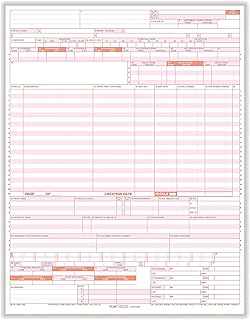
Navigating the labyrinth of healthcare claims begins with identifying the correct form, a task often fraught with confusion. For inpatient hospital claims, the CMS-1450 (formerly UB-04) is the standard form used across the United States. This form is specifically designed for institutional providers, including hospitals, to bill Medicare, Medicaid, and private insurers. Its structured format ensures uniformity in reporting patient demographics, diagnosis codes, and procedural details, reducing errors and streamlining reimbursement processes.
While the CMS-1450 is the go-to form for inpatient claims, understanding its components is equally crucial. The form is divided into sections that require precise information, such as revenue codes, which categorize services like room and board or operating room usage. For instance, revenue code 0210 is used for inpatient hospital services, excluding physician fees. Accurate completion of these fields is essential, as errors can lead to claim denials or delays. For example, misclassifying a service under the wrong revenue code could result in a rejected claim, necessitating a time-consuming resubmission.
A common pitfall in inpatient claim submissions is the misuse of condition codes, which provide additional information about the patient’s stay. For instance, condition code 42 indicates that a patient was transferred to another acute care hospital. Failing to include this code when applicable can complicate reimbursement, as it affects payment calculations under Medicare’s transfer policy. Similarly, occurrence codes (e.g., code 09 for a late bill) must be used judiciously to avoid misinterpretation by payers.
To ensure accuracy, hospitals often employ specialized billing software that auto-populates fields based on patient data. However, manual verification remains critical. For example, cross-checking ICD-10-CM diagnosis codes against the patient’s medical record can prevent discrepancies. A patient admitted for pneumonia (code J18.9) should not be billed under a code for asthma (J45.9), as this mismatch would trigger audits or denials. Regular staff training on form updates, such as annual changes to revenue codes or billing guidelines, further minimizes errors.
In conclusion, mastering the CMS-1450 form is non-negotiable for efficient inpatient claim processing. By understanding its structure, codes, and common pitfalls, healthcare providers can optimize reimbursement workflows. Practical steps include investing in training, leveraging technology for accuracy, and maintaining vigilance in form completion. After all, in the high-stakes world of healthcare billing, the right form—filled out correctly—is the first step to securing rightful payments.
Hope Hicks: Is She Still Hospitalized?
You may want to see also
Explore related products




![]()
Key Fields for Inpatient Claims
Inpatient hospital claims hinge on precise data entry in specific fields to ensure accurate reimbursement and compliance. The Patient Information section is non-negotiable, requiring the full legal name, date of birth, and unique identifier (e.g., Social Security Number or Member ID). Errors here can lead to claim denials or delays, as insurers cross-reference this data with their records. For pediatric claims, include the parent or guardian’s details, and verify age-specific coverage limits, such as extended neonatal care for infants under 28 days. Pro tip: Double-check the patient’s address and contact information, as discrepancies can trigger fraud alerts.
The Admission and Discharge Dates fields are critical for determining the length of stay and corresponding reimbursement rates. Insurers often use these dates to calculate per diem rates or bundled payments, particularly for Medicare Severity-DRGs (MS-DRGs). For example, a stay exceeding 7 days may trigger a higher reimbursement tier, but only if the dates are accurately recorded. Caution: Avoid backdating or future-dating these fields, as this raises red flags for auditors. If the discharge date is uncertain at the time of submission, use the anticipated date and submit a corrected claim later.
Diagnosis and Procedure Codes form the backbone of inpatient claims, directly impacting reimbursement and medical necessity reviews. ICD-10-CM diagnosis codes must align with CPT or HCPCS procedure codes to demonstrate clinical appropriateness. For instance, a claim for a cardiac catheterization (CPT 93454) should include a primary diagnosis like acute myocardial infarction (I21.01). Missing or mismatched codes result in denials or downcoding. Practical tip: Use encoder software to validate code pairs and ensure compliance with NCCI (National Correct Coding Initiative) guidelines.
The Revenue and Charge Fields require meticulous attention to detail, as they translate services into billable amounts. Each line item must include a revenue code (e.g., 0210 for pharmacy) and a corresponding charge, with modifiers where applicable. For example, a claim for a semi-private room (revenue code 0110) should reflect the daily rate multiplied by the length of stay. Errors in these fields can lead to underpayment or overpayment, both of which require time-consuming adjustments. Comparative analysis: Outpatient claims often use HCPCS codes instead of revenue codes, so ensure your staff understands the distinction.
Lastly, the Provider and Facility Information fields are essential for linking the claim to the correct entity. Include the rendering provider’s NPI (National Provider Identifier) and the facility’s CMS Certification Number (CCN) for Medicare claims. For teaching hospitals, add the GME (Graduate Medical Education) swing bed indicator if applicable. Persuasive note: Accurate provider data not only ensures payment but also protects against potential fraud allegations, as insurers scrutinize these fields closely. Regularly update this information to reflect staffing or facility changes.
Hospital Patient Care Technicians: Their Vital Role Explained
You may want to see also
Explore related products


$38.95




![]()
ICD & CPT Code Requirements
Accurate coding is the backbone of successful inpatient hospital claims. ICD (International Classification of Diseases) and CPT (Current Procedural Terminology) codes are the universal language of medical billing, translating complex diagnoses and procedures into standardized data for insurance companies. Missing, incorrect, or incomplete codes can lead to claim denials, delayed payments, and even audits.
ICD codes, maintained by the World Health Organization, classify diseases, disorders, injuries, and health conditions. For inpatient claims, ICD-10-CM (Clinical Modification) codes are used. These alphanumeric codes provide granularity, capturing the specific diagnosis, laterality (left vs. right), and episode of care. For example, a patient admitted for a fractured left femur would require a code specifying the type of fracture, open or closed, and whether it's an initial encounter for treatment.
CPT codes, developed by the American Medical Association, describe medical procedures and services. Inpatient claims often involve a combination of evaluation and management (E/M) codes, surgical codes, and codes for ancillary services like imaging or laboratory tests. Selecting the correct CPT code requires a thorough understanding of the procedure performed, including its complexity, duration, and the physician's involvement. For instance, a laparoscopic cholecystectomy (gallbladder removal) has a different CPT code than an open cholecystectomy, reflecting the less invasive nature of the laparoscopic approach.
While ICD and CPT codes are distinct, they are interconnected. ICD codes justify the medical necessity of the procedures billed with CPT codes. A claim for a complex surgical procedure without a corresponding ICD code indicating a severe condition is likely to be denied. Think of ICD codes as the "why" and CPT codes as the "what" of a claim. Both are essential for painting a complete picture of the patient's encounter.
Regularly updating your knowledge of ICD and CPT codes is crucial. Both coding systems undergo annual revisions, reflecting advancements in medical knowledge and technology. Utilizing reputable coding resources, attending workshops, and subscribing to industry publications can help ensure you're using the most current and accurate codes. Remember, precision in coding is not just about compliance; it's about ensuring fair reimbursement for the services provided and ultimately, the financial health of your healthcare organization.
Utah Valley Hospital Registration Location: A Quick Guide for Visitors
You may want to see also
Explore related products





![]()
Patient Information Accuracy Tips
Accurate patient information is the cornerstone of successful inpatient hospital claims. Errors in demographics, insurance details, or treatment codes can lead to claim denials, delayed reimbursements, and administrative headaches. A single misplaced digit in a patient's date of birth or an outdated insurance policy number can trigger a cascade of issues, costing both time and money.
Consider this scenario: A 45-year-old patient with diabetes is admitted for a complication. Their insurance plan requires prior authorization for certain medications, but the hospital’s records list an incorrect policy effective date. This oversight delays approval, prolonging the patient’s treatment and increasing costs. To avoid such pitfalls, verify patient demographics (name, DOB, address) and insurance details (policy number, group ID, effective dates) at every touchpoint—admission, discharge, and during transfers between departments.
Training staff to double-check information is critical. Implement a system where two staff members independently verify key data fields before submission. For instance, one nurse confirms the patient’s DOB and insurance provider, while another cross-references it with the electronic health record (EHR). This redundancy reduces human error and ensures consistency. Additionally, leverage technology like barcode scanners for patient identification and automated alerts for expired insurance policies to streamline accuracy.
Another practical tip is to standardize data entry formats. For example, require dates in MM/DD/YYYY format and phone numbers in (XXX) XXX-XXXX. This minimizes confusion and ensures uniformity across all claims. Encourage patients to update their information during each visit, especially if they’ve recently changed insurers or moved. Providing a simple, user-friendly form at check-in can facilitate this process.
Finally, audit claims periodically to identify recurring errors. Analyze denial patterns to pinpoint problem areas—whether it’s incorrect diagnosis codes, missing modifiers, or incomplete physician signatures. Use these insights to refine training programs and update internal protocols. By prioritizing patient information accuracy, hospitals can improve claim acceptance rates, reduce administrative burdens, and focus on what truly matters: delivering quality care.
Travel Guide: Kolkata to LV Prasad Eye Hospital Hyderabad Route
You may want to see also
Explore related products






![]()
Common Errors to Avoid
Submitting inpatient hospital claims requires precision, yet errors frequently derail reimbursement. One common mistake involves using outdated claim forms. CMS updates the UB-04 form annually, yet providers often overlook these revisions, leading to rejections. For instance, the 2023 version introduced new fields for telehealth modifiers, which, if omitted, can trigger denials. Always verify the form’s revision date against the current year’s requirements before submission.
Another frequent error is incomplete or inconsistent patient information. Discrepancies between the patient’s name, date of birth, or policy number on the claim form and the insurer’s records result in immediate rejections. For example, a hyphenated last name missing a hyphen or an incorrect digit in the policy number can halt processing. Cross-reference the claim data with the patient’s ID and insurance card to ensure accuracy.
Coding errors also plague inpatient claims, particularly with diagnosis and procedure codes. Using unspecified ICD-10 codes or failing to link diagnoses to procedures triggers audits or denials. For instance, a claim for a cholecystectomy without a corresponding diagnosis code for cholelithiasis raises red flags. Utilize coding tools or consult a certified coder to validate accuracy, especially for complex cases like sepsis or trauma.
Finally, neglecting to include required documentation attachments delays claims. Insurers often demand medical records, operative reports, or discharge summaries to substantiate inpatient stays. Failing to attach these documents or submitting incomplete records results in requests for additional information, prolonging reimbursement. Organize and attach all necessary files systematically, ensuring they align with the claim’s billed services.
Avoiding these errors streamlines the claims process, reducing denials and accelerating payment. Regularly train staff on form updates, implement double-checks for patient data, invest in coding education, and standardize documentation submission. These steps transform a reactive approach into a proactive strategy, safeguarding revenue and minimizing administrative burdens.
Quickly Deliver Toys to Philadelphia Children’s Hospital: A Step-by-Step Guide
You may want to see also
Frequently asked questions
The correct claim form for inpatient hospital claims is the CMS-1500 for professional services or the UB-04 (CMS-1450) for institutional claims. The UB-04 is specifically designed for hospitals and inpatient facilities.
No, the CMS-1500 form is typically used for outpatient or professional services, not inpatient hospital claims. For inpatient claims, the UB-04 form is the appropriate choice.
The UB-04 form can be obtained from the NUCC (National Uniform Claim Committee) or through medical supply vendors. Ensure you are using the most current version to avoid claim rejections.